
Abstract
The aim of this study was to investigate the tooth-whitening efficacy and oral side effects of the two tray-based bleaching systems Visalys whitening (VW) and Opalescence PF (OP). A stratified, randomised distribution of the subjects (n = 60) to two treatment groups was performed according to baseline tooth brightness (L* values) as determined by colourimeter and to the criteria smoker/non-smoker. Tooth colour was evaluated by measuring L*a*b* values generated from standardised digital image analysis with Adobe Photoshop® of the facial surfaces of the right central maxillary incisor. Tooth hypersensitivity, with intensity graded from 0 (no hypersensitivity) to 10 (high hypersensitivity), was assessed chair-side using an air syringe. After bleaching therapy, both treatment groups demonstrated significant improvements in tooth colour (p ≤ 0.05). A shift towards less yellow (−Δb*) and brighter (+ΔL*) tooth colour was observed. Δb* was significantly higher in the OP group in comparison to the VW group, ΔL* showed no significant difference between the both treatment groups (p ≤ 0.05). After bleaching, the intensity of tooth hypersensitivity was increased significantly compared to baseline in both groups (p ≤ 0.05), with no significant difference between the both groups. Both highly concentrated bleaching systems are effective as tooth-whitening systems, with few reported side effects such as transient tooth hypersensitivity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tooth bleaching with hydrogen peroxide or carbamide peroxide has enjoyed great popularity to enhance aesthetics in anterior teeth. It has been reported that bleaching is a safe and effective method that provides a less-invasive and less-costly alternative than crowns or veneers for treatment of discoloured teeth [39, 46, 49].
Acceptable whitening technique included the “in-office” technique (professionally applied) and the “at-home” applied technique (patient applied), or a combination of those [20, 23]. Home bleaching agents most commonly consist of 10 or 15% carbamide peroxide gel, which is equivalent to 3.6 and 5.4% hydrogen peroxide, respectively [44]. Beside, variety of gel systems with varying peroxide concentrations, flavours, desensitizing agents or other modifications to the formulation are available [11]. Both bleaching agents with hydrogen peroxide or carbamide peroxide as primary active ingredients have been demonstrated to be effective for external bleaching [2, 29, 30, 35].
A number of methods are available for evaluating the efficacy of bleaching products [14]. Shade guides, photography, colourimetry or computer digitisation can be used to assess tooth-colour changes. Tooth-colour determination using the commonly cited shade-based guides have limitations as they are subjected to examiner and environmental factors that can potentially influence classification of tooth colour [18, 28]. The L*a*b* Centre Internationale De L’Eclairage three-dimensional colour space scale is the most frequently quoted index used in bleaching research and can be generated from colourimetric, spectrophotometric or digital image analysis [9]. Digital images are analysed on L*a*b* values using computer software analysis. Bengel [5] demonstrated an analysis of digital images with commercial software (Adobe Photoshop) and found reproducible results.
Tolerability issues associated with peroxide-based bleaching therapies are well-documented and well-characterised with transient tooth hypersensitivity and gingival irritation documented as the most commonly reported side effects [4, 7, 24, 25, 31, 40, 45]. The tooth hypersensitivity is temporary and ceases when treatment terminates, without apparent harm to the pulp [47]. The bleaching mechanism is based on the ability of hydrogen peroxide to penetrate tooth structure and produce free radicals that oxidise organic stains within the tooth [37]. Feinman et al. [12] concluded, in a review about the physiologic mechanisms of bleaching products, that the bleaching agent oxidises organic material in the inter-prismatic spaces. Bubbling and foaming of the free oxygen softens and removes the inter-prismatic debris. The free movement of the hydrogen peroxide through the enamel, dentin and pulp may cause the transient hypersensitivities. Up to 65% of individuals have been reported to be affected at least once during the bleaching regimen. Such events are generally mild in nature and resolve either during or upon completion of treatment. These effects have been reported for virtually all delivery systems and peroxide concentrations although it was suggested that highly concentrated professionally administered, in-office treatments may enhance tooth hypersensitivity to a higher extent than home-bleaching applications [40]. It was shown that the higher the concentration of a bleaching agent is, the greater is the risk of tooth hypersensitivity [38]. Other oral soft-tissue side effects have also been reported. Pohjola et al. [45] observed gingival irritation in 20–30% of the participants in a recent study, whilst in a study published by Haywood et al. [25], gingival irritations were observed in 31% of the cases during at-home bleaching. Tolerability of side effects seems to be dependent upon peroxide concentration and contact time of the bleaching agent with the teeth [8, 17].
Side effects may also depend on the kind of peroxide formulation in a bleaching product. Carbamide peroxide needs be hydrolytically cleaved by salivary impact into carbamide and hydrogen peroxide before the chemical process of bleaching. In bleaching systems containing pure hydrogen peroxide, the active bleaching agent is already readily available. Because of the difference in chemistry, carbamide peroxide systems are usually advised to be applied for longer time periods at each daily application than pure hydrogen peroxide systems. The different kinetics of peroxide release may have an impact on both efficacy and intra-oral side effects.
Therefore, the aim of the study was to compare the efficacy of a 7.5% hydrogen peroxide tray bleaching system versus a 20% carbamide peroxide (i.e. 7.2% hydrogen peroxide) custom tray bleaching system. Additionally, the degree and frequency of oral side effects were investigated to evaluate clinical tolerability of both bleaching products.
Materials and methods
Products used in the study
This mono-centric, randomised, two-armed, parallel clinical study evaluated the efficacy and tolerability of two tray-based bleaching systems. The study was reviewed and approved by the Ethics Committee of the University of Goettingen (no.: 5/6/04). The time flow of the study is given in Table 1.
The two bleaching systems tested in this study were Visalys whitening (VW; Kettenbach, Eschenburg, Germany) and Opalescence PF (OP; Ultradent, South Jordan, USA). VW is a 7.5% hydrogen peroxide gel (Lot# 04139001) and OP is a 20% carbamide peroxide gel (Lot# 85612.2). Twenty percent carbamide peroxide is equivalent to 7.2% hydrogen peroxide. Bleaching was performed for 12 days according to manufacturers instructions with subjects assigned to the VW group undergoing two applications a day of 30 min each, those assigned to the OP undergoing one application of 4 h/day. About 200–300 mg gel were used for one charge of the tray. Maxillary trays were vacuum formed from 1.5-mm thick soft acrylate foils on plaster models. The canines and incisors were augmented on labial surfaces out with composite (1.5-mm thickness) before manufacturing of the tray to achieve a reservoir. The trays were filled with VW or OP in the area of incisors and canines only.
Subjects
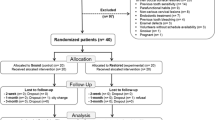
Sixty volunteers with restoration or caries-free teeth, tooth colour Vita shade A2 or darker, no crowns on upper cuspids or incisors were enrolled in the study at baseline. Thirty subjects were treated with the tray system VW (group A) and 30 with tray bleaching system OP (group B). A stratified, randomised distribution of the subjects to the two treatment groups was performed according to the baseline tooth brightness (L* values) as determined by a dental colourimeter (Shade Eye—Shofu Dental Corporation, San Marcos, CA) and according to the criteria smoker/non-smoker (Table 2).
Subjects were advised to use no other bleaching products throughout the study and were provided with tooth brushes (Oral B P35, Gillette, Ireland) and tooth paste (elmex, GABA GmbH, Lörrach, Germany) to ensure standardised oral hygiene procedures for the period of the study.
Patients with prior tooth hypersensitivities, anterior restorations, poor oral hygiene, generalised gingival recession, caries, heavy structural alteration of the tooth structure and tetracycline or fluorosis staining were not included in the study. Furthermore, patients with infectious diseases, high risk for endocarditis, allergic reactions versus components of the bleaching agents, xerostomia as well as pregnant or breastfeeding women were excluded in accordance with the regulations of the Ethics Committee of the University of Goettingen.
Efficacy of the bleaching systems—digital imaging and colour determination
Tooth colour of the facial surfaces of the right central maxillary incisor was measured using standardised digital image photography and analysis technology from Adobe Photoshop® (Adobe Systems Incorporated, San Jose, CA) as described by Bengel [5]. Imaging was carried out at baseline and 5 days after bleaching therapy after a dental prophylaxis.
Standardised digital images were captured with a high-resolution digital colour (Canon EOS 10D, Tokyo, Japan). The camera was equipped with a linear polariser to permit cross-polarised light. The lights were equipped with blue filters (Hama, Monheim, Germany) to use the camera at a constant colour temperature (about 5,000 K). Linear polarisers mounted on the lights allowed the camera-mounted linear polariser to be adjusted for extinction of highlights (specular reflection). For each examination period, extrinsic lighting in the examination room was minimal and standardised. Subjects were positioned on a chair in front of a chin rest used to fix the head in a reproducible position. The subject placed their chins on the chin rest. All photography was performed at the same distance (100 cm) of object (tooth) to lens. Two plastic retractors were used to retract lips and cheeks. The operator positioned the subject so that the central maxillary incisor was in the plane of focus.
As a colour reference, a circular (1 mm in diameter) patch obtained from a standardised professional photography gray card (QP Card 101, QPcard AB, Göteborg, Sweden) was positioned on the gingiva adjacent to the two central incisors. The gray card has a reflectance value of 18% and represented the middle tone used for exposure determination, halfway between pure black and pure white. The gray card patch acts as a neutral test target. In a first step, the image is fine-tuned and standardised with regard to brightness using the gray patch as a reference. Then, colour values of the right central maxillary incisor were determined with Adobe Photoshop® and converted to L*a*b* values representing a standard three-dimensional colour space (L*: brightness—dark to light, a*: green to red and b*: blue to yellow) according to Commission Internationale de L’Eclairage [9].
Evaluation of tooth hypersensitivities
The evaluation of hypersensitivities was performed at baseline, at the end of therapy and 5 days after bleaching therapy with a gentle stream of cold air applied with the multi-purpose syringe of the dental unit. Hypersensitivities were graded on a scale from 0 to 10 (0 = no hypersensitivity, 10 = high hypersensitivity). The stimulus was defined as a 2-s air blast delivered from the multi-purpose syringe of a dental unit, with its nozzle held in a distance of 2 mm from the labial site of the maxillary anterior teeth to be tested.
In addition, the self-reported hypersensitivities during bleaching regimen were registered by the subjects in a kind of diary. The patients were instructed to rinse with cold water (5 ± 1°C) once a day and to grade the degree of hypersensitivity on a scale from 0 to 10 (0 = no hypersensitivity, 10 = high hypersensitivity).
Evaluation of tolerability
At baseline, at the end of therapy and 5 days after therapy, a full oral examination was carried out by a trained examiner. One day after the end of therapy, an additional examination of the oral cavity was performed out to check if any ongoing side effects had resolved fully. Any abnormal findings such as redness, oedema or epithelial irritation of soft tissues were recorded. Irritation was defined as desquamation of the outer layers of the gingival epithelium appearing as a white layer. Subjects were also interrogated with respect to any symptoms perceived during the bleaching therapy. All reported adverse effects were recorded by the examiner.
Evaluation of acceptability
After completion of bleaching treatment, subjects were interrogated on the acceptance of the bleaching therapy. The patients had to evaluate whether the treatment was comfortable, slightly disturbing, uncomfortable or very uncomfortable. Five days after therapy, patients were asked if they would recommend the therapy to associates/friends and if they were disposed to repeat therapy.
Statistical analysis
Statistical analysis was done with parametric analysis for ΔL*, Δa* and Δb* and non-parametric analysis of variance (Kruskal–Wallis test) for hypersensitivity. Comparisons between the two groups with respect to the different parameters analysed were performed with t tests. Level of significance was set at p ≤ 0.05.
Results
Three subjects from the Visalys group and one from the Opalescence group withdrew during bleaching therapy because of product-related side effects. These were reported by the subjects as severe tooth hypersensitivity, gum irritation and toothache.
Whitening effect
The colour change (ΔL*, Δa* and Δb*) for both groups are given in Table 3.
After bleaching therapy, tooth colour had changed significantly for ΔL*, Δa* and Δb* (p < 0.001) compared to baseline in both treatment groups. A significant shift towards less yellow (−Δb*) and brighter (+ΔL*) tooth colour was observed for both groups. Δb* amounted to −2.26 ± 1.29 for group A: VW and −3.15 ± 1.27 for group B: OP (mean ± standard deviation). ΔL* was +1.60 ± 1.83 for VW and +2.59 ± 3.05 for OP (mean ± standard deviation). No significant difference between treatment groups was recorded for ΔL* (p = 0.46) and Δa* (p = 0.32). However, Δb* colour determination for Opalescence was significantly different compared to VW (p < 0.029). L* and b* values before and after whitening treatment are shown in Figs. 1 and 2.

Plot of L* values before and after whitening treatment for Visalys whitening and Opalescence PF

Plot of b* values before and after whitening treatment for Visalys whitening and Opalescence PF
In both treatment groups, smokers and non-smokers did not show significant difference in bleaching outcome (ΔL*: p = 0.57; Δa*: p = 0.9; Δb*: p = 0.41).
Hypersensitivities
Hypersensitivities as assessed with the chair-side-applied stream of cold air
At the end of the bleaching therapy, the intensity of tooth hypersensitivity was significantly different compared to baseline in both treatment groups (p ≤ 0.05): group A, 1.67 ± 1.90 (baseline, 0.33 ± 0.52); group B, 2.66 ± 2.70 (baseline, 0.69 ± 1.05). There was no significant difference (p ≤ 0.05) between both treatment groups (Table 4). The hypersensitivities 5 days after the bleaching therapy were not significantly different as compared to baseline.
Hypersensitivity as assessed by the subjects using cold water
As graded by the subjects, perceived hypersensitivities increased in both groups significantly during bleaching therapy compared to baseline (p ≤ 0.05), with the two groups differing significantly. In the Opalescence group, average degree of hypersensitivities was statistically significantly higher compared to the Visalys group (Fig. 3).

Plot of mean intensity of self-reported hypersensitivity (0 = no hypersensitivity; 10 = strongest hypersensitivity). Bleaching was performed on day 1–12
Tolerability
Gingival irritation was observed during bleaching therapy in 78.6% of all patients (VW, 77.8%; OP, 79.3%) with mild inflammation of gingival (red colour), 41.1% with erosive alteration of gingival (VW, 33.3%; OP, 48.3%) and 67.9% gum burning/irritation (VW, 74.1%; OP, 62.1%). There were no significant differences in observed or reported evaluations of tolerability between the two tray bleaching systems. In all cases, the gingival irritations observed were mild and restricted to the gingival margins. These events were transient and fully resolved after the end of the bleaching regimen.
Recommendation and repetition of the bleaching regimen
Seventy-eight percent of the volunteers using VW (group A) stated that they would recommend it to an associate/friend compared to the Opalescence group (group B), where 62% of the subjects would recommend the product to an associate/friend. The comparison yielded no significant difference between the two groups. Seventy-eight percent of subjects in group A and 66% of subjects in group B claimed to be interested in repetition of the therapy. However, there was no significant difference between group A and B.
Comfort of the bleaching regimen
In both groups, a similar proportion of subjects complained on lack of comfort with no significant difference between the two groups.
Twenty-eight percent of all subjects rated the bleaching therapy as comfortable (group A, 29.6%; group B, 27.6) and 48.1% rated it as slightly uncomfortable (group A, 55.6%; group B, 41.4). Eighteen percent (group A, 7.4%; group B, 27.6) and 5% (group A, 7.4%; group B, 3.4) of all subjects described the regimen as uncomfortable or very uncomfortable. Thus, the majority of the subjects (76.7%) did not have severe complaints on the therapy.
Discussion
In the present study, the efficacy and side effects of two different highly concentrated tray-based bleaching systems VW and OP was tested. The two products exhibit nearly the same peroxide concentration, with the one product as carbamide peroxide and the other as pure hydrogen peroxide. It is assumed that these different peroxide formulations might have a different behaviour with respect to peroxide liberation. However, it should be noticed that other ingredients or patterns of the two products, such as viscosity, might have an impact on peroxide release kinetics as well but were not included in the analysis of the present study. This was due to fact that the manufacturers did not disclose the complete compositions of the gels.
Different procedures, shade guides, photography, colourimetry or computer digitisation are described for determination of bleaching efficacy and tooth whitening [17, 25, 28, 42]. In earlier studies, product effects were largely characterised by relating changes in tooth colour against individual shades such as the tabs of the Vita system [3, 13, 16, 41]. Human perception of tooth colour is very complex and consists of both subjective and objective components. The subjective component of colour is highly variable and dependent on factors such as ambient lighting, the colour of the person’s skin and the distribution/appearance of adjacent teeth. Other potential problems using shade tabs to measure tooth lightness are: some investigators use “non-standard” shade guides; the units are not typically evenly distributed in colour space; they are not as discriminating as the measured colourimeter values and colour matching using a shade guide is subject to clinician variability and bias [26]. Whilst this approach offers a reasonable assessment of the absolute bleaching effect of a product based upon the change from pre-treatment score, the influence of examiner subjectivity and other environmental factors limit its application in comparative research. The use of instrumentation to measure tooth colour has a number of advantages over examiner-based evaluation techniques [26]. More recent studies are based on the use of digital imaging systems to generate L*a*b* values as a means for quantifying tooth colour. This allows direct comparison between products and between different studies as it satisfies the conditions of being an objective, linear and reproducible method [15]. Compared with electronic devices such as spectrophotometers and colourimeters, digital photography, when used for the assessment of tooth colour and the outcome of bleaching procedures as done in the present study, has an additional advantage in that there are numeric data that can be evaluated as well as an image [5, 6, 36]. However, as shown by Yap et al. [50], one should be aware that discrepancy exists between human-eye and computerised colourimetric colour matching.
The method applied in the present study was firstly described by Bengel [5]. The procedure uses digital images that are analysed with commercial software (Adobe Photoshop®). Use of the software allows for objective, linear and quantitative evaluating of colour change. Together with the fact that the images were taken under standardised ambient conditions, adjustment of the images to the applied gray card patches ensured standardisation of the analysis. Using this method, it was shown that both bleaching systems improved tooth colour significantly (p ≤ 0.05) compared to baseline during 12-day active phase of bleaching therapy without distend difference between the groups. The difference between the both bleaching systems could be explained by the different kinetics of hydrogen peroxide and carbamide peroxide.
The hydrogen peroxide concentration of the two tested bleaching regimes was quite similar. However, VW was applied twice a day for 30 min each, OP only once, for 3–4 h. Hydrogen peroxide, released from the carbamide compound, is metabolised by catalase, peroxidase and hydro peroxidase in saliva and oral tissue [19]. In the bleaching process, carbamide peroxide reacts with water to release hydrogen peroxide, which in turn liberates free oxygen radicals to produce a whitening effect [21]. The results of the present study shows that the two differently formulated gels with nearly similar hydrogen peroxide concentration were equally effective with respect to tooth whitening.
Dental bleaching has been reported to cause a number of side effects, including tooth hypersensitivity, gingival irritation, tooth pain, tingling of the tissues and sore throat [4, 7, 24, 25, 31, 40, 45]. The most common side effects are tooth hypersensitivity and gingival irritation. These effects are correlated with the peroxide concentration of the bleaching gel, with the number and length of daily applications, pH of the whitening solution and other factors [17, 18, 32]. Dental hypersensitivity may be a result of penetration of bleaching agents into the pulp chamber resulting in transient inflammatory reactions [10, 32, 48]. Furthermore, dehydration of the teeth during application of bleaching gels is also proposed as a reason for dental hypersensitivity [1]. All of the observed and the majority of reported oral adverse effects were mild and transient in nature [7, 33]. Haywood et al. [25] observed hypersensitivity in 52% of the cases and gingival irritation in 31%. Extensive toxicological studies have been published to examine the safety of hydrogen peroxide or carbamide peroxide for tooth whitening and concluded that 10% carbamide peroxide (equivalent to 3.6% hydrogen peroxide), when applied in a mouth tray, is safe [22, 33, 34]. In the present study, the identification of patients with hypersensitivities was determined with an air stimulus. This approach has proven to be a reliable method for evaluation of the intensity of hypersensitivity [27, 43]. Degree of tooth hypersensitivity was reported by the patient using a scale from “0” to “10” (0—no hypersensitivity, 10—high hypersensitivity). This assessment method for grading of tooth hypersensitivity has been applied in previous studies and presents a reliable tool for determining tooth hypersensitivity [27]. To get more information about the time profile of the degree of hypersensitivity, the patients were instructed to check the tooth hypersensitivity with cold water daily. In addition, the subjects documented the hypersensitivity in a pain diary. Like in recent studies, all of the observed and the majority of reported oral adverse effects were mild and transient in nature. The intensity of tooth sensitivities after bleaching increased more in the Opalescence group, but the difference between the groups was not significant. In the literature, no comparable studies with highly concentrated tray-based bleaching systems are available. Nevertheless, the safety data from this study correlates well with that previously reported in the literature for lower concentrated regimes and further supports the favourable tolerability of peroxide based at-home bleaching products [25, 40, 45].
No statistically significant differences were observed between both treatment groups with respect to subject-perceived tooth hypersensitivity or gum irritation. In all cases, erythema or desquamation of the papilla correlated to areas covered by the bleaching tray. This type of irritation is common to tray-based systems representing mechanical compression of the papilla as reported elsewhere.
Nevertheless, the two highly concentrated systems showed degrees of side effects, which were similar to the levels reported for lower concentrated regimes.
However, in both groups, majority of the subjects stated that the bleaching regimen was comfortable or only slightly disturbing (76.7%). The majority of subjects from both groups were willing to repeat the bleaching therapy or recommend it to friends (VW, 77.8%, OP, 62.1%).
Conclusions
In conclusion, both highly concentrated bleaching systems are effective as tooth-whitening systems, with few reported side effects such as transient tooth hypersensitivity.
The bleaching systems demonstrated significant tooth colour improvement for Δb* and ΔL*. They did produce significantly different whitening response for Δb*, with OP showing significant higher Δb*. After bleaching therapy, the intensity of tooth hypersensitivity was increased significantly compared to baseline, with no significant difference between the both groups.
References
Attin T, Paque F, Ajam F, Lennon AM (2003) Review of the current status of tooth whitening with the walking bleach technique. Int Endod J 36:313–329
Auschill TM, Hellwig E, Schmid S, Hannig M, Arweiler NB (2002) Efficacy of different bleaching techniques and their effect on enamel surface. Schweiz Monatsschr Zahnmed 112(9):894–900 (in German)
Barlow A, Gerlach RW, Date RF, Brennan K (2003) Clinical response of two brush-applied peroxide whitening systems. J Clin Dent 14(3):59–63
Barnes DM, Kihn PW, Romberg E, George D, De Paola L, Medina E (1998) Clinical evaluation of a new 10% carbamide peroxide tooth-whitening agent. Compend Contin Educ Dent 19(10):968–978
Bengel WM (2003) Digital photography and the assessment of therapeutic results after bleaching procedures. J Esthet Restor Dent 15(Suppl 1):21–32
Bentley C, Leonard RH, Nelson CF, Bentley SA (1999) Quantitation of vital bleaching by computer analysis of photographic images. J Am Dent Assoc 130:809–816
Christensen GJ (1998) Bleaching teeth: report of a survey, 1997. J Esthet Dent 10(1):16–20
Collins LZ, Maggio B, Gallagher A, York M, Schäfer F (2004) Safety evaluation of a novel whitening gel, containing 6% hydrogen peroxide and a commercially available whitening gel containing 18% carbamide peroxide in an exaggerated use clinical study. J Dent 32:47–50
Commission Internationale de L’Eclairage (1978) Recomendations on uniform colour spaces. Colour difference equations. Psychometric colour terms. Paris, France: Bureau Central de la CIE, Suppl 2 to CIE pub 14 (E-13.1) 1971/ (TC-1.3)
Cooper JS, Bokmeyer TJ, Bowles WH (1992) Penetration of the pulp chamber by carbamide peroxide bleaching agents. J Endod 18(7):315–317
Dunn JR (1998) Dentist-prescribed home bleaching: current status. Compend Contin Educ Dent 19(8):760–764
Feinmann RA, Madry G, Yarborough D (1991) Chemical, optical and physiologic mechanisms of bleaching products. Pract Periodontics Aesthet Dent 3:32–37
Garcia-Godoy F, Villalta P, Bartizek RD, Barker ML, Biesbrock AR (2004) Tooth whitening effects of an experimental power whitening toothbrush relative to an 8.7% hydrogen peroxide paint-on gel control. Am J Dent 17:25–30
Gegauff AG, Rosenstiel SF, Langhout KJ, Johnston WM (1993) Evaluating tooth colour change from carbamide peroxide gel. J Am Dent Assoc 124(6):65–72
Gerlach RW, Barker ML, Sagel PA (2003) Objective and subjective whitening reponse of two self-directed bleaching systems. Am J Dent 15:7A–12A
Gerlach RW, Barker ML (2003) Clinical response of three direct-to-consumer whitening products: strips, paint-on gel, and dentifrice. Compend Contin Educ Dent 24(6):458–465
Gerlach RW, Gibb RD, Sagel PA (2000) A randomized clinical trial comparing a novel 5.3% hydrogen peroxide whitening strip to 10%, 15%, and 20% carbamide peroxide tray-based bleaching systems. Compend Contin Educ Dent 29:22–28
Gerlach RW, Zhou X (2001) Vital bleaching with whitening strips: summary of clinical research on effectiveness and tolerability. J Contemp Dent Pract 2(3):1–16
Hannig C, Zech R, Henze E, Dorr-Tolui R, Attin T (2003) Determination of peroxides in saliva—kinetics of peroxide release into saliva during home bleaching with Whitestrips and Vivastyle in vivo. Arch Oral Biol 48:559–568
Haywood VB (1991a) Overview and status of mouth guard bleaching. J Esthet Dent 3(5):157–161
Haywood VB (1991b) Nightguard vital bleaching: a history and product update. Esthet Dent Update 2(4):63–66
Haywood VB (1994) Considerations and variations of dentist-prescribed, home-applied vital tooth-bleaching techniques. Compend Contin Educ Dent 15(Suppl 17):616–621
Haywood VB, Heymann HO (1991) Nightguard vital bleaching, how safe is it? Quintessence Int 22(7):515–523
Haywood VB, Leonard RH, Dickinson GL (1997) Primarily research. Efficacy of six months of nightguard vital bleaching of tetracycline-stained teeth. J Esthet Dent 9(1):13–19
Haywood VB, Leonard RH, Nelson CF, Brunson WD (1994) Effectiveness, side effects and long-term status of nightguard vital bleaching. J Am Dent Assoc 125(9):1219–1226
Horn DJ, Bulan-Brady J, Hicks ML (1998) Sphere spectrophotometer versus human evaluation of tooth shade. J Endod 24(12):786–790
Kielbassa AM, Attin T, Hellwig E, Schade-Brittinger C (1997) In vivo study on the effectiveness of a lacquer containing CaF2/NaF in treating dentine hypersensitivity. Clin Oral Investig 1(2):95–99
Kugel G, Kastali S (2000) Tooth-whitening efficacy and safety: a randomized and controlled clinical trial. Compend Contin Educ Dent 29:16–21
Kwon YH, Huo MS, Kim KH, Kim SK, Kim YJ (2002) Effects of hydrogen peroxide on the light reflectance and morphology of bovine enamel. J Oral Rehabil 29(5):473–477
Lenhard M (1996) Assessing tooth colour change after repeated bleaching in vitro with 10% carbamide peroxide gel. J Am Dent Assoc 127(11):1618–1624
Leonard RH Jr, Haywood VB, Eagle JC, Garland GE, Caplan DJ, Matthews KP, Tart ND (1999) Nightguard vital bleaching of tetracycline-stained teeth: 54 months post treatment. J Esthet Dent 11(5):265–277
Leonard RH, Haywood VB, Philipps C (1997) Risk factors for developing tooth sensitivity and gingival irritation associated with nightguard vital bleaching. Quintessence Int 28(8):527–534
Li Y (2000) Peroxide-containing tooth whiteners: an update on safety. Compend Contin Educ Dent 21(Suppl 28):4–9
Marshall MV, Cancro LP, Fischman SL (1995) Hydrogen peroxide: a review of its use in dentistry. J Periodontol 66(9):786–796
Matis BA, Wang Y, Jiang T, Eckert GJ (2002) Extended at-home bleaching of tetracycline-stained teeth with different concentrations of carbamide peroxide. Quintessence Int 33(9):645–655
Mc Caslin AJ, Haywood VB, Potter BJ, Dickenson GL, Russell CM (1999) Assessing dentin color changes from nightguard vital bleaching. J Am Dent Assoc 130:1485–1490
McEvoy SA (1989) Chemical agents for removing intrinsic stains from vital teeth. II. Current techniques and their clinical application. Quintessence Int 20(5):379–384
Mokhlis GR, Matis BA, Cochran MA, Eckert GJ (2000) A clinical evaluation of carbamide peroxide and hydrogen peroxide whitening agents during daytime. J Am Dent Assoc 131(9):1269–1277
Moraes RR, Marimon JL, Schneider LF, Correr Sobrino L, Camacho GB, Bueno M (2006) Carbamide perocide bleaching agents: effects on surface roughness of enamel, composite and porcelain. Clin Oral Investig 10:23–28
Nathanson D (1997) Vital tooth bleaching: sensibility and pulpal considerations. J Am Dent Assoc 128:41–44
Nathoo S, Stewart B, Petrone M, Chaknis P, Zhang YP, DeVizio W, Volpe AR (2003) Comperative clinical investigation of the tooth whitening efficacy of tow tooth whitening gels. J Clin Dent 14(3):64–69
Niedermann R, Tantraphol MC, Slinin P, Hayes C, Conway S (2000) Effectiveness of dentist-presecribed, home-applied tooth whitening. A meta analysis. J Contemp Dent Pract 15:20–36
Orologio GD, Lorenzi RL, Anselmi M, Opisso V (1999) Dentin desensitizing effects of gluma alternate, health-dent desensitizer and scotchbond multi-purpose. Am J Dent 12:103–106
Papathanasiou A, Barwell D, Kugel G (2001) A clinical study evaluating a new chairside and take-home whitening system. Compend Contin Educ Dent 22(4):289–294
Pohjola RM, Browning WD, Hackmann ST, Myers ML, Downey MC (2002) Sensitivity and tooth whitening agents. J Esthet Restor Dent 14(12):85–91
Rosenstiehl SF, Gegauff AG, Johnston WM (1996) Randomized clinical trail of the efficacy and safety of a home bleaching procedure. Quintessence Int 27(6):413–424
Schulte JR, Morrisette DB, Gasior EJ, Czajewski MV (1994) The effects of bleaching application time on the dental pulp. J Am Dent Assoc 125(10):1330–1335
Thitinanthapan W, Satomont P, Vongsavan N (1999) In vitro penetration of the pulp chamber by three brands of carbamide peroxide. J Esthet Dent 11(5):259–264
Wiegand A, Vollmer D, Foitzik M, Attin R, Attin T (2005) Efficacy of different whitening modalities on bovine enamel and dentin. Clin Oral Investig 9:91–97
Yap AU, Sim CP, Loh WL, Teo JH (1999) Human-eye versus computerized colour matching. Oper Dent 24(6):358–363
Acknowledgement
This study was supported by Kettenbach (Eschenburg, Deutschland).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ziebolz, D., Helms, K., Hannig, C. et al. Efficacy and oral side effects of two highly concentrated tray-based bleaching systems. Clin Oral Invest 11, 267–275 (2007). https://doi.org/10.1007/s00784-007-0108-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-007-0108-1