
Abstract
In anterior cruciate ligament (ACL) reconstruction, transtibial drilling of the femoral tunnel has been criticized for its vertical and less anatomical tunnel, which accompanied rotational instability of knee. Many authors recommend anteromedial (AM) portal drilling technique, which creates more oblique and anatomic femoral tunnel. However, recent researches show that oblique tunnel is related to risks of too short femoral tunnel, blowout of back wall, and posterolateral structures injury. Is oblique femoral tunnel really essential for anatomic reconstruction? We introduce a modified AM technique, which abandons the oblique tunnel and provides vertical femoral tunnel and oblique graft with anatomic starting point. The fundamental of the new technique is that oblique graft but not oblique tunnel is essential for rotational stability of knee. Thus, it avoids the risks and preserves anatomic reproduction of ACL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Optimal femoral tunnel placement has been intensively concerned in anterior cruciate ligament (ACL) reconstruction, yet tunnel misplacement may compromise the restoration of knee stability.
For the preparation of the femoral tunnel, transtibial (TT) technique [1–4] and anteromedial (AM) portal technique [2, 3, 5] are most widely used methods. Compared with TT technique, obviously the advantages of AM technique include unconstrained starting point and excellent rotational stability as a result of the creation of more oblique (or horizontal) and anatomic femoral tunnel [2, 3, 5]. Nevertheless, risks of AM technique, such as short or bicortical sockets, blowout along back wall of lateral femoral condyle, and danger to peroneal neurovascular structures, have been noticed soon [6–9]. Unfortunately, it seems that AM technique generates more problems in order to resolve one. We provide a viewpoint which may provide a solution combined the advantages of both TT and AM techniques. The origin of our view is the answers for two questions. Is oblique tunnel or oblique graft essential to reproduce the course of the native ACL and to avoid abnormal rotational laxity? Oblique graft is essence. Is anatomic ACL reconstruction by AM technique doomed to create an oblique femoral tunnel? No. The two answers imply that anatomic ACL reconstruction may be realized by another solution: vertical femoral tunnel and oblique graft (Fig. 1).

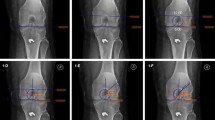
Postoperative anteroposterior view X-ray graph of a right knee. Traditional femoral tunnel preparation may follow the direction of 11 o’clock (line A) or 10 o’clock (line B) of the clock-face description. It is obvious that tunnel of line A is vertical and long, whereas line B is oblique and short. Line C provides another possible solution which has the same femoral starting position (FSP) on the notch wall as line B and the tunnel toward the direction of line A; therefore, it realizes vertical femoral tunnel and oblique graft. Arrow EndoButton, line D the joint line
Could this solution really happen in surgery or was it just a theoretical possibility? Bedi [7] and we [10] have previously discussed the probability that a femoral starting point (FSP) at a low clock-face position might also create a vertical tunnel. To show the practicability of the new solution, we reported a modified AM technique, in which both vertical femoral tunnel and oblique graft were easily obtained in clinical cases, and we named this method as femoral tunnel obliquity adjustment (FTOA) technique. The FTOA technique not only preserves anatomic reconstruction as the superiority of AM technique, but also prepares vertical tunnel to avoid the pitfalls which have been listed in recent studies [6–9].
Technical note
Surgical technique
All procedures but the preparations of femoral tunnel were same as the traditional AM drilling technique. The patients were positioned supine on the operating table with an inflated tourniquet applied to the operative extremity. With a tendon striper, both the semitendinosus and gracilis tendons were harvested. After all of four limbs of graft were separately baseball-running stitched with non-absorbable sturdy suture (Ethibond), the graft was sized and then tensioned and conditioned. Using the standard anterolateral and anteromedial portals, routine diagnostic arthroscopy and debridement of ruptured ACL were performed. Moreover, a notchplasty was required for the cases of narrow notch.
Femoral tunnel preparation using the FTOA technique:
At 90° of flexion, the anatomic FSP was marked by radiofrequency device (Video 1) on the center of the lateral bifurcate ridge, which located between the native AM and PL bundle insertion sites [11], and it might also follow the clock-face reference (at the 10 o’clock position for the right knee or the 2 o’clock the left knee). Since some researchers [11] and we [10] reported that clock-face reference might provide a disservice to anatomic reconstruction methods, in this step, both bony landmarks and clock-face reference were considered. Then, at 100° of knee flexion, with the assistance of the femoral aimer, a guide pin and a thin cannulated reamer (5.0 mm in diameter), a shallow pit (3 mm depth) was made at the center of the mark (Fig. 2a, Video 2), and then, the reamer and guide pin were removed out of the joint. In this step, the orientation of guide pin was not important, but 3-mm-depth pit at insertion of native ACL must be created as FSP of graft.

a A shallow pit (arrowhead) is created on the lateral wall (LW) of the intercondylar notch according to the mark made by radiofrequency device. b The guide pin (P) is placed on the bottom of the shallow pit (the red circle) by freehand toward a more vertical orientation than traditional AM technique. The pin (P) can be adjusted to follow any orientation in purple shaded area between blue arrow and green arrow according to the surgeon’s will. R tibial remnant of ACL, PCL posterior cruciate ligament (color figure online)
Finally, the femoral tunnel was drilled through the AM portal with the knee placed in flexion between 100° and 120°. Through AM portal, the guide pin was placed on the bottom of the shallow pit and drilled in relatively vertical direction by freehand (usually equal to the direction of 11 o’clock for the right knee or the 1 o’clock the left knee, Figs. 2b, 3a–c). It seemed that the pin toward 11 o’clock was contradiction with FSP at the 10 o’clock position, actually it was not. In previous publication [10], we have discussed this issue that coronal obliquity of tunnel and clock-face description of FSP should be separated into two individual conceptions, which can not be translated to each other in most situations. Then, the guide pin was over-drilled with a reamer of the size of the graft diameter (usually between 7 and 10 mm) to a depth of 25 mm. The far cortex was breached by a 4.5 mm reamer and the tunnel length was assessed with the depth gauge and recorded (Video 3). Femoral graft fixation was performed by EndoButton continuous loop (Smith and Nephew Endoscopy), which was usually between 15 and 25 mm, whereas the tendinous portion on tibial side was fixed at 30° of knee flexion by bioabsorbable interference screw. The knee was arthroscopically observed again to exclude graft impingement (Video 4).

a The 3D-CT of distal femur in prone view. The magnification of the yellow box is shown as b and c. b While the guide pin is drilled freehand without assistance of the shallow pit toward the direction of red line, the pin may slip toward the direction of yellow arrow. c After the guide pin is rest on the bottom of the shallow pit (the green half circle) and stably drilled, it is over-drilled with a reamer and therefore the pit vanishes in the coming femoral tunnel (the yellow lines). L lateral side of femur, M medial side of femur, P posterior side of femur (color figure online)
Radiographic assessment
The postoperative anteroposterior view X-ray graph was evaluated for the coronal angle of the femoral tunnel, which was defined by the angle subtended between the tunnel and the joint line (Fig. 1). In 4 cases, the postoperative 3D-CT was performed to assess the position of femoral tunnel aperture.
Results
To date, ten patients underwent ACL reconstruction by the FTOA technique. The duration of creation of the shallow pit was about 2 min. The FTOA technique did not take obviously longer time than traditional AM method. The mean femoral tunnel length was 41.7 mm (range 38–48 mm), while posterior wall blowout of lateral femoral condyle and posterolateral structure injury has not been observed.
Postoperative X-ray graph of a right knee (Fig. 1) showed that the femoral tunnel created by the FTOA technique (line C) was much more vertical than that by the traditional AM technique (line B), while FSP of both tunnels is at 10 o’clock on the notch wall. The coronal angle of the femoral tunnel by the FTOA technique, which was defined by the angle subtended between the tunnel and the joint line (line D), was 66.2° (equal to 11:12 of the clock-face description), whereas the coronal angle by the traditional AM technique was 33.8° (equal to 10:08 of the clock-face description). The mean coronal angle of all ten FTOA cases was 55.1° (range 39.0°–67.6°), which was equal to 10:50 of the clock-face description.
Based on the previously reported data of anatomic sites of AM and PL bundles of ACL [12], the postoperative 3D-CT of our study showed that the center of FSP was very close to the midpoint between the native insertion sites of AM and PL bundles (Fig. 4a). The 3D-CT also showed that the exit of tunnel on the lateral aspect of femur located at 54.2 % of anterior-to-posterior anatomical axes, which was near the midpoint (Fig. 4b).

a According the quadrant method, the postoperative 3D-CT shows that the center of femoral tunnel aperture (the red point) is close to the midpoint between the native AM (the blue point) and PL (the green point) bundles of ACL. Three yellow circles around the red point are tunnel aperture centers of other 3 cases. b The center of the exit of tunnel (the red point on EndoButton) on the lateral facet of femur is near the midpoint of anterior-to-posterior axes (the blue line) (color figure online)
Discussion
Researchers recognized that TT technique usually results in vertical graft orientation which can be rotational instability in despite of its excellent anteroposterior stability [1–4, 13, 14]. The AM technique outperforms TT technique because of its easy creation of more oblique femoral tunnel for anatomic reproduction of ACL [3]. However, pitfalls of unsafe surgical procedures compromised AM technique to be ideal method [5–9].
In our study, the FTOA technique abandons the popular oblique tunnel but provides a vertical femoral tunnel with an anatomic starting point. The postoperative 3D-CT showed that the center of FSP was very close to the midpoint between the native insertion sites of AM and PL bundles (Fig. 4a). Under arthroscopic view (Video 3), it was found that the aperture of completed femoral tunnel was quite low (distal) on the lateral wall of the intercondylar notch, and the guide rope connected femoral tunnel and tibial tunnel indicated the orientation of the coming ACL graft was quite oblique. The 3D-CT (Fig. 4a), arthroscopic view, and postoperative X-ray (Fig. 1) proved that even with a vertical femoral tunnel, the ACL graft could be oblique and with an anatomic FSP. Moreover, the exit of femoral tunnel on the lateral facet of femur approximately located on the midpoint of anterior-to-posterior axes (Fig. 4b), and the mean femoral tunnel length was 41.7 mm (range 38–48 mm). It implies that the FTOA technique can avoid risks as a result of oblique tunnel drilling through AM portal. The fundamental of the FTOA technique is that oblique graft but not oblique tunnel is essential for restoration of normal rotational laxity. Our study proves that oblique tunnel is unnecessary for anatomic ACL reconstruction. Have we ever been fooled by the misunderstanding of oblique tunnel in anatomic ACL reconstruction? It may be.
Golish SR [6] showed that the differences in tunnel length between starting positions were statistically significant, and femoral tunnel at 10:17 o’clock was around 37 mm. Using the FTOA technique, the guide pin can follow any orientation in a sector area (Fig. 2b), which means that from the same FSP, the femoral tunnel obliquity or tunnel length can be adjusted. In our study, the mean femoral tunnel length was 41.7 mm, which implied that 10 o’clock starting position was not doomed to short tunnel length.
Certainly, in theory, surgeons can drill femoral guide pin freehand without assistance of shallow pit (Fig. 3b), but any experienced arthroscopist knows it is tough mission on the smooth wall of notch. The angle between the lateral wall and the guide pin is too acute to stable the guide pin. It inevitably leads guide pin slip around, so that the FSP may shift away from anatomic insertion (Fig. 3b). The shallow pit provides a rough operating area for accurate drilling according to the surgeon’s will (Fig. 3c). Some doctors may doubt that the FTOA technique leads to enlargement of the aperture of femoral tunnel. Actually, the shallow pit created by thin reamer has been over-drilled with thick reamer; therefore, the pit totally vanished in the coming femoral tunnel (Fig. 3c). Recently, we have already performed double-bundle ACL reconstruction using the FTOA technique, and it would be reported in future.
There are some limitations in this technical note. Firstly, we only investigated the possibility of the FTOA technique as surgical procedures and did not arrange control group and observed the clinical outcomes. Secondly, though our study provided postoperative X-ray and 3D-CT to indicate the validation of the FTOA technique, the small number of cases might compromise the concrete conclusion. No doubt, a randomize controlled trial compared the FTOA technique and traditional AM portal drilling with large number of cases and long period follow-up should be performed in the future.
Conclusion
The FTOA technique abandons the oblique femoral tunnel by traditional AM portal drilling technique and provides an anatomic and safe mode with vertical tunnel and oblique graft, which avoids the risks of AM technique, such as short tunnel, blowout along back wall of lateral femoral condyle, and danger to peroneal neurovascular structures.
References
Giron F, Cuomo P, Edwards A, Bull AM, Amis AA, Aglietti P (2007) Double-bundle “anatomic” anterior cruciate ligament reconstruction: a cadaveric study of tunnel positioning with a transtibial technique. Arthroscopy 23(1):7–13 PMID: 17210421
Harner CD, Honkamp NJ, Ranawat AS (2008) Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy 24(1):113–115 PMID: 18188873
Steiner ME, Battaglia TC, Heming JF, Rand JD, Festa A, Baria M (2009) Independent drilling outperforms conventional transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med 37(10):1912–1919 PMID: 19729364
Jepsen CF, Lundberg-Jensen AK, Faunoe P (2007) Does the position of the femoral tunnel affect the laxity or clinical outcome of the anterior cruciate ligament–reconstructed knee? A clinical, prospective, randomized, double-blind study. Arthroscopy 23(12):1326–1333 PMID: 18063177
Lubowitz JH (2009) Anteromedial portal technique for the anterior cruciate ligament femoral socket: pitfalls and solutions. Arthroscopy 25(1):95–101 PMID: 19111224
Golish SR, Baumfeld JA, Schoderbek RJ, Miller MD (2007) The effect of femoral tunnel starting position on tunnel length in anterior cruciate ligament reconstruction: a cadaveric study. Arthroscopy 23(11):1187–1192 PMID: 17986406
Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ III (2010) Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthroscopy 26(3):342–350 PMID: 20206044
Chang CB, Yoo JH, Chung BJ, Seong SC, Kim TK (2010) Oblique femoral tunnel placement can increase risks of short femoral tunnel and cross-pin protrusion in anterior cruciate ligament reconstruction. Am J Sports Med 38(6):1237–1245 PMID: 20348283
Gelber PE, Reina F, Torres R, Pelfort X, Tey M, Monllau JC (2010) Anatomic single-bundle anterior cruciate ligament reconstruction from the anteromedial portal: evaluation of transverse femoral fixation in a cadaveric model. Arthroscopy 26(5):651–657 PMID: 20434663
Xu H, Zhang C (2010) Can coronal oblique angel be translated to clock-face position in femoral tunnel preparation of anterior cruciate ligament reconstruction? Arthroscopy 26(12):1566–1568 PMID: 21112474
van Eck CF, Lesniak BP, Schreiber VM, Fu FH (2010) Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy 26(2):258–268 PMID: 20141990
Forsythe B, Kopf S, Wong AK, Martins CAQ, Anderst W, Tashman S, Fu FH (2010) The location of femoral and tibial tunnels of anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am 92(6):1418–1426 PMID: 20516317
Lee MC, Seong SC, Lee S, Chang CB, Park YK, Jo H, Kim CH (2007) Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction. Arthroscopy 23(7):771–778 PMID: 17637414
Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL (2003) Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o’clock and 10 o’clock femoral tunnel placement. 2002 Richard O’Connor Award paper. Arthroscopy 19(3):297–304
Conflict of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The patients in this case report were informed that data of their case would be submitted for publication and they agreed to this.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 2 (MPG 4672 kb)
Supplementary material 3 (MPG 4048 kb)
Supplementary material 4 (MPG 8246 kb)
Supplementary material 5 (MPG 1622 kb)
Rights and permissions
About this article
Cite this article
Zhang, C., Xu, H., Li, X. et al. Oblique femoral tunnel or oblique graft? A modified anteromedial portal technique to obtain vertical femoral tunnel and oblique graft in anatomic anterior cruciate ligament reconstruction. Eur J Orthop Surg Traumatol 23, 731–735 (2013). https://doi.org/10.1007/s00590-012-1046-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-012-1046-4