
Abstract
Insufficient blood supply to the intervertebral disc (IVD) has been proposed to play a role as causative factor in IVD degeneration. There is an association between IVD diseases and increased risk of dying of ischaemic heart disease. Obesity and tobacco are potential risk factors for degenerative IVD disease. High blood cholesterol and triglycerides serum levels are risk factors for atherosclerosis, and could be responsible for a decreased in the blood supply to the already poor vascularized IVD. We performed a frequency-matched case–control study to determine the serum levels of patients with symptomatic herniated lumbar disc. We examined the fasting serum lipid levels in 384 subjects who were operated at our institution. Group 1 included 169 consecutive patients (115 men and 54 women; mean age: 59.1 years, range 29–85) who underwent surgery for symptomatic disc herniation. Group 2 (control group) included 169 patients (115 men and 54 women; mean age: 61 years, range 26–86) who underwent arthroscopic meniscectomy for a meniscal tear in the same period. These patients were frequency-matched by age (within 3 years) and gender with patients of Group 1. Sera were extracted from blood samples and the concentrations of total cholesterol (TC) and triglycerides (TG) were determined. When comparing the two groups, patients with symptomatic herniated lumbar disc showed statistically significant higher triglyceride concentration (P = 0.02) and total cholesterol concentration (P = 0.01). Serum lipid levels may be a risk factor for IVD pathology. An enhanced understanding of these factors holds the promise of new approaches to the prevention and management of IVD pathology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low back pain is frequent, causes high health care costs in Western industrialized countries, and is the first most costly problem in Workers’ Compensation systems [15]. The overwhelming majority of back pain is associated with degeneration of the intervertebral disc (IVD) [13]. Over the last decade, novel diagnostic and therapeutic strategies have been developed [37, 43]. Although many of the imaging and surgical difficulties have been addressed [6–8, 22, 25, 26], the mechanisms which underly the aethiopathogenesis of lumbar IVD disease remains incompletely understood [27].
The sciatica syndrome is characterized by low back pain with radiculopathy [12]. Sciatica often has a lengthy course and causes prolonged disability [21, 41]. The mechanical compression of spinal nerve root by herniated IVD is only one of the components of a complex pathophysiological mechanism leading to this clinical syndrome.
Insufficient blood supply to the IVD has been proposed to play a role as causative factor in IVD degeneration [4, 33]. There is an association between IVD diseases and increased risk of dying of ischaemic heart disease [31]. Obesity and tobacco are potential risk factors for degenerative IVD disease [10]. A genetic component has been implicated in degenerative IVD disease, but investigations into the genetic factors involved in the aetiology of this condition are still in their infancy [13, 19, 34].
A possible relationship between serum lipids and degenerative IVD disease has been proposed [20, 21]. The IVD has a complex hierarchical structure with regional variations in composition, structure, and cellular morphology and phenotypes [28, 29, 35]. It is composed of various connective tissues that undergo biochemical and structural changes with aging [5, 9, 32]. The IVD is the largest avascular structure of the human body, which relies on diffusion through the vertebral endplate for nutrition [39].
High blood cholesterol [20, 21, 40] and triglycerides [2] serum levels are risk factors for atherosclerosis, which could be responsible for a decreased in the blood supply to the already poor vascularized IVD [17]. At tissue level, structures with precarious nutrient supply, such as the IVD, may suffer [30] and gradually degenerate [17] as a consequence of failure of nutrient supply to IVD cells [42].
We undertook a cross-sectional frequency-matched case–control study of the serum lipids level obtained from patients undergoing surgery for a symptomatic lumbar disc, and compared them with a control group of patients of a similar age with musculo-skeletal pathology of the lower limb.
Materials and methods
All procedures described in this study were approved by the Ethics Committee of our Institution. All patients provided written informed consent.
The study included 384 subjects who were operated at our institution.
Group 1 included 169 patients (115 men and 54 women; mean age: 59.1 years, range 29–85) who underwent surgery for a symptomatic disc herniation in 2001 and 2008.
Group 2 (control group) included 169 patients (115 men and 54 women; mean age: 61 years, range 26–86) who underwent arthroscopic meniscectomy for a meniscal tear in the same period, and had no evidence of back pain [23, 24]. These patients were frequency-matched by age (within 3 years) and gender with patients of Group 1 (Table 1).
Patients in group 1 were included in the study if they had (a) radiculopathy, defined by unilateral radicular leg pain (L3, L4, L5, or S1) with either signs of nerve root irritation (straight leg raising test or femoral stretch test depending on the level) or neurologic deficit (motor weakness, numbness, or lack of the corresponding reflex), (b) magnetic resonance imaging signs of herniated disc, (c) refractory radicular pain despite adequate medical treatment or progressive motor weakness, and (d) electromyographic signs of radiculopathy.
Patients were excluded from the study if they had multiple IVD herniations, spondylolysis, spondylolisthesis, foraminal or central canal stenosis, and spondyloarthritis.
Patients of in Group 2 were included in the study if they had a meniscal tear diagnosed on clinical and imaging grounds, and a meniscal tear noticed at the time of surgery.
Patients were excluded from both the two groups of the study if they had primary osteoarthritis of the operated or contralateral joint, previous operations on the shoulder or knee, inflammatory joint disease, hypertension, or diabetes.
All blood samples were collected in an identical manner between 07.00 and 07.30 after an overnight fast started at 12.00 midnight. Biochemical analyses of blood were performed on fresh samples. A five millilitre blood sample was taken from the patients into tubes (Vacutainer System, Becton–Dickinson, NJ, USA), and centrifuged at 3,500 rpm for 10 min. Sera were extracted from the samples and the concentrations of total cholesterol (TC) and triglycerides (TG) were by enzymatic methods with the CIBA Corning 550 Express Autoanalyzer (Boehringer Mannheim, Mannheim, Germany). Patients were considered to have established hypercholesterolaemia at levels >6.2 mmol/L, and light hypercholesterolaemia at levels between 5.2 and 6.2 mmol/L [1]. Patients were considered to have established hypertriglyceridemia at levels >4.5 mmol/L [1].
Statistics
Data were entered in a commercially available database. Descriptive statistics were calculated, and analytical statistics were performed with non-paired sample t test using Statistical Programs for the Social Sciences (SPSS). Significance was set at P < 0.05.
Results
The serum concentrations of triglyceride and total cholesterol were measurable in all patients.
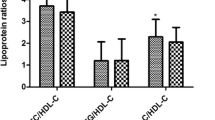
When comparing the two groups, patients with symptomatic herniated disc showed statistically significant higher triglyceride concentration (P = 0.02) and total cholesterol concentration (P = 0.01) (Tables 2 and 3).
Group 1
In Group 1 (symptomatic disc herniation), triglyceride concentration was >4.5 mmol/L in eight patients. No patients were under treatment for high serum triglyceride levels. In the same group, total cholesterol concentration was >6.2 mmol/L in 53 of 169 patients. Light hypercholesterolaemia (5.2–6.2 mmol/L) was present in 50 of 169 patients. No patients were under treatment for high serum cholesterol levels.
Group 2
In Group 2 (control group), triglyceride concentration was >4.5 mmol/L in five patients. No patients were under treatment for high serum triglyceride levels. In the same group, total cholesterol concentration was >6.2 mmol/L in 39 of 169 patients. Light hypercholesterolaemia (5.2–6.2 mmol/L) was present in 37 of 169 patients. No patients were under treatment for high serum cholesterol levels.
Discussion
We compared the serum lipids level from patients undergoing surgery for a symptomatic lumbar disc herniation, and compared them with a control group of patients of a similar age with musculo-skeletal pathology of the lower limb in a cross-sectional frequency-matched case–control study. Patients with a symptomatic disc herniation had statistically higher serum cholesterol and triglycerides lipid levels than a control group with musculo-skeletal pathology of the lower limb.
Strength of the present study includes the systematic collection of blood samples, the use of pre-operative imaging and surgery to diagnose disc herniation and meniscal tears, and the relatively large sample size of our study group. Nevertheless, we acknowledge the cross-sectional nature of the present investigation, which cannot completely resolve issues concerning temporality. Another limitation of our study was that we have no data about high-density lipoprotein (HDL), low-density lipoprotein (LDL), and very low-density lipoprotein (VLDL) concentrations in our patients. More detailed analysis could reveal lipoprotein abnormalities. The association between LDL and HDL cholesterol and the development of coronary heart disease is well established [14], and the management of coronary heart disease has traditionally focused on reduction of LDL cholesterol or of the total lipid profile [36]. We do not know whether such strategies might exert a beneficial effect on IVD problems as well. We are fully aware that more anthropometric measures could be performed (for example, waist and hip girth, and skin-fold measurements). Unfortunately, we did not collect these data in our patients: this could be the subject of future endeavours.
A correlation between higher serum lipid level and sciatica has been showed in Finnish patients [20, 21]. However, in those investigations, patients were assessed by interview and clinical examination, but no confirmation of the underlying pathology was made using imaging. One of the strengths of the present study is that all our patients received a clinical, electromyographical, radiological, and surgical diagnosis of herniated disc. Moreover, we are not aware of any study detailing the cholesterol and triglyceride serum levels in patients with a symptomatic disc herniation in the general Italian adult population.
We do not have information on the physical activity of our patients, and this is a major limitation of this study, as physical activity is inversely associated with lipid levels [3]. There are other confounding factors that preclude definitive conclusions. For example, we were not able to include the activity level of our patients in our study and we do not know whether patients with meniscal tears can be less active than patients with the disc herniation and if the activity level is a confounding factor. Also, we did not make a distinction about the presence of degenerative disc disease versus the presence of a disc herniation with radiculopathy. IVD pathology is a spectrum of disease. Therefore, there is a subset of patients that can have a herniated disc without the previous clinical or radiographic evidence of disc degeneration. Similarly, there are patients that can have symptomatic or asymptomatic lumbar spondylosis without a disc herniation.
Moreover, even though there may be a statistically significant difference between the two Groups, in terms of absolute amount/concentration, the difference was very small. Within the general population it is likely that many people have similar values, without a disc herniation. Larger studies on the topic could clarify this point.
There is some evidence that atheromatous lesions in the abdominal aorta may be related to IVD degeneration and long-term back symptoms, as demonstrated by MR aortography [17]. We did not perform such imaging investigation. However, this was dictated by practicalities, as it would have been difficult, if not impossible, to perform a MR aortography for all our patients in our setting, as this would have overloaded our imaging team. Again, this could be the subject of further, more refined studies.
The precise mechanisms that give rise to a symptomatic disc herniation and the aetiology of IVD disease remain unclear. Combinations of many factors play a role in the development of degenerative IVD disease. The association between IVD degeneration and adiposity has been examined. Elevated adiposity can be frequently associated with IVD degeneration. Limited data suggests that elevated adiposity develops prior to IVD degeneration, although firm conclusions cannot yet be reached [11].
Theoretically, obesity may contribute to decreased vascularity through its associations with risk factors for vascular disease, such as elevated cholesterol [18], atherosclerosis [16], diabetes, hypertension, metabolic syndrome and decreased physical activity [38].
The IVD is poorly vascularized, and it receives blood supply through diffusion through the vertebral endplate. High blood cholesterol [20, 21, 40] and triglycerides [2] serum levels are risk factors for atherosclerosis, which could be responsible for a decreased in the blood supply to the already poor vascularized IVD [17]. At tissue level, structures with precarious nutrient supply, such as the IVD, may suffer [30] and gradually degenerate [17], as a consequence of failure of nutrient supply to disc cells [42].
In conclusion, there appears to be an association between serum lipids level and a symptomatic disc herniation. As this was a cross-sectional study, we could not determine temporality or rule out other factors that may influence IVD degeneration process. Additional research is required to improve our understanding of aethiopathogenesis of IVD degeneration.
References
Andreoli M (2000) Manuale medico di endocrinologia a metabolismo. Il pensiero scientifico:691–718
Austin MA, Hokanson JE, Edwards KL (1998) Hypertriglyceridemia as a cardiovascular risk factor. Am J Cardiol 81:7–12
Bassuk SS, Manson JE (2003) Physical activity and the prevention of cardiovascular disease. Curr Atheroscler Rep 5:299–307
Battie MC, Videman T, Gill K, Moneta GB, Nyman R, Kaprio J, Koskenvuo M (1991) 1991 Volvo Award in clinical sciences. Smoking and lumbar intervertebral disc degeneration: an MRI study of identical twins. Spine 16:1015–1021
Boudriot U, Schmitt J, Pfeiffer M (2005) Thoracic herniation after lumbar spine fusion. Arch Orthop Trauma Surg 125:493–498
Denaro L, Longo UG, Denaro V (2009) Vertebroplasty and kyphoplasty: reasons for concern? Orthop Clin North Am 40:465–471 viii
Denaro L, Longo UG, Papalia R, Di Martino A, Maffulli N, Denaro V (2008) Eosinophilic granuloma of the paediatric cervical spine. Spine (Phila Pa 1976) 33:E936–E941
Denaro V, Longo UG, Denaro L (2010) Vertebroplasty versus conservative treatment for vertebral fractures. Lancet 376:2071 author reply 2071–2072
Echarri JJ, Forriol F (2005) Influence of the type of load on the cervical spine: a study on Congolese bearers. Spine J 5:291–296
Frymoyer JW (1988) Back pain and sciatica. N Engl J Med 318:291–300
Gaida JE, Ashe MC, Bass SL, Cook JL. Is adiposity an under-recognised risk factor for tendinopathy? A systematic review. Arthr Care Res (In press)
Genevay S, Finckh A, Payer M, Mezin F, Tessitore E, Gabay C, Guerne PA (2008) Elevated levels of tumour necrosis factor-alpha in periradicular fat tissue in patients with radiculopathy from herniated disc. Spine 33:2041–2046
Gilbertson L, Ahn SH, Teng PN, Studer RK, Niyibizi C, Kang JD (2008) The effects of recombinant human bone morphogenetic protein-2, recombinant human bone morphogenetic protein-12, and adenoviral bone morphogenetic protein-12 on matrix synthesis in human annulus fibrosis and nucleus pulposus cells. Spine J 8:449–456
Gotto AM (1998) Triglyceride as a risk factor for coronary artery disease. Am J Cardiol 5:22Q–25Q
Hegmann KT, Moore JS (1998) Common neuromusculoskeletal disorders. In: King PM (ed) Sourcebook of occupational rehabilitation. Plenum, New York, pp 30–32
Hubert HB, Feinleib M, McNamara PM, Castelli WP (1983) Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 67:968–977
Kauppila LI, Mikkonen R, Mankinen P, Pelto-Vasenius K, Maenpaa I (2004) MR aortography and serum cholesterol levels in patients with long-term nonspecific lower back pain. Spine 29:2147–2152
Kim KS, Owen WL, Williams D, Adams-Campbell LL (2000) A comparison between BMI and conicity index on predicting coronary heart disease: the Framingham Heart Study. Ann Epidemiol 10:424–431
Larson JW 3rd, Levicoff EA, Gilbertson LG, Kang JD (2006) Biologic modification of animal models of intervertebral disc degeneration. J Bone Joint Surg Am 88(Suppl 2):83–87
Leino-Arjas P, Kaila-Kangas L, Solovieva S, Riihima H, Kirjonen J, Reunanen A (2006) Serum lipids and low back pain-an association? A prospective study of a normal working population sample. Spine 31:1032–1037
Leino-Arjas P, Kauppila L, Kaila-Kangas L, Shiri R, Heistaro S, Heliovaara M (2008) Serum lipids in relation to sciatica among Finns. Atherosclerosis 197:43–49
Longo UG, Denaro V (2009) Spinal augmentation: what have we learnt? Lancet 373:1947 author reply 1947–1948
Longo UG, Franceschi F, Ruzzini L, Spiezia F, Maffulli N, Denaro V (2009) Higher fasting plasma glucose levels within the normoglycaemic range and rotator cuff tears. Br J Sports Med 43:284–287
Longo UG, Franceschi F, Spiezia F, Forriol F, Maffulli N, Denaro V (2010) Triglycerides and total serum cholesterol in rotator cuff tears: do they matter? Br J Sports Med 44:948–951
Longo UG, Loppini M, Denaro L, Maffulli N, Denaro V (2010) Rating scales for low back pain. Br Med Bull 94:81–144
Longo UG, Papapietro N, Maffulli N, Denaro V (2009) Thoracoscopy for minimally invasive thoracic spine surgery. Orthop Clin North Am 40:459–464 vii
Longo UG, Ripalda P, Denaro V, Forriol F (2006) Morphologic comparison of cervical, thoracic, lumbar intervertebral discs of cynomolgus monkey (Macaca fascicularis). Eur Spine J 15:1845–1851
Maiuri F, Iaconetta G, Gambardella A (2000) Ossification of the yellow ligament causing thoracic cord compression. Arch Orthop Trauma Surg 120:346–348
Maiuri F, Iaconetta G, Gambardella A, Buonamassa S (2000) Cervical spine stenosis due to ossification of the posterior longitudinal ligament in Italian patients: surgical treatment and outcome. Arch Orthop Trauma Surg 120:441–444
Mitchell JRA, Adams JH (1977) Aortic size and aortic calcification: a necropsy study. Atherosclerosis 27:437–446
Penttinen J (1994) Back pain and risk of fatal ischaemic heart disease: 13 year follow up of Finnish farmers. Bmj 309:1267–1268
Post RB, Leferink VJ (2004) Spinal mobility: sagittal range of motion measured with the SpinalMouse, a new non-invasive device. Arch Orthop Trauma Surg 124:187–192
Ratcliffe JF (1982) The anatomy of the fourth and fifth lumbar arteries in humans: an arteriographic study in one hundred live subjects. J Anat 135:753–761
Risbud MV, Guttapalli A, Tsai TT, Lee JY, Danielson KG, Vaccaro AR, Albert TJ, Gazit Z, Gazit D, Shapiro IM (2007) Evidence for skeletal progenitor cells in the degenerate human intervertebral disc. Spine 32:2537–2544
Roughley PJ (2004) Biology of intervertebral disc aging and degeneration: involvement of the extracellular matrix. Spine 29:2691–2699
Schaefer EJ, Asztalos BF (2006) The effects of statins on high-density lipoproteins. Curr Atheroscler Rep 8:41–49
Scuderi GJ, Brusovanik GV, Anderson DG, Dunham CJ, Vaccaro AR, Demeo RF, Hallab N (2006) Cytokine assay of the epidural space lavage in patients with lumbar intervertebral disk herniation and radiculopathy. J Spinal Disord Tech 19:266–269
Siervogel RM, Wisemandle W, Maynard LM, Guo SS, Chumlea WC, Towne B (2000) Lifetime overweight status in relation to serial changes in body composition and risk factors for cardiovascular disease: The Fels Longitudinal Study. Obes Res 8:422–430
Stairmand JW, Holm S, Urban JP (1991) Factors influencing oxygen concentration gradients in the intervertebral disc: a theoretical analysis. Spine 16:444–449
Steinberg D (2002) Atherogenesis in perspective: hypercholesterolemia and inflammation as partners in crime. Nat Med 8:1211–1217
Svensson HO, Vedin A, Wilhelmsson C, Andersson GB (1983) Low-back pain in relation to other diseases and cardiovascular risk factors. Spine 8:277–285
Urban JPG, Roberts S (2003) Degeneration of the intervertebral disc. Arthritis Res Ther 5:120–130
Vaccaro AR, Fehlings MG (2007) The applicability of clinical equipoise and sham surgery in patients with symptomatic lumbar radiculopathy due to a herniated disc: the SPORT trial. Spine 32:2039–2040
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
All procedures described in this study were approved by the Ethics Committee of our Institution. All patients provided written informed consent.
Rights and permissions
About this article
Cite this article
Longo, U.G., Denaro, L., Spiezia, F. et al. Symptomatic disc herniation and serum lipid levels. Eur Spine J 20, 1658–1662 (2011). https://doi.org/10.1007/s00586-011-1737-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-011-1737-2