
Abstract
Background
Although pancreaticoduodenectomy has been recognized in the past for its severe complications, improvements in operative methods and perioperative management have made it a safe procedure. Therefore, pancreaticoduodenectomy can be performed in elderly patients, and our experience and outcomes are described in this report.
Methods
We retrospectively investigated 142 patients in whom pancreaticoduodenectomy was performed without stenting tubes during pancreaticojejunostomy. The patients were classified into two groups: (A) those older and (B) younger than 75 years. The outcomes, including preoperative characteristics, intraoperative characteristics, postoperative complications and mortality, are herein reported. Continuous variables were compared using Student’s t test and the Chi-square test.
Results
There were no differences between groups A and B in terms of sex, operative time, amount of blood loss, performance status, soft pancreas rate, disease distribution and operative procedure. Comorbidities in groups A and B were statistically different. Regarding the preoperative status, the elderly patients exhibited lower serum albumin and hemoglobin levels than the younger patients. There were no differences in mortality (0 vs. 0 %), morbidity (24.3 vs. 29.5 %, p = 0.362), postoperative hospital days or major complications such as pancreatic fistula development, delayed gastric emptying, intra-abdominal abscess development, biliary fistula formation and postpancreatectomy hemorrhage.
Conclusions
Pancreaticoduodenectomy can be safely performed in elderly as well as younger patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pancreaticoduodenectomy (PD) is the most effective treatment for patients with localized periampullary tumors [1]. In recent years, the safety of PD has improved significantly with respect to surgical technique and perioperative care [2]. However, the development of pancreatic fistula is one of the most common and serious complications that occurs after pancreaticojejunostomy during PD [3].
It is widely accepted that fibrous pancreatic remnants in patients with chronic pancreatitis or pancreatic carcinoma facilitate healing of pancreatic anastomoses. On the other hand, the presence of soft and friable pancreatic parenchyma, frequently found in patients with periampullary cancer and endocrine or cystic lesions, makes it difficult to perform anastomosis [4]. Poon et al. [5] reported that external drainage of the pancreatic duct with a stent reduces the rate of leakage in patients who have undergone pancreaticojejunostomy after PD. On the other hand, pancreatic duct stenting for PD does not decrease the frequency or activity of postoperative pancreatic fistulas [6]. Conversely, pancreaticojejunostomy with duct-to-mucosa anastomosis could be performed more safely without, rather than with, the use of stenting tubes for pancreatic fistula that develop following PD [7–9]. Furthermore, the incidence of short-term complications of PD has been gradually decreasing. Additionally, PD with duct-to-mucosa anastomosis of pancreaticojejunostomy with or without a stenting tube did not differ in a long-term follow-up [10].
Most developed world countries have accepted the age of 65 years as a definition of ‘elderly’ or older person, and people of age 75 or older in Japan are often referred to as the old–old. The old–old are often referred to as frail elderly due to increases in disease and health impairments in later life. Japan’s population is aging. The older population—persons of 65 years or older—in Japan numbered 13.2 million in 2008 and constituted 22.1 % of the population, while the old–old of age 75 years or older accounted for 10.4 % [11].
Until recently, mortality and morbidity following PD in elderly patients were significantly high [12–14]. Therefore, the safety and preservation of the quality of life are the foremost requirements for surgeons performing PD in the elderly. As noted earlier, PD has been aggressively performed in elderly patients coincident with the increasing numbers of elderly in the population.
No reports are available regarding nonstented pancreaticojejunostomy for PD in elderly patients. It is necessary to evaluate the safety of nonstented pancreaticojejunostomy in the elderly with a decreased reserve function.
The aim of this study was to evaluate PD with duct-to-mucosa anastomosis of pancreaticojejunostomy without a stenting tube in the elderly compared with younger patients.
Methods
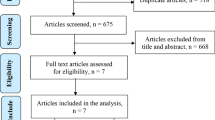
A retrospective study was conducted on a series of 142 consecutive patients with pancreaticobiliary diseases who underwent PD without stenting tubes for duct-to-mucosa pancreaticojejunostomy between 2002 and 2010. The subjects included 37 patients older than 75 years of age (group A) and 105 patients younger than 75 years of age (group B) (Table 1). Preoperative characteristics, intraoperative characteristics, postoperative complications, morbidity and mortality were compared between the two groups. Patients with a PS of 3 or 4 were ineligible for surgical intervention in all generations. If they had an American Society of Anesthesiologists physical status system (ASA) score of 1, 2 or 3 under general operative conditions, PD was performed in all generations.
A “normal soft pancreas” was defined as a pancreas with normal exocrine and endocrine functions with a diameter of the main pancreatic duct <3 mm without apparent fibrosis detected in postoperative pathological specimens. In 48 patients, the presence of pancreatic fistulas in patients whose drain amylase level was measured was defined according to the ISGPF criteria [15]. In 98 patients, before seeing the reports of the ISGPF, the presence of pancreatic fistula was defined according to the criteria of Balcom et al. [16]. The measurable volumes of drain fluid available on and after postoperative day 3 were used to measure the drain amylase levels in all patients. Delayed gastric emptying and postpancreatectomy hemorrhage were also defined according to the definitions proposed by the ISGPS [17, 18].
Operative techniques
Anastomosis between the pancreas and jejunum was performed using end-to-side two-layer anastomosis. Pancreaticojejunostomy without the use of a stenting tube was devised as follows. Anastomosis of the outer layer was performed between the pancreatic parenchyma and jejunal seromuscularis using 3-0 nonabsorbable sutures. Anastomosis between the pancreatic duct and jejunal mucosa was performed precisely using 5-0 or 6-0 monofilament absorbable sutures. With one suture placed in the anterior wall and multiple sutures placed in the bilateral walls, the duct lumen was kept open. Interrupted sutures were placed in the anterior and posterior walls without using a scope. Prophylactic octreotide was not administered postoperatively.
Anastomosis between the jejunum and the stomach or duodenum with antecolic reconstruction was made as straight as possible so as to improve the physical flow until peristalsis improved. All patients underwent reconstruction using modified Child’s methods.
PD was performed in all patients by five different surgeons using the same operative methods. The procedure sought to improve and obtain definitive anastomoses and transection of the pancreas with attention to blood supply at the stump.
Statistical analysis
A comparison between groups A and B was made using the Chi-square test, and the averages were compared using Student’s t test. Differences were considered significant at p < 0.05. Numerical data are expressed as the mean ± SD.
Results
The patient backgrounds are shown in Table 1. There were no differences in sex, operative time, amount of blood loss, performance status, normal pancreas rate, disease distribution or operative procedure between groups A and B. Age differed in both groups according to the study selection design.
The preoperative characteristics before PD are shown in Table 2. There were no differences in body mass index (BMI), total bilirubin levels or creatinine levels between groups A and B. However, the serum albumin and hemoglobin (Hb) levels in group A (albumin 3.6 ± 0.7, Hb 11.9 ± 0.2) were significantly lower than those in group B (albumin 3.8 ± 0.1, Hb 12.9 ± 0.1) (p < 0.05). Additionally, the preoperative complication rate in the elderly group (54.5 %) was significantly higher than that in the younger group (38.1 %).
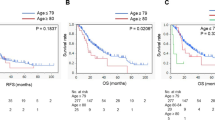
The operative results after PD are shown in Table 3. There were no differences between the older and younger groups in mortality (0 vs. 0 %), morbidity (24.3 vs. 29.5 %, p = 0.362) or postoperative hospital days. There were also no differences between the two groups in major complications such as pancreatic fistula (grade A–C) development, delayed gastric emptying, intra-abdominal abscess development, biliary fistula formation and postpancreatectomy hemorrhage.
Discussion
PD has been increasingly used in the expanding elderly population. In patients with periampullary tumors, PD has been performed for curative resection during each generation. However, weighing the risks and indications for surgical resection is further difficult due to the lack of clinical data on major intra-abdominal surgery in the elderly [13]. Abdominal surgery in elderly patients is associated with a high risk of postoperative complications, and once complications develop, multiple organ failure is likely to ensue [19]. Pancreaticojejunostomy can be safely performed without the use of stenting tubes [8]. Internal stenting of duct-to-mucosa pancreatojejunostomy does not diminish the rate of pancreatic fistula formation or alter overall patient outcomes [8, 9]. It is important to evaluate the use of PD with duct-to-mucosa anastomosis of pancreaticojejunostomy without a stenting tube in the elderly versus younger patients.
In our study, the preoperative complication rate in group A was significantly higher than that observed in group B.
Cameron et al. [20] reported that advanced age is not a factor in predicting either morbidity or mortality and that no differences are observed in elderly patients with respect to preoperative risk factors such as prior myocardial infarction, hypertension, diabetes, chronic obstructive pulmonary disease, peripheral vascular disease and so on. In the same study, no specific complications were more frequent in the older group [21]. In our study, postoperative status was similar in the two groups and no differences were observed in such parameters as operative time, amount of blood loss, hospital days and soft pancreas rate. In addition to the difference in preoperative complications, the levels of serum albumin and hemoglobin were lower in the elderly group than in the younger group. This result indicated that, although the elderly patients had poorer nutrition than the younger patients, BMI did not differ between the two groups. Therefore, postoperative care should be more attentive to these points in elderly patients than in younger patients.
Some reports have shown that morbidity and mortality rates are significantly higher in elderly compared to younger patients [12–14, 22]. On the other hand, Hodul et al. [23] reported that PD can be performed safely in patients 70 years of age or older with morbidity and mortality rates similar to those observed in younger individuals. In addition, Lee et al. [24] compared patients over and under 80 years of age and found no differences in preoperative comorbidity or postoperative morbidity (49.4 vs. 48.9 %) and mortality (4.3 vs. 4.4 %). In our study, neither mortality nor morbidity was significantly different in the elderly and younger patients. The use of duct-to-mucosa anastomosis without stenting tubes appears to be associated with lower rates of pancreatic fluid leakage and fistula formation, which has been confirmed by other centers that have used the same procedure [6, 8, 9]. However, in the absence of comparative studies of stenting techniques, conclusions regarding the efficacy of the nonstenting technique remain to be established. In recent years, improvements in surgical techniques and perioperative care of patients undergoing duct-to-mucosa anastomosis of pancreaticojejunostomy without stenting have resulted in declines in mortality and morbidity rates.
In addition, in our study, there were no differences in postoperative complications between the two groups. Similar to the results of other reports, there were no differences between the two groups with respect to grave progress of pancreatic fistulas. The low rate of pancreatic fistula development after PD observed in our study was due to the use of nonstenting duct-to-mucosa anastomosis of pancreaticojejunostomy in all generations, and the incidence of pancreatic fistula development in the elderly patients was similar to that observed in the younger patients. Regarding delayed gastric emptying that prolonged hospital stays, our study showed no differences between the two groups. However, the incidence of delayed gastric emptying in elderly patients has been reported to be higher than that in younger patients [25, 26]. In this study, anastomosis between the jejunum and the stomach or duodenum with antecolic reconstruction was made as straight as possible so as to improve the physical flow until peristalsis improved. Therefore, the incidence of delayed gastric emptying in our study was decreased in all generations compared with that observed in previous reports [25, 26].
Aging is a significant risk factor for preoperative patients in poor nutritional condition. However, according to our procedures, aging is not the only risk factor to indicate for PD in patients with periampullary disease.
Conclusion
PD without the use of stenting tubes in duct-to-mucosa pancreaticojejunostomy can be safely performed in elderly as well as in younger patients.
References
Tani M, Kawai M, Hirono S, Ina S, Miyazawa M, Nishioka R, et al. A pancreaticoduodenectomy is acceptable for periampullary tumors in the elderly, even in patients over 80 years of age. J Hepatobiliary Pancreat Surg. 2009;16:675–80 (Epub 2009 Apr 22).
Malleo G, Marchegiani G, Salvia R, Butturini G, Pederzoli P, Bassi C. Pancreaticoduodenectomy for pancreatic cancer: the Verona experience. Surg Today. 2011 41:463–70 (Epub 2011 Mar 23).
Kuroki T, Tajima Y, Kitasato A, Adachi T, Kanematsu T. Stenting versus non-stenting in pancreaticojejunostomy: a prospective study limited to a normal pancreas without fibrosis sorted by using dynamic MRI. Pancreas. 2011;40:25–9.
Pessaux P, Sauvanet A, Mariette C, Paye F, Muscari F, Cunha AS, et al. External pancreatic duct stent decreases pancreatic fistula rate after pancreaticoduodenectomy: prospective multicenter randomized trial. Ann Surg. 2011;253:879–85.
Poon RT, Fan ST, Lo CM, Ng KK, Yuen WK, Yeung C, et al. External drainage of pancreatic duct with a stent to reduce leakage rate of pancreaticojejunostomy after pancreaticoduodenectomy: a prospective randomized trial. Ann Surg. 2007; 246:425–33 (discussion 433–5).
Winter JM, Cameron JL, Campbell KA, Chang DC, Riall TS, Schulick RD, et al. Does pancreatic duct stenting decrease the rate of pancreatic fistula following pancreaticoduodenectomy? Results of a prospective randomized trial. J Gastrointest Surg. 2006;10:1280–90 (discussion 1290).
Imaizumi T, Hatori T, Tobita K, Fukuda A, Takasaki K, Makuuchi H. Pancreaticojejunostomy using duct-to-mucosa anastomosis without a stenting tube. J Hepatobiliary Pancreat Surg. 2006;13:194–201.
Suzuki S, Kaji S, Koike N, Harada N, Tanaka S, Hayashi T, et al. Pancreaticojejunostomy of duct to mucosa anastomosis can be performed more safely without than with a stenting tube. Am J Surg. 2009;198:51–4 (Epub 2009 Feb 13).
Smyrniotis V, Arkadopoulos N, Kyriazi MA, Derpapas M, Theodosopoulos T, Gennatas C, et al. Does internal stenting of the pancreaticojejunostomy improve outcomes after pancreatoduodenectomy? A prospective study. Langenbecks Arch Surg. 2010;395:195–200.
Suzuki S, Kaji S, Koike N, Harada N, Hayashi T, Suzuki M, et al. Pancreaticoduodenectomies with a duct-to-mucosa pancreaticojejunostomy anastomosis with and without a stenting tube showed no differences in long-term follow-up. J Hepatobiliary Pancreat Sci. 2011;18:258–62.
Ishikawa A, Beppu M. Population statistics of Japan 2008. Tokyo: Yamato-Sogo; 2006.
Ouaïssi M, Sielezneff I, Pirrò N, Merad A, Loundou A, Chaix JB, et al. Pancreatic cancer and pancreaticoduodenectomy in elderly patient: morbidity and mortality are increased. Is it the real life? Hepatogastroenterology. 2008;88:2242–6.
Makary MA, Winter JM, Cameron JL, Campbell KA, Chang D, Cunningham SC, et al. Pancreaticoduodenectomy in the very elderly. J Gastrointest Surg. 2006;10:347–56.
Brozzetti S, Mazzoni G, Miccini M, Puma F, De Angelis M, Cassini D, et al. Surgical treatment of pancreatic head carcinoma in elderly patients. Arch Surg. 2006;141:137–42.
Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, International Study Group on Pancreatic Fistula Definition, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138:8–13.
Balcom JH, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with pancreatic resections. Changing indications, older patients, and decreasing length of hospitalization. Arch Surg. 2001;136:391–8.
Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery. 2007;142:761–8.
Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007;142:20–5.
Kojima Y, Yasukawa H, Katayama K, Note M, Shimada H, Nakagawara G. Postoperative complications and survival after pancreatoduodenectomy in patients aged over 70 years. Surg Today. 1992;22:401–4.
Cameron JL, Pitt HA, Yeo CJ, Lillemoe KD, Kaufman HS, Coleman J. One hundred and forty-five consecutive pancreaticoduodenectomies without mortality. Ann Surg. 1993;217:430-5 (discussion 435–8).
Hodul P, Tansey J, Golts E, Oh D, Pickleman J, Aranha GV. Age is not a contraindication to pancreaticoduodenectomy. Am Surg. 2001;67:270-5 (discussion 275–6).
Riall TS, Reddy DM, Nealon WH, Goodwin JS. The effect of age on short-term outcomes after pancreatic resection: a population-based study. Ann Surg. 2008;248:459–67.
Finlayson E, Fan Z, Birkmeyer JD. Outcomes in octogenarians undergoing high-risk cancer operation: a national study. J Am Coll Surg. 2007;205:729–34 (Epub 2007 Oct 1).
Lee MK, Dinorcia J, Reavey PL, Holden MM, Tsai WY, Stevens PD, et al. Pancreaticoduodenectomy can be performed safely in patients aged 80 years and older. J Gastrointest Surg. 2010;14:1838–46 (Epub 2010 Sep 8).
Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg. 2004;240:293–8.
Sohn TA, Yeo CJ, Cameron JL, Lillemoe KD, Talamini MA, Hruban RH, et al. Should pancreaticoduodenectomy be performed in octogenarians? J Gastrointest Surg. 1998;2:207–16.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Suzuki, S., Kaji, S., Koike, N. et al. Pancreaticoduodenectomy can be safely performed in the elderly. Surg Today 43, 620–624 (2013). https://doi.org/10.1007/s00595-012-0383-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-012-0383-6