
Abstract
Objectives
To evaluate the long-term outcomes of in-office bleaching with violet LED light (LED) alone or combined with carbamide (CP) or hydrogen (HP) peroxides.
Methods
Volunteers of a previous short-term study were recalled for 6- and 12-month follow-ups, according to the following interventions (n = 18/group): LED, CP, LED/CP, HP, and LED/HP. The objective color (ΔEab, ΔE00) and whiteness index (ΔWID) changes were calculated applying the CIELab coordinates’ values obtained using a spectrophotometer. A visual shade guide determined the tooth’s subjective color change (ΔSGU). Data were submitted to one-way ANOVA or Welch’s ANOVA, following appropriate post hoc tests (α = 5%).
Results
The LED and CP groups exhibited the lowest ΔEab, ΔE00, and ΔSGU (p < 0.05), but the LED group displayed a significantly lower ΔWID. After 12 months, the LED/CP group presented a higher ΔEab and ΔE00 than the CP group (p < 0.05). ΔEab, ΔE00, ΔSGU, or ΔWID means did not differ statistically between the LED/CP and HP groups. The LED/HP group presented a higher ΔE00 than the HP group, regardless of the time.
Conclusions
The bleaching efficacy of LED alone was significantly lower compared to the LED/CP and HP-containing protocols. After 12 months, the LED/CP and HP groups did not differ in bleaching efficacy. LED irradiation only increased the objective color change of bleaching gels.
Clinical relevance
LED alone promoted a long-term perceptible bleaching, but not compatible with that of high-concentrated HP. The bleaching outcomes of violet irradiation to 37% CP were maintained over time, with LED/CP demonstrating comparable results to HP even after 12 months.
National Clinical Trials Registry (REBEC)
RBR-5t6bd9
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In-office dental bleaching is one of the most frequent esthetic treatments performed by dentists and is often indicated for fast chromatic and perceptible changes in the anterior teeth [1,2,3,4]. The bleaching gels available for in-office bleaching are composed of highly concentrated hydrogen (HP) or carbamide (CP) peroxides [5]. The main difference between these two gels is the composition of CP, which presents carbamide peroxide with urea. When these compounds come into contact with water, they break down into hydrogen peroxide and ammonium and, later, in oxygen-free radicals and water. Therefore, the CP gel contains only one-third of the total hydrogen peroxide concentration compared to the HP gel [6]. As a consequence, HP may display a higher bleaching efficacy than CP, taking into consideration the same application time [7].
In recent decades, several types of light sources have been used to attempt to increase the efficacy of in-office bleaching gels [8]. The rationale behind this approach is to heat the peroxide gels through the thermal energy generated from the light. As a consequence, the increase in the release of free radicals could enhance the bleaching effects [8, 9]. Researchers have shown controversial bleaching outcomes in regard to the use of the argon laser, halogen lamp, blue LED, or diode laser [10,11,12]. Such divergent outcomes could be explained based on the differences between irradiation protocols, time of use, or irradiance and power stability of the different light sources. Also, differences in the bleaching gel’s type, concentration, or application regimen hinder the comparison among studies [10, 13]. However, systematic reviews concluded that no light irradiation source was able to enhance the efficacy of in-office bleaching gels [8, 13,14,15].
Some clinical reports have suggested the use of a new violet LED light for in-office dental bleaching [16,17,18,19,20]. In these clinical case reports, the violet LED was used in combination with CP and HP. However, the violet LED light manufacturer also recommends the irradiation of violet light without any peroxide or chemical agent [21]. Based on the lower light penetrability of the violet wavelength [22], some authors have speculated that the violet light alone possibly degrades the extrinsic staining molecules adhered to the enamel surface by a photocatalyst process [18, 20].
It is worth mentioning that the violet LED bleaching protocols, combined or not with peroxide agents, have been applied without sufficient evidence to support their efficacy and safety. Only three randomized clinical trials assessed the efficacy of violet LED and its effect on tooth sensitivity, either alone or combined with at least one type of peroxide agent (CP or HP) [23,24,25]. The effect of violet LED alone on tooth sensitivity was minimum. Also, the combination of violet light with 37% CP gel presented the same efficacy as that of the non-irradiated 35% HP gel, but with reduced tooth sensitivity [25].
Even though some clinical trials attest to the limited ability of violet LED to bleach without peroxides or to increase the efficacy of peroxide agents, these reports are part of short-term evaluations only (up to 14-day follow-up) [23,24,25]. Besides, there is no evidence for the clinical efficacy of violet LED irradiation protocols using updated colorimetric systems. None of the clinical trials reported the color change based on the CIEDE2000, a system that corrects discrepancies in the CIELab color change formula [26]. Moreover, the clinical application of the whiteness index for dentistry, an index developed specially to detect the whiteness levels of teeth and is more suitable to visual perception, ought to contribute to the understanding of the topic [27].
Therefore, this study determined the long-term colorimetric evaluation (6 and 12 months from bleaching procedures) from a randomized and controlled clinical trial of violet LED in-office bleaching protocols. The null hypotheses tested were that after 6 and 12 months from bleaching, (1) violet LED light alone would not present the same bleaching efficacy as CP or HP gels, (2) violet irradiation would not increase the color and/or whiteness changes promoted by CP and HP, and (3) irradiation of CP with violet LED would not result in a bleaching efficacy similar to that observed for high-concentrated hydrogen peroxide.
Material and methods
Ethical aspects
The ethical aspects of this clinical trial were approved under the registration numbers: 72879717.7.0000.5418 (Issuing authority: Plataforma Brasil) and 2.229.061 (Issuing authority: Local Ethical Committee). An amendment was also approved by the Local Ethical Committee (3.776.209). This research was registered in the National Clinical Trials Registry (REBEC—RBR-5t6bd9) and followed the CONSORT guidelines. This is a long-term evaluation of a previously short-term published study [25]. Patients included in this study signed an informed consent in accordance with the Declaration of Helsinki before the first clinical session.
Recruitment of volunteers
The patients were recruited from the University through announcement signs distributed into a few facilities of the building. Patients of dental clinics, dental students, faculties, and staff were able to enroll for the initial appointment, which checked the eligibility criteria. Before signing the consent form, potential patientswere clinically evaluated and wereselected based on the inclusion or exclusion criteria found in Table 1.
The number of patients was determined by a sample size calculation, using color change values from a published study [28]. Adopting a 5% level of significance, an 80% power, and a 0.50 effect size (f), the calculation indicated a minimum of 16 patients to detect differences among groups (BioStat, AnalystSoft, Walnut, CA, USA). Twenty volunteers were recruited, taking into consideration a further possibility of drop-out. The short-term study conducted by Kury et al. (2020) showed that 18 patients from each intervention group concluded the bleaching treatments and returned for the 14-day follow-up [25].
Randomization, blinding, and allocation
A research member, not responsible for either treating or evaluating the patients, performed the randomization and allocation concealment of the volunteers (V.C.). A code written in an opaque and sealed envelope was assigned to each participant. Then, the envelopes were randomly distributed into the five intervention groups [24, 28, 29]. The randomization was open only to the operator, before the beginning of the bleaching intervention. Two members were directly involved with the clinical appointments: one operator (E.E.W) and one evaluator (M.K.). The operator was informed of which group each participant was allocated to because of the bleaching agents and light characteristics. However, the evaluator of the colorimetric analysis was blinded to the procedures. The volunteers were not aware of either the type or the concentration of the bleaching gel they were exposed to. For this purpose, any label, brand logo, or packaging that would enable identification of the products was removed [30]. The evaluator was previously calibrated during the in-office bleaching appointments of five participants excluded from the clinical trial. This calibration was performed by measuring the color of the cervical and middle third from the buccal surface of the upper canines after each training bleaching session [29]. The operator was responsible for recording the data. Another research member, also blinded, was in charge of scheduling the follow-up appointments (S.S.P.).
Interventions (bleaching procedures)
The bleaching protocols were defined according to the bleaching gel (HP, CP, or none) and light irradiation method (violet LED or none) used, and patients were randomly allocated into five different groups (n = 20/group): LED, CP, LED/CP, HP, and LED/HP. Table 2 displays the composition of the bleaching gels and the technical specification of violet LED. The bleaching protocols were as follows.
LED
The complete LED irradiation cycle totals 30 min (twenty 1-min irradiations with consecutive 30-s intervals). The gingival tissues were protected with a gingival barrier of flowable composite resin (Top Dam, FGM, Joinville, SC, Brazil) light-cured for 20 s (Valo, Ultradent, South Jordan, UT, USA). The violet LED device (MMOptics, São Carlos, SP, Brazil) was permanently positioned 8 mm away from the arches throughout the irradiation cycles. The teeth were kept hydrated with moist gauze during the intervals. The protocol was repeated for eight sessions at 4-day intervals.
CP or LED/CP
The gingival tissue was protected with a barrier as previously described. The 37% CP gel (FGM, Joinville, SC, Brazil) was applied directly on the teeth’s buccal surface. The CP gel was applied for 30 min without refreshing and either combined with the irradiation of the violet LED light as described above (LED/CP), or without the use of the light source (CP). At the end of the session, the bleaching gel was removed and rinsed from the teeth. The protocol was repeated for three sessions at 7-day intervals.
HP or LED/HP
The thickener and 35% hydrogen peroxide (FGM, Joinville, SC, Brazil) were mixed in a container. This mixture was applied on the entire buccal surface from premolar to premolar with a micro brush after protecting the gingival tissues with a gingival barrier, as previously described. Initially, the gel showed a reddish color, changing to transparent within the first minutes. The HP gel was applied for 30 min without refreshing and either combined with the irradiation of the violet LED light as described above (LED/HP) or without the use of the light source (HP). The protocol was repeated for three sessions at 7-day intervals.
Colorimetric evaluation
A digital spectrophotometer (Easy Shade, Vita Zahnfabrik, Bad Säckingen, Germany) evaluated the upper right canine color. A custom-made silicon barrier (Zhermak, Kouigo, Italy) of each patient's superior arch was obtained. A hole in the cervical/middle region of the upper right canine standardized the position of the spectrophotometer’s tip for readings on the buccal enamel surface [28].
The baseline/initial L* (luminosity: black—/ white +), a* (red + / green -), b* (yellow + / blue -), H (hue), and C (chroma) values were recorded after dental prophylaxis and before the first bleaching session (T0) [25] and after 6 (T6m) and 12 (T12m) months from the last bleaching application. The patients were not submitted to dental prophylaxis at T6m and T12m, but they were required to brush their teeth before the follow-up sessions. During the appointment intervals, the patients were directed to not brush their teeth with whitening toothpaste. The coordinates (L*, a*, b*) were recorded and used to calculate objective color change, which was the primary outcome of the research. ΔEab and ΔE00 (color change) calculations were performed using the CIELab and CIEDE2000 formula, respectively, as follows [26]:
The SL, SC, and SH are weighting functions that adjust the final color change in the location of L*, a*, and b* coordinates. K represents parametric correction factors, and R is a rotation function that establishes interaction among hue and chroma differences in the blue area. Two Δ values were obtained considering two time points ([T6m – T0] and [T12m – T0]). The 50:50% perceptibility threshold (PT) for the adopted values were 1.2 ΔEab and 0.8 ΔE00 units [31].
Moreover, Δ values considering the same time points above were calculated for the whiteness index for dentistry (ΔWID), based on the CIELAB system [27]:
The 50:50% perceptibility threshold for the whiteness index change (WPT) was considered 0.61 ΔWID units [32]. Finally, a visual shade guide (ΔSGU – Vita Zahnfabrik, Bad Säckingen, Germany) evaluated the subjective color change of the upper right canine [33]. The tabs of the shade guide system were sorted in terms of lightness values. According to Table 3, the numbers 1 through 16 were assigned to each value in a decreasing order. The numbers recorded in each appointment were used to calculate the subjective color change. The subjective assessment considered the same time intervals, and the evaluator was previously calibrated and blinded in terms of which group each patient belonged.
Statistical analyses
The normality and the equal variances of the data obtained in the objective colorimetric evaluation were explored using the Shapiro–Wilk and Levene tests (SPSS 23, IBM, Chicago, IL, USA). The data attending both the normality and equal variance assumptions (p > 0.05) were submitted to one-way ANOVA and Tukey’s test. Because the normality distribution of the ΔEab [T6m – T0] and ΔWID [T12m – T0] was confirmed, but the equality of variance assumption failed, data were assessed using Welch’s ANOVA, followed by the post hoc Games-Howell test. The data from the subjective color change (ΔSGU) were analyzed using the non-parametric Kruskal–Wallis and Dunn multiple comparisons’ tests. The significance level was set at 5%.
Results
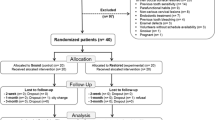
The bleaching procedures and the 14-day follow-up appointments occurred in 2018 [25]. The 6-month and 1-year follow-ups assessed the long-term efficacy of the bleaching protocols during 2019. The flow of the patients throughout the clinical trial and the drop-off numbers per intervention group are illustrated in Fig. 1. Table 4 presents the demographic data of the volunteers.

Flow chart including the long-term evaluation of the volunteers
The observed post hoc power values were above 0.95 for all the outcomes evaluated. Table 5 and Figs. 2 and 3 display the mean objective (ΔEab and ΔE00) and median subjective (ΔSGU) color change values 6 and 12 months from each protocol. After 6 months (T6m – T0), violet LED exhibited the lowest ΔEab among the groups (p < 0.001), with no color differences compared to CP (ΔE00 and ΔSGU; p > 0.05). No differences were observed among CP, LED/CP, and HP according to the objective (ΔEab and ΔE00) and subjective parameters (ΔSGU) (p > 0.05). LED/HP exhibited the highest ΔEab and ΔE00, but its ΔSGU was comparable to those of LED/CP and HP.

Mean and standard deviation values of the objective color changes (ΔEab and ΔE00) after 6 and 12 months from the last bleaching session. Means followed by different letters statistically differ at 5%. The uppercase letters compare different bleaching protocols within the same period of evaluation

Box plot of the subjective color changes (ΔSGU) showing the median, quartile ranges, and minimum and maximum values after 6 and 12 months from the last bleaching session. Medians followed by different letters statistically differ at 5%. The uppercase letters compare different bleaching protocols within the same period of evaluation
After 12 months (T12m – T0), LED and CP groups exhibited the lowest ΔEab and ΔE00 (p < 0.001). CP, LED/CP, and HP exhibited no differences in terms of ΔSGU (p > 0.05). LED/CP presented significantly higher ΔEab and ΔE00 than that obtained with the CP group. LED/HP exhibited the highest color changes among the groups according to ΔE00 (p < 0001), but with no statistical differences to HP (ΔEab and ΔSGU) and LED/CP (ΔSGU).
All the groups presented mean ΔEab and ΔE00 values above the 50:50% perceptibility threshold. The differences among ΔSGU mean values presented the same statistical pattern over time, showing that LED and CP groups did not present statistical differences independently of the evaluation time. Violet LED did not increase the ΔSGU of the CP and HP gels (LED/HP = HP; LED/CP = CP).
Table 6 and Fig. 4 depict the mean ΔWID values after 6 and 12 months from bleaching. The LED group presented the lowest means (p < 0.05) within separate evaluation times. The irradiation of the CP and HP gels with the LED did not significantly increase the ΔWID means (LED/CP = CP; LED/HP = HP) within each evaluation time. LED/CP and HP showed no statistical differences in terms of the whiteness index, independently of the time point (p > 0.05). All the ΔWID means were above the 50:50% perceptibility threshold.

Mean and standard deviation values of the whiteness index for dentistry changes (ΔWID) after 6 and 12 months from the last bleaching session.Means followed by different letters statistically differ at 5%. The uppercase letters compare the different bleaching protocols within the same period of evaluation
Discussion
Although there are few available clinical trials on the efficacy of violet LED for in-office bleaching [23,24,25], those studies demonstrated only the short-term effects on the colorimetric outcomes. The 6- and 12-month follow-ups of this study demonstrated that the violet LED alone produced color and whiteness changes significantly inferior to the HP groups. However, LED alone and CP exhibited no statistical differences concerning the ΔEab and ΔE00 at the 12-month evaluation. Therefore, the first null hypothesis was rejected because the violet LED alone promoted color change comparable to those of the peroxide agents. It is possible to observe that the objective differences (ΔEab) between the LED and CP groups were maintained up to the 6-month follow-up. Nevertheless, the 12-month evaluation suggested a color rebound in the CP group, which could have favored the similarity among LED and CP. Interestingly, the subjective color change (ΔSGU) revealed no differences between these two groups throughout the study.
In this context, the discrepancies among colorimetric outcomes could be credited to the method of data collection itself. The ΔSGU is considered a subjective method that lighting, age, gender, and eye fatigue might directly impact the decision of the teeth’s value [34]. On the other hand, the ΔE00, ΔEab, and ΔWID data are calculated based upon CIELab coordinates collected from precise instruments such as spectrophotometers. This equipment provides the coordinate values by means of a visible spectral reflectance process [35]. Even though subjective color determination is widely used because the visual shade guide is cost-effective, previous studies pointed out that the objective evaluations are more accurate than visual shade tabs [35, 36].
Researchers hypothesized that the mechanism of the action of violet LED alone is based on the interaction of the visible wavelength (approximately 405 nm) with the extrinsic staining adhered to the surface of buccal enamel [18, 21]. Indeed, in vitro studies showed that the irradiation of artificially stained teeth by violet LED resulted in medium to high color or whiteness changes [19, 37, 38]. However, the outcomes obtained in the present clinical scenario suggested that the light effect alone is perceptible, but less efficient than high-concentrated hydrogen peroxide. Thus, the fact that patients exhibited teeth with lower staining and were submitted to prophylaxis before bleaching might have impacted the outcomes.
Since the whiteness index for dentistry calculation takes into account the CIELab coordinates [27], it makes sense that the WID changes promoted by violet LED were significantly lower than the CP and HP groups. The WID evaluation indicates changes in the teeth’s spectral behavior that migrate to high lightness and low saturation [27]. Also, this index performs a greater correlation with visual color perception. Based on the ΔWID presented in this study, it is possible to infer that the impact of the light itself on the whiteness of teeth was significantly lower than that of peroxide-based agents.
The color change calculation based on the CIEDE2000 system is an important data that was also not used in the previous clinical trials on the violet LED in-office bleaching [23,24,25]. The differences among the ΔEab and ΔE00 calculations rely on the weighting functions that adjust the final ΔE00 in the location of the L*, a*, and b* coordinates. Applying the lightness, hue, and chroma, CIEDE2000 corrects the interaction of hue and chroma in the b* coordinate. It also alters the low influence of the a* coordinate, which is important only for colors with low chroma [39]. A recent review from Paravina et al. (2019) displayed the individual ΔEab and ΔE00 values compatible with visual perceptibility as well as with excellent efficacy of bleaching [40]. Therefore, the authors of this study believed that the inclusion of these three objective parameters (ΔEab, ΔE00 and ΔWID) would guarantee a more accurate and broader discussion.
The violet LED irradiation increased the ΔEab and ΔE00 of the CP gel, but only at the 12-month evaluation. Thus, the second null hypothesis that bleaching gels irradiated by violet LED would not present higher changes than CP or HP alone was rejected. The decrease in the color change of the CP group (without light) after 12 months could be credited for the lower decomposition of the CP gel into hydrogen peroxide [6]. However, a 6% HP gel, which presents lower total hydrogen peroxide concentration than 37% CP, resulted in stable color change after 1 year [41]. Therefore, the presence of urea in the CP gel might have decreased the CP by-products (without LED irradiation) interaction in the dentin. Also, the characteristics and habits of each patient cannot be ruled out, because the patients’ habits, such as the consumption of dark beverages or even toothbrushing, influence the color rebound [42].
On the other hand, the more stable LED/CP outcomes might be a result of the synergistic effect of the CP itself and the photolytic activity of the violet light [9]. Even though previous clinical trials concluded that the painful sensation during bleaching was lower for the CP protocol, CP did not attain the chromatic changes as observed for HP [7, 25]. Vaez et al. (2019) showed that the humidification with a damp gauze of enamel prior to the 37% CP application enhanced the efficacy of the in-office bleaching protocol [43]. Thus, activation methods could be appropriate to increase the 37% CP bleaching outcomes. LED/CP presented a color change significantly higher than CP only at the 12-month evaluation, but its similarity with HP was observed independent of the evaluation time. Therefore, the third null hypothesis that LED/CP and HP groups’ changes would not be similar after 12 months was rejected. Clinically, this observation for LED/CP could be extrapolated to a stable and high-efficient [40] bleaching protocol with lower levels of tooth sensitivity [25] in comparison to 35% HP.
The significantly higher ΔEab and ΔE00 results of LED/HP compared to the HP protocol observed at the 6-month follow-up were only replicated for ΔE00 at the 12-month follow-up. An important limitation regarding these results was the different number of patients able to return to the last appointment in each group. The drop-off was justified because patients moved to long-distance cities. The highest drop-out rate in the HP group (n = 4) at T12m could have been responsible for the increase in the standard deviation, not resulting in statistical difference between the groups in the ΔEab evaluation. However, the CIEDE2000 system displayed a higher color change for LED/HP even under such circumstances. Regardless of the increase detected in ΔE00 for LED/HP, it is worth mentioning that the intensity of tooth sensitivity for this group during bleaching was overall higher in comparison to HP [25]. Also, the HP and LED/CP protocols exhibited excellent bleaching efficacy [39], thereby questioning the necessity of irradiating the HP gel.
It is important to highlight that the colorimetric analyses herein were only performed using the upper right canine. The decision to use the upper canine was based upon the fact that the chromophores are located in the dentin [6]. Also, a previous study in the literature showed that the esthetic outcomes on thicker teeth tend to saturate later than in thinner teeth, i.e., the upper central incisor [44]. However, further studies could attempt to evaluate if the bleaching outcomes with the present protocols would be different in other dental elements.
Since all the patients reported absence of tooth sensitivity symptoms after 1 week from the last bleaching appointment, no tooth sensitivity data was added to this study. No complaints regarding tooth sensitivity were reported at either the 6- and 12-month follow-ups. Also, further studies could evaluate other application times of the bleaching gels, as the present clinical trial applied the protocols recommended by the light manufacturer and published in previous studies [19, 20]. Following the American Dental Association (ADA) guidelines, effective and safe performance of bleaching in patients is dependent on an appropriate standard exam and the correct diagnosis of the dental discoloration prior to treatment [45].
To summarize, the colorimetric evaluation over time of patients showed that the color and whiteness changes caused by the violet LED alone is perceptible. However, this protocol did not translate into the high levels of bleaching efficacy and did require a longer treatment time. In other words, patients would be submitted to 8 sessions of violet LED bleaching without reaching the esthetic outcomes observed for peroxide-driven bleaching. On the other hand, the violet LED irradiation of CP promoted stable colorimetric changes and exhibited long-term similar efficacy to HP. At the 12-month follow-up, the ΔE00 was the only colorimetric parameter showing significant increase in efficacy for LED/HP.
Conclusion
Within the limitations of this study, the possible conclusions could be drawn as follows:
-
The use of violet LED alone (without bleaching gels) resulted in perceptible long-term bleaching outcomes, but its efficacy was significantly lower than LED/CP and HP-containing protocols;
-
The increase in the long-term efficacy of CP and HP gels irradiated with violet LED was dependent on the evaluation time and the colorimetric system. The combination of violet LED with gels tended to increase the long-term color change (ΔEab and ΔE00) outcomes, but not the ΔWID results;
-
LED/CP reached the efficacy (ΔEab, ΔE00, and ΔWID) of the HP protocol even after 12 months from the bleaching procedures.
References
Silva F, Chisini LA, Demarco FF, Horta BL, Correa MB (2018) Desire for tooth bleaching and treatment performed in Brazilian adults: findings from a birth cohort. Braz Oral Res 32:e12. https://doi.org/10.1590/1807-3107bor-2018.vol32.0012
Pavicic DK, Kolceg M, Lajnert V, Pavlic A, Brumini M, Spalj S (2018) Changes in quality of life induced by tooth whitening are moderated by perfectionism: a randomized, double-blind, placebo-controlled trial. Int J Prosthodont 31:394–396. https://doi.org/10.11607/ijp.5499
Basting RT, Amaral FL, França FM, Flório FM (2012) Clinical comparative study of the effectiveness of and tooth sensitivity to 10% and 20% carbamide peroxide home-use and 35% and 38% hydrogen peroxide in-office bleaching materials containing desensitizing agents. Oper Dent 37:464–473. https://doi.org/10.2341/11-337-C
Kose C, Calixto AL, Bauer JR, Reis A, Loguercio AD (2016) Comparison of the effects of in-office bleaching times on whitening and tooth sensitivity: a single blind, randomized clinical trial. Oper Dent 41:138–145. https://doi.org/10.2341/15-085-C
Rodríguez-Martínez J, Valiente M, Sánchez-Martín MJ (2019) Tooth whitening: from the established treatments to novel approaches to prevent side effects. J Esthet Rest Dent 31:431–440. https://doi.org/10.1111/jerd.12519
Kwon SR, Wertz PW (2015) Review of the mechanism of tooth whitening. J Esthet Rest Dent 27:240–257. https://doi.org/10.1111/jerd.12152
Peixoto AC, Vaez SC, Pereira N, Santana C, Soares K, Romão A, Ferreira LF, Martins-Filho P, Faria-E-Silva AL (2018) High-concentration carbamide peroxide can reduce the sensitivity caused by in-office tooth bleaching: a single-blinded randomized controlled trial. J Appl Oral Sci 26:e20170573. https://doi.org/10.1590/1678-7757-2017-0573
SoutoMaior JR, de Moraes S, Lemos C, Vasconcelos B, Montes M, Pellizzer EP (2019) Effectiveness of light sources on in-office dental bleaching: a systematic review and meta-analyses. Oper Dent 44:E105–E117. https://doi.org/10.2341/17-280-L
Joiner A (2006) The bleaching of teeth: a review of the literature. J Dent 34:412–419. https://doi.org/10.1016/j.jdent.2006.02.002
Lima DA, Aguiar FH, Liporoni PC, Munin E, Ambrosano GM, Lovadino JR (2009) In vitro evaluation of the effectiveness of bleaching agents activated by different light sources. J Prosthodont 18:249–254. https://doi.org/10.1111/j.1532-849X.2008.00420.x
Marson FC, Sensi LG, Vieira LC, Araújo E (2008) Clinical evaluation of in-office dental bleaching treatments with and without the use of light-activation sources. Oper Dent 33:15–22. https://doi.org/10.2341/07-57
Ontiveros JC, Paravina RD (2009) Color change of vital teeth exposed to bleaching performed with and without supplementary light. J Dent 37:840–847. https://doi.org/10.1016/j.jdent.2009.06.015
Maran BM, Ziegelmann PK, Burey A, de Paris MT, Loguercio AD, Reis A (2019) Different light-activation systems associated with dental bleaching: a systematic review and a network meta-analysis. Clin Oral Investig 23:1499–1512. https://doi.org/10.1007/s00784-019-02835-x
He LB, Shao MY, Tan K, Xu X, Li J (2012) The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: a systematic review and meta-analysis. J Dent 40:644–653. https://doi.org/10.1016/j.jdent.2012.04.010
Maran BM, Burey A, de Paris MT, Loguercio AD, Reis A (2018) In-office dental bleaching with light vs. without light: a systematic review and meta-analysis. J Dent 70:1–13. https://doi.org/10.1016/j.jdent.2017.11.007
Panhoca VH, Oliveira BP, Rastelli ANS, Bagnato VS (2017) Dental bleaching using violet light alone: clinical case report. Dentistry 7:1–4
Lago A, Ferreira W, Furtado GS (2017) Dental bleaching with the use of violet light only: reality or future? Photodiag Photodyn Ther 17:124–126. https://doi.org/10.1016/j.pdpdt.2016.11.014
Rastelli A, Dias HB, Carrera ET, de Barros A, Dos Santos D, Panhóca VH, Bagnato VS (2018) Violet LED with low concentration carbamide peroxide for dental bleaching: a case report. Photodiag Photodyn Ther 23:270–272. https://doi.org/10.1016/j.pdpdt.2018.06.021
Gallinari MO, Cintra L, Souza M, Barboza A, Esteves L, Fagundes TC, Briso A (2019) Clinical analysis of color change and tooth sensitivity to violet LED during bleaching treatment: a case series with split-mouth design. Photodiag Photodyn Ther 27:59–65. https://doi.org/10.1016/j.pdpdt.2019.05.016
Kury M, Resende BA, da Silva DP, Wada EE, Antonialli FM, Giannini M, Cavalli V (2019) Clinical application of violet LED in-office bleaching with or without traditional systems: case series. Oral Health Dent Stud 2:1–11
Zanin F (2016) Recent advances in dental bleaching with laser and LEDs. Photomed Laser Surg 34:135–136. https://doi.org/10.1089/pho.2016.4111
Rueggeberg FA, Giannini M, Arrais C, Price R (2017) Light curing in dentistry and clinical implications: a literature review. Braz Oral Res 31:e61. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0061
Brugnera AP, Nammour S, Rodrigues JA, Mayer-Santos E, de Freitas PM, Brugnera A, Junior A, Zanin F (2020) Clinical evaluation of in-office dental bleaching using a violet light-emitted diode. Photobiomodul Photomed Laser Surg 38:98–104. https://doi.org/10.1089/photob.2018.4567
Gallinari MO, Cintra L, Barboza A, da Silva L, de Alcantara S, dos Santos PH, Fagundes TC, Briso A (2020) Evaluation of the color change and tooth sensitivity in treatments that associate violet LED with carbamide peroxide 10 %: a randomized clinical trial of a split-mouth design. Photodiag Photodyn Ther 30:101679. https://doi.org/10.1016/j.pdpdt.2020.101679
Kury M, Wada EE, Silva D, Tabchoury C, Giannini M, Cavalli V (2020) Effect of violet LED light on in-office bleaching protocols: a randomized controlled clinical trial. J Appl Oral Sci 28:e20190720. https://doi.org/10.1590/1678-7757-2019-0720
Sharma G, Wu W, Dalal EN (2005) The CIEDE2000 color-difference formula: implementation notes, supplementary test data, and mathematical observations. Color Res App 30:21–30
Pérez M, Ghinea R, Rivas MJ, Yebra A, Ionescu AM, Paravina RD, Herrera LJ (2016) Development of a customized whiteness index for dentistry based on CIELAB color space. Dent Mater 32:461–467. https://doi.org/10.1016/j.dental.2015.12.008
Loguercio AD, Servat F, Stanislawczuk R, Mena-Serrano A, Rezende M, Prieto MV, Cereño V, Rojas MF, Ortega K, Fernandez E, Reis A (2017) Effect of acidity of in-office bleaching gels on tooth sensitivity and whitening: a two-center double-blind randomized clinical trial. Clin Oral Investig 21:2811–2818. https://doi.org/10.1007/s00784-017-2083-5
Santos AECGD, Bussadori SK, Pinto MM, Pantano Junior DA, Brugnera A Jr, Zanin FAA, Rodrigues MFSD, Motta LJ, Horliana ACRT (2018) Evaluation of in-office tooth whitening treatment with violet LED: protocol for a randomised controlled clinical trial. BMJ Open 8:e021414. https://doi.org/10.1136/bmjopen-2017-021414
Vildósola P, Bottner J, Avalos F, Godoy I, Martín J, Fernández E (2017) Teeth bleaching with low concentrations of hydrogen peroxide (6%) and catalyzed by LED blue (450 ± 10 nm) and laser infrared (808 ± 10 nm) light for in-office treatment: randomized clinical trial 1-year follow-up. J Esthet Restor Dent 29:339–345. https://doi.org/10.1111/jerd.12318
Paravina ZD, Ghinea R, Herrera LJ, Bona AD, Igiel C, Linninger M, Sakai M, Takahashi H, Tashkandi E, Perez M (2015) Color difference thresholds in dentistry. J Esthet Rest Dent 27:S1–S9. https://doi.org/10.1111/jerd.12149
Pérez MM, Herrera LJ, Carrillo F, Pecho OE, Dudea D, Gasparik C, Ghinea R, Bona AD (2019) Whiteness difference thresholds in dentistry. Dent Mater 35:292–297. https://doi.org/10.1016/j.dental.2018.11.022
Martini EC, Favoreto MW, Coppla FM, Loguercio AD, Reis A (2020) Evaluation of reservoirs in bleaching trays for at-home bleaching: a split-mouth single-blind randomized controlled equivalence trial. J Appl Oral Sci 28:e20200332. https://doi.org/10.1590/1678-7757-2020-0332
Joiner A, Luo W (2017) Tooth colour and whiteness: a review. J Dent 67S:S3–S10. https://doi.org/10.1016/j.jdent.2017.09.006
iel C, Weyhrauch M, Wentaschek S, Scheller H, Lehmann KM, (2016) Dental color matching: a comparison between visual and instrumental methods. Dent Mater J 35:63–69. https://doi.org/10.4012/dmj.2015-006
Liberato WF, Barreto IC, Costa PP, de Almeida CC, Pimentel W, Tiossi R (2019) A comparison between visual, intraoral scanner, and spectrophotometer shade matching: a clinical study. J Prosthet Dent 12:271–275. https://doi.org/10.1016/j.prosdent.2018.05.004
Kury M, Perches C, da Silva DP, André CB, Giannini TCPM, M, Cavalli V, (2020) Color change, diffusion of hydrogen peroxide, and enamel morphology after in-office bleaching with violet light or nonthermal atmospheric plasma: an in vitro study. J Esthet Rest Dent 32:102–112. https://doi.org/10.1111/jerd.12556
Kobayashi RS, Picolo MZD, Kury M, de Almeida Resende B, Florez FLE, Cavalli V (2021) Effects of dental bleaching protocols with violet radiation on the color and chemical composition of stained bovine enamel. Photodiag Photodyn Ther 102194. Advance online publication. https://doi.org/10.1016/j.pdpdt.2021.102194
Pecho OE, Ghinea R, do Amaral EA, Cardona JC, Della Bona A, Pérez MM (2016) Relevant optical properties for direct restorative materials. Dent Mater 32:e105–e112. https://doi.org/10.1016/j.dental.2016.02.008
Paravina RD, Pérez MM, Ghinea R (2019) Acceptability and perceptibility thresholds in dentistry: a comprehensive review of clinical and research applications. J Esthet Rest Dent 31:103–112. https://doi.org/10.1111/jerd.12465
Estay J, Angel P, Bersezio C, Tonetto M, Jorquera G, Peña M, Fernández E (2020) The change of teeth color, whiteness variations and its psychosocial and self-perception effects when using low vs. high concentration bleaching gels: a one-year follow-up. BMC Oral Health 20:255. https://doi.org/10.1186/s12903-020-01244-x
Chen YH, Yang S, Hong DW, Attin T, Yu H (2020) Short-term effects of stain-causing beverages on tooth bleaching: a randomized controlled clinical trial. J Dent 95:103318. https://doi.org/10.1016/j.jdent.2020.103318
Vaez SC, Correia A, Santana TR, Santana M, Peixoto AC, Leal PC, Faria-E-Silva AL (2019) A simple method to increase the bleaching effectiveness of high-concentrated carbamide peroxide used for in-office bleaching. J Esthet Rest Dent 14:324–332
de Oliveira Duque CC, Soares DG, Basso FG, Hebling J, de Souza Costa CA (2017) Influence of enamel/dentin thickness on the toxic and esthetic effects of experimental in-office bleaching protocols. Clin Oral Investig 21(8):2509–2520. https://doi.org/10.1007/s00784-017-2049-7
American Dental Association – ADA (2020) Statement on the safety and effectiveness of tooth whitening products. https://www.ada.org/en/about-the-ada/ada-positions-policies-and-statements/tooth-whitening-safety-and-effectiveness. Assessed 20 April 2021
Funding
This research was supported by the São Paulo State Research Foundation (FAPESP – #2017/08625–0, #2017/23841–1 and #2017/24847–3). This study was financed in part by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Piracicaba Dental School Ethical Committee—2.294.061 and 3.776.209) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
M. Kury has received research grant (FAPESP #17–08625-0). E. E. Wada has received research grant (FAPESP #17–24847-3). V. Cavalli has received research grant (FAPESP #17–23841-1).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kury, M., Wada, E.E., da Silva Palandi, S. et al. Colorimetric evaluation after in-office tooth bleaching with violet LED: 6- and 12-month follow-ups of a randomized clinical trial. Clin Oral Invest 26, 837–847 (2022). https://doi.org/10.1007/s00784-021-04062-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-04062-9