
Abstract
Total elevated plasma homocysteine (Hcy) is a risk factor for thromboembolism. Vascular endothelium is important to regulate coagulation, but the impact of Hcy on the clot-promoting activity (CPA) of endothelial cells has not been fully understood. In our study, human umbilical vein endothelial cells (HUVECs) were treated with Hcy (8, 20, 80, 200, 800 μmol/L) for 24 h. Annexin V was utilized to detect phosphatidylserine (PS) externalization and endothelial microparticles (MPs) formation. CPA was assessed by recalcification time and purified clotting complex tests. We found that Hcy enhanced the externalized PS and consequent CPA of HUVECs in a dose-dependent fashion, effect of Hcy had statistical significance at 800 μmol/L. In addition, Hcy also increased the shedding of procoagulant endothelial MPs. Blocking of PS with 128 nmol/L annexin V reduced approximately 70% CPA of HUVECs and endothelial MPs, but human anti-tissue factor antibody had little inhibitive effect. Our results showed that Hcy increased CPA of HUVECs via PS externalization and MPs release. Our present study has implications for hyperhomocysteinemia-related hypercoagulability.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Homocysteine (Hcy) is a sulfur-containing amino acid generated during methionine metabolism (Currò et al. 2009; Cai et al. 2009). Enhanced levels of plasma Hcy caused by dietary, hormonal, metabolic, toxic or genetic factors (McCully 2007) are positively correlated with an increased risk of thrombosis (den Heijer et al. 2007; Dayal et al. 2006). But the precise mechanism of Hcy-related thromboembolic events has not been clearly established.
Endothelium spreading the blood vessels in every tissue maintains an anticoagulant potential under normal conditions (Cines et al. 1998). However, after exposure to Hcy, vascular endothelial cells (ECs) possess procoagulant phenotype. Probable reasons include induction of tissue factor (TF) and factor V activity (Fryer et al. 1993; Rodgers and Kane 1986), down-regulation of protein C activation, thrombomodulin and von Willebrand factor synthesis (Rodgers and Conn 1990; Lentz and Sadler 1991, 1993), reduction of heparan sulfate expression (Nishinaga et al. 1993), and inhibition of tissue plasminogen activator binding to ECs (Hajjar 1993). In addition, endothelial microparticles (MPs), and small plasma membrane MPs derived from endothelium (Piccin et al. 2007), have been proposed to be involved in thrombogenesis (Chirinos et al. 2005).
Phosphatidylserine (PS) sequesters on the inner side of the cellular membrane bilayer, but it redistributes to the outer surface during cell apoptosis or activation (Shi et al. 2006). Apoptotic cells also release MPs with PS exposure on their surface (Fu et al. 2010). Besides, PS is essential for promoting membrane binding and catalytic activity of tenase (FIXa/FVIIIa) and prothrombinase (FXa/FVa) complexes in the cascade that leads to the production of thrombin (Zwaal and Schroit 1997). Therefore, we aimed to investigate the relationship between endothelial MPs shedding as well as PS externalization and Hcy-induced CPA of ECs.
Annexin V—also described as vascular anticoagulant-alpha, anchorin C II, placental anticoagulant protein I, placental protein 4, lipocortin V, calphobindin I, thromboplastin inhibitor and endonexin II (Tait et al. 1991)—binds to PS most efficiently (Brumatti et al. 2008). This protein forms two-dimensional crystals to shield the procoagulant phospholipids (Reviakine et al. 1998), so it has potent anticoagulant properties (Andree et al. 1992). In view of these facts, we used annexin V to study Hcy-associated CPA of ECs.
Materials and methods
Materials
Hcy, fluoresceine isothiocyanate (FITC)-annexin V apoptosis detection kit with propidium iodide (PI), bovine serum albumin (BSA), ethylenediaminetetraacetic acid (EDTA) and trypsin solution were from Sigma-Aldrich (St Louis, MO, USA). FluoSpheres 1 μm polystyrene microspheres were obtained from Invitrogen (Carlsbad, CA, USA). Human umbilical vein endothelial cells (HUVECs), poly-l-lysine and complete endothelial cell medium were from Sciencell (San Diego, CA, USA). Human prothrombin, thrombin, factors Va, VIIa, IXa, X and Xa were from Haematologic Technologies Inc. (Burlington, VT, USA). Recombinant human factor VIII, polyclonal antibody (Ab) against human tissue factor (TF) and FITC-conjugated anti-human TF Ab were purchased from American Diagnostica Inc. (Stamford, CT, USA). The Chromogenix substrate S-2238 and S-2765 were obtained from DiaPharma Group (West Chester, OH, USA). Purified recombinant annexin V and FITC mouse IgG1 isotype control were from BD Biosciences (San Jose, CA, USA).
Cell culture and treatment
A total of 2 × 105 HUVECs (2–4 passages), seeded in poly-l-lysine coated T-25 flasks, were cultured in 5-mL complete endothelial cell medium at 37°C under a 5% CO2 humidified atmosphere. The confluent cells at 2-day in culture were treated with various concentrations of Hcy (8–800 μmol/L) for 24 h.
Endothelial MPs preparation
By a previously described method (Combes et al. 1999), culture media from flasks were harvested and cleared from HUVECs fragments by centrifugation (4,300×g, 5 min). After high-speed centrifugation (100,000×g, 90 min, 10°C) of the supernatants by ultracentrifuge (HITACHI GX SERIES HIMAC CS 120 GXL, Japan), pelleted endothelial MPs were resuspended in 100 μL of Tyrode’s buffer (137 mmol/L NaCl, 2.7 mmol/L KCl, 11.9 mmol/L NaHCO3, 0.42 mmol/L NaH2PO4, 1 mmol/L MgCl2, 2 mmol/L CaCl2, 5.5 mmol/L glucose, 5 mmol/L Hepes and 0.35% BSA, pH 7.4) and utilized immediately.
Flow cytometry
To detect PS externalization and TF expression on the cell surface, 5 × 105 HUVECs were incubated with 10 μL of FITC-IgG1 isotype control or FITC-annexin V (15 min) or FITC-anti-TF Ab (30 min) in the dark (Fu et al. 2010) before the addition of 10 μL PI solution. Samples were analyzed by flow cytometry (FACSAria, Becton–Dickinson, USA). We used FCS express V3 (De Novo Software, Los Angeles, CA, USA) to analyze the results.
MPs are less than 1 μm and PS positive (Fu et al. 2010). Endothelial MPs formation was quantified as follows, 100 μL of MPs-containing buffer was incubated with 10 μL of FITC-annexin V for exactly 30 min in the dark. After addition of 400 μL Tyrode’s buffer including a known amount of 1 μm yellow-green fluorescent beads, MPs were counted on the flow cytometer.
Confocal microscopy
To locate PS, suspended HUVECs were incubated with FITC-annexin V and PI followed by washing. The samples were excited with 488 nm emission line of a krypton–argon laser, and narrow bandpass filters were used to restrict emission wavelength overlap. Images were captured by Zeiss LSM 510 Meta confocal microscope (Carl Zeiss Jena GmbH, Jena, Germany).
Scanning electron microscopy
Human umblical vein endothelial cells on coverslips were fixed with 2.5% glutaraldehyde-phosphate fixative. After washing with 0.1 mol/L Na-cacodylate HCl buffer, samples were postfixed in 1% OsO4 and dehydrated. Then, platinum (10-nm thick) was sprayed on the cells. We viewed images on a S-3400 N Scanning Electron Microscope (Hitachi Ltd., Tokyo, Japan) by an ultra-high-resolution mode.
Coagulation time and inhibition tests
Clotting time was evaluated by a one-step recalcification time test (Zhou et al. 2010). Suspensions of 100 μL HUVECs (1 × 105 cells in Tyrode’s buffer) or endothelial MPs were incubated with 100 μL of MPs-free plasma obtained using ultracentrifugation, as previously described (Taube et al. 1999) (anticoagulated with 3.8% sodium citrate, 1:9, v/v), for 180 s at 37°C. After the addition of preheated 25 mmol/L CaCl2 (100 μL), the time to fibrin strand generation was recorded by an Amelung KC4A coagulometer (Labcon, Heppenheim, Germany). Annexin V (128 nmol/L) or anti-TF Ab (40 μg/mL) was used to inhibit the plasma clotting reaction.
Factor Xa, prothrombinase tests and inhibition assays
The activation of intrinsic factor Xa in the presence of HUVECs was carried out as follows (Fu et al. 2010). Cells (1 × 105) were mixed with 1 nmol/L factor IXa, 5 nmol/L factor VIII, 0.2 nmol/L thrombin, 130 nmol/L factor X and 5 mmol/L CaCl2 in factor Xa buffer (8.8 mL ddH2O, 1 mL 10 × TBS, 200 μL 10% BSA). The reaction was stopped by 7 mmol/L EDTA. After incubation with 10 μL of S-2765 (0.8 mmol/L), factor Xa generation was measured immediately at 405 nm on a BioTek Microplate Reader (Winooski, VT, USA). For extrinsic factor Xa production, cells were incubated with 1 nmol/L factor VIIa, 130 nmol/L factor X and 5 mmol/L CaCl2. Factor Xa formation was obtained after the addition of 0.8 mmol/L S-2765. For the prothrombinase assay, the samples were mixed with 1 nmol/L factor Va, 0.05 nmol/L factor Xa, 1 μmol/L prothrombin and 5 mmol/L CaCl2 in prothrombinase buffer (8.95 mL ddH2O, 1 mL 10× TBS, 50 μL 10% BSA). Thrombin production was determined using S-2238 (0.8 mmol/L). Inhibition tests of thrombin generation were followed by a supplement of varying doses of annexin V (0–128 nmol/L).
Statistical analysis
Results with at least three replicates were presented as mean ± SD, and were analyzed with paired Student’s t-test. P < 0.05 was considered to be statistically significant.
Results
Measurement of PS and TF on HUVECs and MPs counts
Different concentrations of Hcy, similar to those detected in the blood of healthy individuals or patients with hyperhomocysteinemia (Hankey and Eikelboom 1999) were chosen to treat HUVECs in vitro for 24 h. Both PS and TF are important factors of the coagulation cascade (Zwaal and Schroit 1997; Butenas et al. 2009). FITC-Annexin V and FITC-anti-TF Ab were incubated with HUVECs separately before addition of PI. Hcy-untreated ECs were used as control. Using flow cytometry, Hcy elevated the binding of annexin V to HUVECs in a dose-dependent manner, with statistical significance at 800 μmol/L of Hcy (Fig. 1a). Binding of anti-TF Ab to HUVECs and the extent of late apoptotic cells (annexin V+, PI+) were increased slightly, but no statistical significance. In addition, Hcy dose-dependently enhanced the amount of endothelial MPs, 800 μmol/L of Hcy, with statistical significance (Fig. 1b).

PS, TF on HUVECs and counts of endothelial MPs by flow cytometry. HUVECs were treated with indicated concentrations of Hcy for 24 h. a Cells were stained with green fluorescent proteins and PI. Annexin V+, anti-TF Ab+ or annexin V+/PI+ percent of cells were determined using flow cytometry. Hcy-untreated cells were used as control HUVECs. b MPs of 5 mL culture supernatants in T-25 flasks were collected, labeled with FITC-annexin V. Endothelial MPs were smaller than 1 μm and binding to annexin V. The numbers of endothelial MPs were obtained
Location of PS on HUVECs
Confocal microscope was utilized to identify PS exposure on HUVECs. Suspended HUVECs were collected followed by co-staining with FITC-annexin V (green) and PI (red). Almost no labeling of FITC-annexin V was detected on the surface of control HUVECs (Fig. 2a). However, membranes of partial cells in the early apoptotic stage (annexin V+, PI−) were green after treatment of 800 μmol/L Hcy for 24 h (Fig. 2b). The nuclei of a few HUVECs were labeled with red fluorescence, indicating that integrity of the cell membrane was compromised (Fu et al. 2010) and those ECs entered late apoptotic stage.

Confocal microscopy of PS exposure on suspended HUVECs surface. The bright phase of HUVECs (left). Cells were co-stained with FITC-annexin V and PI (right). a The control HUVECs. b HUVECs were exposed to 800 μmol/L Hcy for 24 h. The membrane of HUVECs displayed green when labeled by FITC-annexin V. A cell nucleus was red when stained by PI (arrow). Bars represent 10 μm
Hcy-induced endothelial MPs release from HUVECs
Microparticles are cell membrane submicron-sized vesicles generated from apoptotic or activated cells (Chironi et al. 2009). Endothelial MPs result from vesiculation of ECs. In our study, we exposed HUVECs to 800 μmol/L Hcy for 24 h. Scanning electron microscopy evidenced HUVECs membrane-shed blebs (smaller than 1 μm), suggesting endothelial MPs could be induced by Hcy in vitro (Fig. 3b).

Ultrastructure of HUVECs and endothelial MPs. HUVECs (stars) were analyzed by scanning electron microscopic examination. a The control HUVEC. b The HUVEC was treated with 800 μmol/L Hcy for 24 h. Endothelial MPs (arrow) were smaller than 1 μm. Bar represents 1 μm
CPA of HUVECs and endothelial MPs
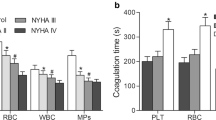
Increased CPA of cells and endothelial MPs were evaluated by decreased recalcification time. HUVECs and MPs showed enhanced CPA which paralleled the increasing Hcy concentrations (Fig. 4a). The decrement of clotting time was significant at 800 μmol/L of Hcy for HUVECs, but 200 μmol/L of Hcy for endothelial MPs. By coagulation complex tests, we found the positive effects of Hcy-treated HUVECs on the conversions of factor X and prothrombin to factor Xa and thrombin, respectively, in a dose-dependent fashion. This increment of intrinsic factor Xa and thrombin productions was especially significant at 800 μmol/L of Hcy (Fig. 4b).

Clotting time and enzyme complexes assays. HUVECs were incubated with various doses of Hcy for 24 h, cells and MPs were harvested. a Recalcification time of HUVECs (1 × 105) and endothelial MPs (prepared from 5 mL culture media in T-25 flasks) were the time to the formation of fibrin strand. b Extrinsic FXa, intrinsic FXa and thrombin production of HUVECs were evaluated at 405 nm in a kinetic microplate reader
Coagulation inhibition assays of HUVECs and endothelial MPs
In the following experiments, we carried out inhibition tests of coagulation to explore the impact of PS and TF on the CPA of both HUVECs and endothelial MPs. CPA of 800 μmol/L Hcy-treated HUVECs for 24 h and harvested MPs were effectively inhibited using 128 nmol/L annexin V, but 40 μg/mL anti-TF Ab had no significant impact (Fig. 5a). Subsequently, using inhibition tests of clotting complexes, we found that formation of FXa and thrombin gradually reduced with raised concentrations of annexin V. By 128 nmol/L annexin V, 60% of intrinsic FXa generation was inhibited (Fig. 5b), while about 70% of extrinsic FXa and thrombin production were inhibited (Fig. 5c, d). These data indicated that PS is important for the CPA of Hcy-treated HUVECs.

Inhibition tests of coagulation time and complexes. After treatment with 800 μmol/L Hcy for 24 h, HUVECs and endothelial MPs were collected. a Clotting time of cells, MPs, and Tyrode’s buffer were measured in the absence or presence of anti-TF Ab (40 μg/mL) or annexin V (128 nmol/L). b–d Intrinsic FXa, extrinsic FXa and thrombin formation of control cells or 800 μmol/L Hcy-treated HUVECs were determined in the presence of increasing concentrations of annexin V (0–128 nmol/L)
Discussion
In an adult human body, about 1–6 × 1013 ECs cover approximately 1–7 m2 surface area (Cines et al. 1998). Quiescent ECs are crucial to present an antithrombotic membrane, but perturbed endothelium by chemical or physical factors provides prothrombotic surface (Cines et al. 1998). Endothelial MPs can also initiate thrombosis and partake in the hypercoagulable state of various prothrombotic abnormalities (Chironi et al. 2009). Our present study demonstrated that Hcy exerted effect on cultured ECs and consequently induced CPA through PS externalization and MPs generation.
Plasma total Hcy ranges from 5 to 15 μmol/L in healthy adults (Perła-Kaján et al. 2007), and higher values are classified as moderate (16–30 μmol/L), intermediate (31–100 μmol/L) and severe (>100 μmol/L) hyperhomocysteinemia (Hankey and Eikelboom 1999). However, most of the previous experiments showed that high concentration of Hcy, about 1–10 mmol/L, enhanced CPA of ECs (Fryer et al. 1993; Rodgers and Kane 1986; Rodgers and Conn 1990; Lentz and Sadler 1991, 1993; Nishinaga et al. 1993; Hajjar 1993). These concentrations of Hcy used were much in excess of the concentrations of total Hcy in hyperhomocysteinemia, making the interpretation of the physiopathologic significance of these studies difficult (Thambyrajah and Townend 2000). Our present study showed that Hcy led to procoagulant phenotype of HUVECs and endothelial MPs release via activation of clotting enzyme complexes. Moreover, the concentrations of Hcy we used here were similar to those found in the patients with hyperhomocysteinemia, so our results had potential physiological and clinical importance.
Hcy induces apoptosis in HUVECs via unfolded protein response activation (Zhang et al. 2001), Fas-mediated pathways upregulation (Suhara et al. 2004), p53-dependent Noxa expression upregulation (Lee et al. 2005) and NADPH oxidase/JNK signaling-dependent mechanism (Dong et al. 2005). Those apopototic characteristics include nuclear condensation and fragmentation, internucleosomal DNA fragmentation and hypoploid DNA contents. The methods used to detect the aforementioned apoptotic features consume time, provide non-specific results, and usually destruct the cell integrity (Zhang et al. 1997). However, translocation of PS from the internal to the external cell surface occurs earlier than the nuclear changes correlated with apoptosis. Thus we quantitatively (using flow cytometry) and qualitatively (using confocal microscopy) monitored PS exposure to evaluate Hcy-induced apoptosis of HUVECs. We found that annexin V, the commonly used PS probe (Brumatti et al. 2008), accurately measured the exposed PS on HUVECs and the counts of endothelial MPs. Besides, PS is reported to partake in coagulation abnormalities of some diseases (Fu et al. 2010; Zhou et al. 2009, 2010; Hou et al. 2011). But little was known about the relationship between PS externalization and Hcy-associated hypercoagulable state. In our current study, annexin V effectively inhibited 70% thrombin production and consequently reduced CPA of HUVECs and endothelial MPs. These results indicated that PS was important for ECs CPA after exposure to Hcy.
Endothelial damage results in TF exposure and initiates extrinsic clotting pathway (Nachman 1992). Relatively, most TF exposure is encrypted and has little CPA, but TF gains procoagulant function through activation by exteriorized PS (Bach 2006). Using flow cytometry, significant rise of TF levels was not detected. We also found that anti-TF Ab could not sufficiently inhibit CPA of Hcy-treated HUVECs or collected endothelial MPs, indicating that TF was not the main factor for Hcy-increased CPA of HUVECs or endothelial MPs. Previous studies showed that TF takes part in the Hcy-related CPA of ECs (Fryer et al. 1993). As most activity of the TF-factor VIIa was inhibited by annexin V, we speculated that the increased TF activity of HUVECs treated by Hcy was PS-dependent.
Thrombin-mediated fibrinogen conversion to fibrin and fibrin cross-linked by factor XIIIa results in generation of a fibrin clot. Continuous editing of Hcy by methionyl-tRNA synthetases leads to the generation of Hcy-thiolactone (Jakubowski 2011). The prothrombotic effects of increased plasma Hcy on clot permeability and lysis in humans are in line with a mechanism involving Hcy-thiolactone-modified fibrinogen (Undas et al. 2006). In cystathionine β-synthase-deficient patients, significantly elevated prothrombotic N-Hcy-fibrinogen in plasma possibly accounts for the enhanced thrombogenesis of these patients (Jakubowski et al. 2008). Furthermore, fibrin clots generated from Hcys-fibrinogen-albumin have a similar decreased ability to support activation of plasminogen, and a similar fibrinolytic resistance as Hcys-fibrinogen formed clots (Sauls et al. 2011). Our current results showed that PS increment elevated thrombin production of Hcy-treated ECs. So the data described in our paper provided additional evidence for the mechanisms involved in Hcy-associated thrombogenesis. Hcy-thiolactone also induces cell death in HUVECs (Mercié et al. 2000; Kerkeni et al. 2006). Further research should focus on the effect of PS and endothelial MPs on Hcy metabolites-induced prothrombotic properties of ECs.
Moreover, fibrinolysis is initiated when plasminogen and tissue plasminogen activator (t-PA) attach to the fibrin clot (Sauls et al. 2011). ECs modulate fibrinolytic system through synthesis and secretion of t-PA and plasminogen activator inhibitor-1 (PAI-1) (Perła-Kaján et al. 2007). Accumulated evidence suggests that Hcy modifies annexin II and inhibits annexin II-mediated t-PA-dependent plasminogen activation in vitro and in vivo (Hajjar 1993, 1998; Jacovina et al. 2009). Thus, Hcy might disturb the EC surface fibrinolysis (Hajjar and Jacovina 1998). Besides, PS activates EC-type PAI-1 and may be essential for the fibrinolytic system (Lambers et al. 1987). Therefore, the procoagulant and fibrinolytic alterations of ECs may simultaneously contribute to the Hcy-related thrombosis.
In conclusion, we demonstrate that the increased PS externalization and endothelial MPs formation are the important factors for Hcy-induced procoagulant properties of ECs. Our study increases understanding of the mechanisms of Hcy-associated thrombotic events. Moreover, annexin V is an useful probe to detect PS and could be developed as an anticoagulant to prevent the development of hyperhomocysteinemia-related hypercoagulability.
References
Andree HA, Stuart MC, Hermens WT, Reutelingsperger CP, Hemker HC, Frederik PM, Willems GM (1992) Clustering of lipid-bound annexin V may explain its anticoagulant effect. J Biol Chem 267:17907–17912
Bach RR (2006) Tissue factor encryption. Arterioscler Thromb Vasc Biol 26:456–461
Brumatti G, Sheridan C, Martin SJ (2008) Expression and purification of recombinant annexin V for the detection of membrane alterations on apoptotic cells. Methods 44:235–240
Butenas S, Orfeo T, Mann KG (2009) Tissue factor in coagulation: which? where? when? Arterioscler Thromb Vasc Biol 29:1989–1996
Cai B, Shan L, Gong D, Pan Z, Ai J, Xu C, Lu Y, Yang B (2009) Homocysteine modulates sodium channel currents in human atrial myocytes. Toxicology 256:201–206
Chirinos JA, Heresi GA, Velasquez H, Jy W, Jimenez JJ, Ahn E, Horstman LL, Soriano AO, Zambrano JP, Ahn YS (2005) Elevation of endothelial microparticles, platelets, and leukocyte activation in patients with venous thromboembolism. J Am Coll Cardiol 45:1467–1471
Chironi GN, Boulanger CM, Simon A, Dignat-George F, Freyssinet JM, Tedgui A (2009) Endothelial microparticles in diseases. Cell Tissue Res 335:143–151
Cines DB, Pollak ES, Buck CA, Loscalzo J, Zimmerman GA, McEver RP, Pober JS, Wick TM, Konkle BA, Schwartz BS, Barnathan ES, McCrae KR, Hug BA, Schmidt AM, Stern DM (1998) Endothelial cells in physiology and in the pathophysiology of vascular disorders. Blood 91:3527–3561
Combes V, Simon AC, Grau GE, Arnoux D, Camoin L, Sabatier F, Mutin M, Sanmarco M, Sampol J, Dignat-George F (1999) In vitro generation of endothelial microparticles and possible prothrombotic activity in patients with lupus anticoagulant. J Clin Invest 104:93–102
Currò M, Condello S, Caccamo D, Ferlazzo N, Parisi G, Ientile R (2009) Homocysteine-induced toxicity increases TG2 expression in Neuro2a cells. Amino Acids 36:725–730
Dayal S, Wilson KM, Leo L, Arning E, Bottiglieri T, Lentz SR (2006) Enhanced susceptibility to arterial thrombosis in a murine model of hyperhomocysteinemia. Blood 108:2237–2243
den Heijer M, Willems HP, Blom HJ, Gerrits WB, Cattaneo M, Eichinger S, Rosendaal FR, Bos GM (2007) Homocysteine lowering by B vitamins and the secondary prevention of deep vein thrombosis and pulmonary embolism: a randomized, placebo-controlled, double-blind trial. Blood 109:139–144
Dong F, Zhang X, Li SY, Zhang Z, Ren Q, Culver B, Ren J (2005) Possible involvement of NADPH oxidase and JNK in homocysteine-induced oxidative stress and apoptosis in human umbilical vein endothelial cells. Cardiovasc Toxicol 5:9–20
Fryer RH, Wilson BD, Gubler DB, Fitzgerald LA, Rodgers GM (1993) Homocysteine, a risk factor for premature vascular disease and thrombosis, induces tissue factor activity in endothelial cells. Arterioscler Thromb 13:1327–1333
Fu Y, Zhou J, Li H, Cao F, Su Y, Fan S, Li Y, Wang S, Li L, Gilbert GE, Shi J (2010) Daunorubicin induces procoagulant activity of cultured endothelial cells through phosphatidylserine exposure and microparticles release. Thromb Haemost 104:1235–1241
Hajjar KA (1993) Homocysteine-induced modulation of tissue plasminogen activator binding to its endothelial cell membrane receptor. J Clin Invest 91:2873–2879
Hajjar KA, Jacovina AT (1998) Modulation of annexin II by homocysteine: implications for atherothrombosis. J Investig Med 46:364–369
Hajjar KA, Mauri L, Jacovina AT, Zhong F, Mirza UA, Padovan JC, Chait BT (1998) Tissue plasminogen activator binding to the annexin II tail domain: direct modulation by homocysteine. J Biol Chem 273:9987–9993
Hankey GJ, Eikelboom JW (1999) Homocysteine and vascular disease. Lancet 354:407–413
Hou J, Fu Y, Zhou J, Li W, Xie R, Cao F, Gilbert GE, Shi J (2011) Lactadherin functions as a probe for phosphatidylserine exposure and as an anticoagulant in the study of stored platelets. Vox Sang 100:187–195
Jacovina AT, Deora AB, Ling Q, Broekman MJ, Almeida D, Greenberg CB, Marcus AJ, Smith JD, Hajjar KA (2009) Homocysteine inhibits neoangiogenesis in mice through blockade of annexin A2-dependent fibrinolysis. J Clin Invest 119:3384–3394
Jakubowski H (2011) Quality control in tRNA charging-editing of homocysteine. Acta Biochim Pol 58:149–163
Jakubowski H, Boers GH, Strauss KA (2008) Mutations in cystathionine beta-synthase or methylenetetrahydrofolate reductase gene increase N-homocysteinylated protein levels in humans. FASEB J 22:4071–4076
Kerkeni M, Tnani M, Chuniaud L, Miled A, Maaroufi K, Trivin F (2006) Comparative study on in vitro effects of homocysteine thiolactone and homocysteine on HUVEC cells: evidence for a stronger proapoptotic and proinflammative homocysteine thiolactone. Mol Cell Biochem 291:119–126
Lambers JW, Cammenga M, König BW, Mertens K, Pannekoek H, van Mourik JA (1987) Activation of human endothelial cell-type plasminogen activator inhibitor (PAI-1) by negatively charged phospholipids. J Biol Chem 262:17492–17496
Lee SJ, Kim KM, Namkoong S, Kim CK, Kang YC, Lee H, Ha KS, Han JA, Chung HT, Kwon YG, Kim YM (2005) Nitric oxide inhibition of homocysteine-induced human endothelial cell apoptosis by down-regulation of p53-dependent Noxa expression through the formation of S-nitrosohomocysteine. J Biol Chem 280:5781–5788
Lentz SR, Sadler JE (1991) Inhibition of thrombomodulin surface expression and protein C activation by the thrombogenic agent homocysteine. J Clin Invest 88:1906–1914
Lentz SR, Sadler JE (1993) Homocysteine inhibits von Willebrand factor processing and secretion by preventing transport from the endoplasmic reticulum. Blood 81:683–689
McCully KS (2007) Homocysteine, vitamins, and vascular disease prevention. Am J Clin Nutr 86:1563S–1568S
Mercié P, Garnier O, Lascoste L, Renard M, Closse C, Durrieu F, Marit G, Boisseau RM, Belloc F (2000) Homocysteine-thiolactone induces caspase-independent vascular endothelial cell death with apoptotic features. Apoptosis 5:403–411
Nachman RL (1992) Review: Stratton lecture. Thrombosis and atherogenesis: molecular connections. Blood 79:1897–1906
Nishinaga M, Ozawa T, Shimada K (1993) Homocysteine, a thrombogenic agent, suppresses anticoagulant heparan sulfate expression in cultured porcine aortic endothelial cells. J Clin Invest 92:1381–1386
Perła-Kaján J, Twardowski T, Jakubowski H (2007) Mechanisms of homocysteine toxicity in humans. Amino Acids 32:561–572
Piccin A, Murphy WG, Smith OP (2007) Circulating microparticles: pathophysiology and clinical implications. Blood Rev 21:157–171
Reviakine II, Bergsma-Schutter W, Brisson A (1998) Growth of protein 2-D crystals on supported planar lipid bilayers imaged in situ by AFM. J Struct Biol 121:356–361
Rodgers GM, Conn MT (1990) Homocysteine, an atherogenic stimulus, reduces protein C activation by arterial and venous endothelial cells. Blood 75:895–901
Rodgers GM, Kane WH (1986) Activation of endogenous factor V by a homocysteine-induced vascular endothelial cell activator. J Clin Invest 77:1909–1916
Sauls DL, Warren M, Hoffman M (2011) Homocysteinylated fibrinogen forms disulfide-linked complexes with albumin. Thromb Res 127:576–581
Shi J, Shi Y, Waehrens LN, Rasmussen JT, Heegaard CW, Gilbert GE (2006) Lactadherin detects early phosphatidylserine exposure on immortalized leukemia cells undergoing programmed cell death. Cytometry A 69:1193–1201
Suhara T, Fukuo K, Yasuda O, Tsubakimoto M, Takemura Y, Kawamoto H, Yokoi T, Mogi M, Kaimoto T, Ogihara T (2004) Homocysteine enhances endothelial apoptosis via upregulation of Fas-mediated pathways. Hypertension 43:1208–1213
Tait JF, Frankenberry DA, Shiang R, Murray JC, Adler DA, Disteche CM (1991) Chromosomal localization of the human gene for annexin V (placental anticoagulant protein I) to 4q26–q28. Cytogenet Cell Genet 57:187–192
Taube J, McWilliam N, Luddington R, Byrne CD, Baglin T (1999) Activated protein C resistance: effect of platelet activation, platelet-derived microparticles, and atherogenic lipoproteins. Blood 93:3792–3797
Thambyrajah J, Townend JN (2000) Homocysteine and atherothrombosis-mechanisms for injury. Eur Heart J 21:967–974
Undas A, Brozek J, Jankowski M, Siudak Z, Szczeklik A, Jakubowski H (2006) Plasma homocysteine affects fibrin clot permeability and resistance to lysis in human subjects. Arterioscler Thromb Vasc Biol 26:1397–1404
Zhang G, Gurtu V, Kain SR, Yan G (1997) Early detection of apoptosis using a fluorescent conjugate of annexin V. Biotechniques 23:525–531
Zhang C, Cai Y, Adachi MT, Oshiro S, Aso T, Kaufman RJ, Kitajima S (2001) Homocysteine induces programmed cell death in human vascular endothelial cells through activation of the unfolded protein response. J Biol Chem 276:35867–35874
Zhou J, Liu S, Ma M, Hou J, Yu H, Lu C, Gilbert GE, Shi J (2009) Procoagulant activity and phosphatidylserine of amniotic fluid cells. Thromb Haemost 101:845–851
Zhou J, Shi J, Hou J, Cao F, Zhang Y, Rasmussen JT, Heegaard CW, Gilbert GE (2010) Phosphatidylserine exposure and procoagulant activity in acute promyelocytic leukemia. J Thromb Haemost 8:773–782
Zwaal RF, Schroit AJ (1997) Pathophysiologic implications of membrane phospholipid asymmetry in blood cells. Blood 89:1121–1132
Acknowledgments
This work was supported by grants from the National Basic Research Program of China (973 Program, 2007CB512000/2007CB512006) and National Natural Science Foundation of China (30973532). The authors thank Li Zhang, Yakun Zhang and Jing Li for excellent technical assistance.
Conflict of interest
Authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Additional information
J. Zhu and R. Xie equally contributed to this work.
Rights and permissions
About this article
Cite this article
Zhu, J., Xie, R., Piao, X. et al. Homocysteine enhances clot-promoting activity of endothelial cells via phosphatidylserine externalization and microparticles formation. Amino Acids 43, 1243–1250 (2012). https://doi.org/10.1007/s00726-011-1196-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00726-011-1196-4