
Abstract
Background
With the advancement of minimally invasive spinal surgery, endoscopic lumbar decompression has been widely used for the treatment of degenerative lumbar spinal diseases. Iatrogenic dural tear is a relatively common complication in endoscopic lumbar spinal surgery. The golden standard of treatment for iatrogenic dural tear is immediate open conversion and direct repair under microscopic visualization. Recently, most of endoscopic spinal surgery is performed under local anesthesia. So, conversion to open surgery is very embarrassing situation because of the need of additional general anesthesia. But, direct endoscopic dural repair is very difficult procedure due to the limitation of manipulation. No report showed direct dural suture under full endoscopic situation.
Purpose
The purpose of this surgical technique is to provide a method of full endoscopic dural suture repair without conversion to open surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Iatrogenic dural tear is a relatively common complication in lumbar spinal surgery. The incidence of iatrogenic dural tears during lumbar decompression surgery varies and ranges from 1 to 17% [1,2,3,4]. Direct consequences from a dural tear include headache, meningeal pseudocyst formation, dural cutaneous fistulas leading to arachnoiditis, delayed wound healing and wound infection. Indirect consequences associated with prolonged bed rest that is often required include pneumonia, pressure ulcers, deep vein thrombosis, pulmonary embolism and aspiration. The treatment of iatrogenic dural tear remains challenging, especially in endoscopic spinal surgery. Recently, most of endoscopic spinal surgery is performed under local anesthesia. The golden standard of treatment for iatrogenic dural tear during endoscopic surgery is immediate open conversion and direct repair under microscopic visualization. However, conversion from endoscopic to open surgery is very embarrassing situation because of the need of additional general anesthesia. Direct endoscopic dural suture repair is very difficult procedure due to the limitation of manipulation. So, there are various sealants for the treatment of dural tear such as fibrin glue, hydrogel, cyanoacrylate, bioabsorbable staples and various types of grafts and patches [5]. But, in most of the cases intraoperative attempt to shielding the defect under endoscopic visualization is ineffective. Moreover, various sealants were associated with complications such as neurotoxicity, allergic reaction, anaphylaxis and transmission of viruses [6]. No reports showed direct dural suture under full endoscopic situation. So, we introduce the novel direct dural suture repair technique under full endoscopic situation without conversion to open surgery.
Surgical technique (Youn’s technique)
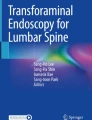
Initially, dural tear or defect site must be cleaned for the direct dural repair procedure. We attempted to do watertight closure of the dural tear, whenever possible, by using simple interrupted suture with 6–0 prolene thread (round-bodied double-arm needle, Ethicon, Johnson and Johnson, SL, USA). It is difficult to do the primary suture repair procedure on a dural defect or tear site using only the endoscopic instruments. In particular, the behavior of sewing up both sides of dural membranes at once by manipulation of a suture needle is not easy due to the gap in the dural tear site. Furthermore, if the procedure of sewing up the dural membrane is not properly performed, it can cause punctures by suture needle on the dural membrane, which may lead to problems such as CSF leakage. Attempts to stick through the two dural membranes at one time, especially in uneasy manipulatory situations, are at risk of entrapment of the rootlet. For that reason, the authors used a double-arm needle to pass one needle through one dural membrane (Fig. 1) and then pulled out the two needles through the working channel of the endoscope (Fig. 2). After single knotting of the suture thread at the outside the endoscope, one needle was passed through the hole of the endoscopic currette (Fig. 3) like putting a thread through a needle. Although the authors used an endoscopic currette for pushing a knot, any device that has a hole and can pass through the working channel can be used (Fig. 4). When the endoscopic currette is pushed gently into the working channel (Fig. 5), the knotted thread can be observed in the endoscope. And the currette can be used to tighten the knot by applying a little tension, like a knot pusher used in a shoulder arthroscopic surgery (Fig. 6). At this time, the suture thread is thin and the tissue of the dural membrane is very weak, so too much tension should not be applied to the suture thread. Because the suture thread is very thin, the knot can be pushed into the surgical field with endoscopic vision only by gentle pushing of the instrument. After repeating the same knotting procedures 2–3 times, we can cut the thread using an endoscopic cutter (Fig. 7). Once the first knot is completed, the gap of the dural defect becomes narrower, making it easier to do the rest of the suture. Therefore, we recommend to use a suture thread with double-arm needle for the first suture in the repair process. By using a double-arm needle, we can save operation time and make suture much easier. After the interval of the dural tear site has narrowed, the second needling can be performed by passing bilateral membranes at the same time (Fig. 8a, b). After direct dural repair in a full endoscopic guide, endoscopic posterior lumbar decompression was performed as planned (Fig. 9).

A double-arm needle

The two needles were pulled out through the working channel of the endoscope

After single knotting of the suture thread at the outside the endoscope, one needle was passed through the hole of the endoscopic currette

An endoscopic currette which was used for pushing a knot

When the endoscopic currette is pushed gently into the working channel, the knotted thread can be observed in the endoscope

The currette can be used to tighten the knot by applying a little tension, like a knot pusher

After repeating the same knotting procedures 2–3 times, we can cut the thread using an endoscopic cutter

a, b After the interval of the dural tear site has narrowed, the second needling can be performed by passing bilateral membranes at the same time

After direct dural repair in a full endoscopic guide, endoscopic posterior lumbar decompression was performed as planned
Discussion
Endoscopic spinal surgery is considered to be a good way to meet the demands of the current time requiring minimally invasive surgery for the body and has made great progress in recent years. As many spinal endoscopic surgeries are performed, surgical complications are naturally increased. One of the most important complications during the endoscopic spinal surgery is an incidental dural tear. And its treatment remains challenging, especially in endoscopic procedures.
During the open lumbar spinal surgeries, primary dural suture repair is accepted as the gold standard for the management of a dural tear [7]. Some authors believe that it is inevitable to repair the dural tear to prevent the occurrence of a pseudomeningocele or even spinal fluid leak [8, 9]. Other techniques also have been employed to deal with the occurrence of a dural tear including the use of fat, muscle or facial grafts, use of fibrin glue [10,11,12,13].
In endoscopic lumbar spinal surgery, direct repair via suturing was impossible due to inaccessible location of dural tear and limited working space. Operating through a small working channel may not allow the manipulation of instruments as accustomed in conventional surgery which could then force the surgeon to convert the procedure to open surgery. There have been several studies on the repair of dural tear using tubular assisted endoscopic procedures, but the study of full endoscopic dural suture repair technique through small working cannula under full endoscopic situation has not been reported yet [14,15,16,17,18].
If a dural tear occurs during spinal endoscopic surgery, the treatment method can be determined according to the size of the tear. If the size of the tear is small, a sealant such as a surgicel collagen matrix or a fibrin glue can be used to seal the hole [19]. However, if the size of the tear is large, primary suture repair is needed. In such cases, the procedure has been carried out by conversion to open spinal surgery [20]. This course of treatment has created an uncomfortable situation for both the patient and the surgeon. Furthermore, because of the high incidence of lumbar spinal endoscopic surgery under local anesthesia in recent years, the sudden conversion to general anesthesia may undermine the rapport between the patient and the surgeon. Therefore, we aimed to introduce primary dural suture repair technique through full endoscopic procedure for dural tear occurred during the endoscopic lumbar spinal surgery under local anesthesia.
In open lumbar spinal surgeries, many surgeons perform primary closure of dural tear with or without the additional fibrin glue [21,22,23]. Those authors recommend direct suturing of the dural tear, and if a subsequent primary closure is not possible, a muscle patch with or without additional closure aids (e.g., fibrin glue, Spongostan, TachoSil, or Gelform) should be considered [21].
Dural repair without direct suturing is also a well-known technique in conventional spine surgery, and about 80% of spine surgeons reported good experience with this technique [24]. There have been also some reports of dural tear treatment without primary dural suture in endoscopic lumbar spinal surgery [7, 14]. However, such treatments seem to be of value as an alternative to treating dural tear without open conversion surgery. Ahn et al. [20] reported that the intraoperative attempt to repair the defect by shielding materials under the endoscopic visualization was ineffective and the proper management option was immediate open conversion and direct repair under microscopic visualization. We authors also believe that direct repair via suturing is the definite treatment method of dural tear if possible. Furthermore, endoscopic dural suture was possible using only suture thread and basic endoscopic instruments prepared in the operating room without specially designed instruments for the suture procedure through our technique.
Similar to open spinal surgery, dural tears affecting the nerve root sleeve or axilla, or lying anteriorly, present a significant challenge to primary suture repair through the endoscopic technique and, therefore, are often managed without suture repair. Suturing root sleeve may theoretically result in stenosis of the affected root, while another potential risk of suture repair is ‘lassoing’ of the underlying cauda equine roots [7]. However, endoscopic dural suture surgery can provide more detailed view of the border between dura and nerve roots compared to open spinal surgery, reducing the fatal accidents of tying the dura and nerve root in a bundle.
Reported failure rates for watertight suture repair range from 5 to 9% [10, 25]. The pin holes created by passage of the suture needle may convert a low pressure dural defect to a high pressure defect resulting in persistent leakage and possible accounting for the 5–9% rate of persistent leakage [26,27,28]. Although we authors believe that watertight suture repair through this full endoscopic technique can produce satisfactory results for dural tears, in cases where CSF leakage due to needles is concerned, an additional sealant such as fibrin glue may be better for the pin holes created by the passage of the suture needle. In addition, even if the size of the defect is too large to achieve watertight repair through a direct suture, dural suturing to reduce the size of the tear and then using ancillary products may increase the healing potential rather than treating the defect with only the sealant.
Conclusion
Endoscopic dural suture repair for dural tear lesion during endoscopic lumbar spinal surgery can be prohibitively difficult. Using Youn’s technique, primary endoscopic dural suture repair can be accomplished after dural tear only with basic endoscopic instruments including an endoscopic ring currette and a 6–0 prolene suture.
References
Epstein NE (2007) The frequency and etiology of intraoperative dural tears in 110 predominantly geriatric patients undergoing multilevel laminectomy with noninstrumented fusions. J Spinal Disord Tech 20(5):380–386
Bosacco SJ, Gardner HJ, Guille JT (2001) Evaluation and treatment of dural tears in lumbar spine surgery: a review. Clin Orthop Relat Res 389:238–247
Jones AA, Stambough JL, Balderston RA, Rothman RH, Booth RE Jr (1989) Long-term results of lumbar spine surgery complicated by unintended incidental durotomy. Spine 14:443–446
Khan MH, Rihn J, Steele G, Davis R, Donaldson WF 3rd, Kang JD, Lee JY (2006) Postoperative management protocol for incidental dural tears during degenerative lumbar spine surgery: a review of 3,183 consecutive degenerative lumbar cases. Spine 31:2609–2613
Dafford EE, Anderson PA (2015) Comparison of dural repair techniques. Spine J 15:1099–1105
Epstein NE (2010) Dural repair with four spinal sealants: focused review of the manufacturers’ inserts and the current literature. Spine J 10:1065–1068
Grannum S, Patel MS, Attar F, Newey M (2014) Dural tears in primary decompressive lumbar surgery. Is primary repair necessary for a good outcome? Eur Spine J 23(4):904–908
Guerin P, El Fegoun AB, Obeid I, Gille O et al (2012) Incidental durotomy during spine surgery: incidence, management and complications. A retrospective review. Injury 43(4):397–401
Epstein NE (2013) A review article on the diagnosis and treatment of cerebrospinal fluid fistulas and dural tears occurring during spinal surgery. Surg Neurol Int 4(Suppl 5):S301–S317
Wang JC, Bohlman HH, Riew KD (1998) Dural tears secondary to operations on the lumbar spine: management and results after a two-year-minimum follow-up of eighty-eight patients. J Bone Joint Surg Am 80(12):1728–1732
Miller PR, Elder FW Jr (1968) Meningeal pseudocysts (meningocele spurius) following laminectomy. Report of ten cases. J Bone Joint Surg Am 50(2):268–276
Karaeminogullari O, Atalay B, Sahin O, Ozalay M et al (2005) Remote cerebellar hemorrhage after a spinal surgery complicated by dural tear: case report and literature review. Neurosurgery 57(1 Suppl):E215
Shaffrey CI, Spotnitz WD, Shaffrey ME, Jane JA (1990) Neurosurgical applications of fibrin glue: augmentation of dural closure in 134 patients. Neurosurgery 26(2):207–210
Oertel JM, Burkhardt BW (2017) Full endoscopic treatment of dural tears in lumbar spine surgery. Eur Spine J 26(10):2496–2503
Sun MJ, Gao SM, Wang YH (2011) Simultaneous intra-operative repair for inadvertent dural tear under posterior lumbar disk scope. Orthop Surg 3(3):188–192
Shibayama M, Mizutani J, Takahashi I, Nagao S et al (2008) Patch technique for repair of a dural tear in microendoscopic spinal surgery. J Bone Joint Surg Br 90(8):1066–1067
Chou D, Wang VY, Khan AS (2009) Primary dural repair during minimally invasive microdiscectomy using standard operating room instruments. Neurosurgery 64(5 Suppl 2):356–358
Than KD, Wang AC, Etame AB, La Marca F et al (2008) Postoperative management of incidental durotomy in minimally invasive lumbar spinal surgery. Minim Invas Neurosurg 51(5):263–266
Galarza M, Gazzeri R, Alfaro R, de la Rosa P et al (2018) Evaluation and management of small dural tears in primary lumbar spinal decompression and discectomy surgery. J Clin Neurosci 50:177–182
Ahn Y, Lee HY, Lee SH, Lee JH (2011) Dural tears in percutaneous endoscopic lumbar discectomy. Eur Spine J 20(1):58–64
Guerin P, El Fegoun AB, Obeid I, Gille O et al (2012) Incidental durotomy during spine surgery: incidence, management and complications. A retrospective review. Injury 43(4):397–401
Papavero L, Engler N, Kothe R (2015) Incidental durotomy in spine surgery: first aid in ten steps. Eur Spine J 24(9):2077–2084
Tafazal SI, Sell PJ (2005) Incidental durotomy in lumbar spine surgery: incidence and management. Eur Spine J 14(3):287–290
Gautschi OP, Stienen MN, Smoll NR, Corniola MV et al (2014) Incidental durotomy in lumbar spine surgery–a three-nation survey to evaluate its management. Acta Neurochir (Wien) 156(9):1813–1820
Hodges SD, Humphreys SC, Eck JC, Covington LA (1999) Management of incidental durotomy without mandatory bed rest. A retrospective review of 20 cases. Spine 24(19):2062–2064
Narotam PK, Jose S, Nathoo N, Taylon C, Vora Y (2004) Collagen matrix (DuraGen) in dural repair: analysis of a new modified technique. Spine 29(24):2861–2867
Cammisa FP Jr, Girardi FP, Sangani PK et al (2000) Incidental durotomy in spine surgery. Spine 25:2663–2667
Jankowitz BT, Atteberry DS, Gerszten PC, Karausky P et al (2009) Effect of fibrin glue on the prevention of persistent cerebral spinal fluid leakage after incidental durotomy during lumbar spinal surgery. Eur Spine J 18(8):1169–1174
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has any potential conflict of interest.
Rights and permissions
About this article

Cite this article
Shin, J.K., Youn, M.S., Seong, Y.J. et al. Iatrogenic dural tear in endoscopic lumbar spinal surgery: full endoscopic dural suture repair (Youn’s technique). Eur Spine J 27 (Suppl 3), 544–548 (2018). https://doi.org/10.1007/s00586-018-5637-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-018-5637-6