
Abstract
Purpose
Although several studies have compared the clinical efficacy of an adductor canal block (ACB) to that of a femoral nerve block (FNB) for analgesia after total knee arthroplasty (TKA), disputes mainly exist in the recovery of quadriceps strength and mobilization ability between the two methods. The aim of the present study was to compare, in a systematic review and meta-analysis, the clinical efficacy of ACB with that of FNB.
Methods
We systematically searched randomized controlled trials comparing FNB with ACB for analgesia after TKA in Pubmed and the Cochrane Library from inception to April 30th 2015. There was no limitation of publication language. Trial quality was assessed using the modified Jadad scale, and eligible data were pooled for meta-analysis.
Results
Five studies of 348 patients were included. Outcomes showed that patients who received ACB had similar or better recovery of quadriceps strength and mobilization ability than those that underwent FNB. Similar efficacy was found between the two strategies regarding adductor strength, pain scores [at rest (p = 0.86), at or after knee flexion (p = 0.31)], opioid consumption (p = 0.99), opioid-associated adverse effects (p = 0.60), length of hospital stay (p = 0.42), patient satisfaction (p = 0.57), and success rate of blockade (p = 0.20).
Conclusions
The present study suggests that TKA patients who receive ACB can achieve similar or even better recovery of quadriceps strength and mobilization ability than those treated with FNB. Taken as a whole, ACB may be a better analgesia strategy after TKA at present.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is a common and safe surgical procedure typically used for relief of symptoms in patients with severe knee osteoarthritis [1]. Despite a comprehensive multimodal analgesic regimen, 25–40 % of the patients that receive TKA will experience a severe movement-related pain in the first or second postoperative day [2]. Severe pain not only excruciates the patients, but also hinders mobilization, which may result in an increased risk of immobility-associated complications. Therefore, optimal pain relief is of great importance for functional recovery after TKA.
Many studies have indicated that the clinical efficacy of a peripheral nerve block is better than intravenous patient-controlled analgesia using opioids and epidural analgesia due to its shorter functional recovery time as well as a lower risk of adverse effects [3, 4]. As a typical example of the peripheral nerve block method, femoral nerve block (FNB) is a well-established analgesia strategy after TKA and considered by many to be the standard method [3–5]. However, patients that receive FNB usually suffer from a substantial reduction in quadriceps muscle strength [6, 7], which leads to the elevated risk of a postoperative fall [8].
To avoid the risk of postoperative falls, adductor canal block (ACB) has recently been used for TKA. Due to the fact that ACB mainly targets the sensory nerves rather than the nerve to the vastus medialis, its influence on quadriceps muscle strength is lower than that of FNB [9–11]. In addition, ACB can effectively reduce postoperative pain and morphine consumption compared with placebo after TKA [12, 13].
Considering the anatomical evidence, it is not surprising that ACB may be superior to FNB. However, outcomes of the previous studies comparing ACB with FNB did not completely support the above evidence. Although definite outcomes were conveyed from published studies regarding the similar pain relief between ACB and FNB [14–19], disputes still exist over many aspects of the efficacy between the two methods. Taking recovery of quadriceps strength and mobilization ability as examples, Kim and Memtsoudis et al. [14, 18] found no significant difference of quadriceps strength between ACB and FNB, while other authors [15, 16, 19] indicated that quadriceps strength after ACB was significantly higher than that observed in FNB groups. In addition, Grevstad et al. [15] and Shah et al. [17] concluded that the mobilization ability assessed by the Timed-Up-and-Go test (refers to the time taken for a person to rise from a chair, walk three meters, turn around, walk back to the chair, and finally sit down), was significantly better in the ACB group than in the FNB group. However, Jæger et al. [19] reported no significant difference of TUG test outcome between the two groups.
In addition to the above disputes, it should be noted that the sample size of these studies was limited (ranging from 48 to 98 patients), which may affect the accuracy of relevant conclusions. Therefore, the present controversies between FNB and ACB as well as the limited sample size of current studies necessitate an evidence-based study.
Therefore, the aim of the present study was to compare, from the perspective of a systematic review with meta-analysis pooling of outcomes with small sample size into a larger one, the clinical efficacy of ACB with that of FNB for analgesia after TKA.
Materials and methods
Study design and search strategy
All the published randomized controlled trials (RCTs) comparing FNB with ACB for TKA analgesia were searched in PubMed and Cochrane Library by two independent reviewers with no time frame restrictions. A structured search was performed using the following search string: “femoral nerve block” OR “adductor canal block”. There was no limitation of publication language.
Eligibility criteria
Only RCTs comparing FNB with ACB for analgesia after TKA were taken into consideration. Cohort studies, clinical controlled trials, and case reports were excluded. Subjects eligible for participation were elderly patients who had undergone unilateral or bilateral primary TKA and had provided a written informed consent.
Study identification
Two reviewers independently screened the titles of all the articles obtained. Any study that was potentially relevant to the topic would be reviewed first for its abstract and eventually by its full text if inadequate information was acquired from the abstract. A third reviewer would be consulted for a final decision if any disagreement on eligibility existed between the first two reviewers.
Methodological quality appraisal
Study methodological assessment was conducted using the modified Jadad scale [20], an eight-item scale designed to evaluate randomization, blinding, withdrawals and dropouts, inclusion and exclusion criteria, adverse effects, and statistical analysis (Table 1). The score for each trial ranges from 0 (lowest quality) to 8 (highest quality). Scores of 4–8 denote good to excellent (high quality) and 0–3 equate to poor or low quality. The critical appraisal was conducted by two independent reviewers and discrepancy was solved by discussion.
Outcome measures
Main outcome measures included quadriceps strength, adductor strength, mobilization ability, and pain scores at rest or after mobilization. Secondary outcomes were cumulative opioid consumption, opioid-associated adverse effects, length of hospital stay, patient satisfaction, and success rate of the blockade.
Statistical analysis
Statistical heterogeneity was evaluated using I 2 statistics, complying with Quality of Reporting of Meta-Analyses (QUOROM) guidelines [21], which describe the percentage of total variation across studies that is due to heterogeneity rather than chance. I 2 can be readily calculated from basic results obtained from a typical meta-analysis as I 2 = 100 % × (Q–df)/Q, where Q is Cochrane’s heterogeneity statistic and df represents the degrees of freedom [22]. Substantial heterogeneity exists when I 2 > 50 %. A random-effects model was adopted for all the comparisons of meta-analysis irrespective of the p value of the heterogeneity test. Dichotomous data were presented as relative risk (RR) and continuous variables as mean difference (MD), both with 95 % confidence intervals (CIs). The meta-analysis was performed by Review Manager 5.3 software (Cochrane Collaboration, Oxford, UK). A p value of ≤0.05 was considered statistically significant.
Results
Study characteristics and methodological quality assessment
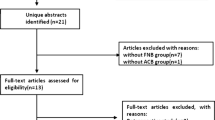
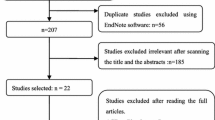
The search procedures and search outcomes were listed in Fig. 1. Altogether, six RCTs [14–19] with a total of 408 patients initially met all the inclusion criteria. Specific scores of the included RCTs are shown in Table 2, indicating that most of the studies achieved a high quality according to the current rating system. The main problem in three of the six studies was the neglect of the method used to assess adverse effects [14–16], which might have caused biases. Considering that the score of methodological assessment of the study performed by Zhang et al. [16] was comparatively low, we decided it was not qualified for the present study. Therefore, a total of five RCTs [14, 15, 17–19] with a total of 348 patients were ultimately included for analysis. One RCT [14], which compared the efficacy of the two methods in patients undergoing bilateral TKA to settle the interpatient variability, was also included. General characteristics of the five RCTs are listed in Table 3.

Flow chart of eligibility selection
Primary outcomes
Quadriceps strength
A total of four studies [14, 15, 18, 19] used two different types of scales to compare quadriceps strength between the two groups (maximum voluntary isometric contraction (MVIC) and Lafayette Manual Muscle Test System). However, only two studies could be pooled for meta-analysis [14, 18], and outcomes showed no significant differences of quadriceps strength between the ACB group and FNB group at 6–8, 24, or 48 h, postoperatively (Fig. 2).

Quadriceps strength after treatment of the ACB group and FNB group, respectively (evaluated by Lafayette Manual Muscle Test System). Forest plot showed no significant differences between the two methods at 6–8 h (p = 0.25), 24 h (p = 0.87), or 48 h (p = 0.24) postoperatively
Adductors strength
Two studies reported the adductors strength after block [15, 19] and both of them showed no significant differences of adductors strength between the two groups. Grevstad et al. [15] reported a median change of adductors MVIC from baseline of 139 % in the FNB group, compared with 107 % in the ACB group (estimated difference: 21 %, p = 0.06). Similarly, Jæger et al. [19] found that the mean adductors MVIC was 71 % of baseline data in the FNB group, compared with 78 % in the ACB group (mean difference: 7 %, p = 0.39).
Mobilization ability
Three studies [15, 17, 19] investigated patient mobilization ability after the use of ACB or FNB. Two reports showed that ACB was superior to FNB in this aspect. Grevstad et al. [15] reported that at 2 h after block, a total of seven patients in the FNB group could not perform the TUG test. However, all of the patients in the ACB group could do the test. Likewise, Shah et al. [17] found that six patients in the FNB group were not willing to do the ambulation test, whereas all patients in the ACB group performed the test.
In addition, Grevstad et al. [15] found that patients in the ACB group performed the TUG test significantly faster than those in the FNB group (32 vs 52 s, p = 0.001), which was supported by the findings of Shah et al [17] (p < 0.001). However, Jæger et al. [19] reported no statistical difference regarding the time to performing the TUG test between the two groups (p = 0.59).
Pain scores at rest
Four studies [14, 17–19] reported pain scores at rest at 24 h postoperatively. However, no significant difference was identified between the two methods [MD = 0.24, 95 % CI (−2.52, 3.00), p = 0.86] (Fig. 3). In addition to the above four studies, Grevstad et al. [15] reported pain scores at rest at 2 h postoperatively, which also showed insignificant difference between the two groups (9 vs 9 mm).

Pain scores at rest between the ACB group and FNB group at 24 h postoperatively. Pooled outcome of four studies showed no significant difference between the two groups (p = 0.86)
Pain scores at or after knee flexion
Three studies [14, 17, 19] reported pain scores at or after knee flexion at 24 h postoperatively, with no statistical difference between the two groups [MD = 4.10, 95 % CI (−3.86, 12.05), p = 0.31] (Fig. 4). In addition, Grevstad et al. [15] and Jæger et al. [19] compared pain scores between the two groups at 45-degree passive knee flexion, which also revealed no statistical differences.

Pain scores at or after knee flexion between the ACB group and FNB group at 24 h postoperatively. Pooled outcome of three studies showed no significant difference between the two groups (p = 0.31)
Secondary outcomes
Opioid consumption
Two studies [18, 19] reported opioid consumption at 24 h postanesthesia, with no significant difference between the two groups [MD = −0.03, 95 % CI (−7.38, 7.31, p = 0.99)] (Fig. 5). Kim et al. [18] also reported opioid consumption at 48 h postanesthesia and the outcome also revealed no statistical difference between the ACB group and FNB group.

Cumulative opioid consumptions between the ACB group and FNB group. Pooled outcome of two studies revealed no significant difference between the two groups (p = 0.99)
Opioid-associated adverse effects
Opioid-associated adverse effects reported in the included RCTs contained nausea and sedation, vomiting, and knee buckling (flexional deformity). Two studies [17, 18] compared the incidence of nausea and sedation between ACB and FNB, however, no significant difference was identified between the two groups [RR = 1.20, 95 % CI (0.61, 2.34), p = 0.60] (Fig. 6). Similarly, Jæger et al. [19] also indicated no statistical differences of adverse effects caused by opioids between ACB and FNB subjects.

Number of patients that suffered from adverse effects of nausea and sedation after ACB and FNB. Pooled outcome of two studies revealed no significant difference between the two groups (p = 0.60)
Length of hospital stay
Two studies [17, 18] compared length of hospital stay between the two groups and no significant difference was found [MD = −0.38, 95 % CI (−1.30, 0.54), p = 0.42] (Fig. 7).

Length of hospital stay between ACB group and FNB group. Pooled outcome of two studies revealed no significant difference between the two groups (p = 0.42)
Patient satisfaction
Two studies [14, 18] reported patient satisfaction score between the two strategies, and likewise, we found no statistical differences between the two groups at 6–8 h postoperatively [MD = 0.17, 95 % CI (−0.09, 0.43), p = 0.20] or at 24 h postoperatively [MD = −0.34, 95 % CI (−0.90, 0.21), p = 0.23] (Fig. 8). In addition, Memtsoudis et al. [14] also reported no significant difference of patient satisfaction at 48 h postoperatively (p = 0.06). The overall outcome showed no statistical difference of patient satisfaction score between the two groups [MD = −0.10, 95 % CI (−0.45, 0.25), p = 0.57] (Fig. 8).

Patient satisfaction score between the ACB group and FNB group. Forest plot of patient satisfaction score showed no statistical difference between the two groups at 6–8 h (p = 0.20), at 24 h (p = 0.23), or at 48 h (p = 0.06), postoperatively
Success rate of blockade
Three studies [15, 17, 18] compared success rates of ACB versus FNB blockades, and the outcomes showed that no significant difference was found between the two methods [RR = 0.97, 95 % CI (0.93, 1.02), p = 0.20] (Fig. 9).

Success rate of blockade between ACB group and FNB group. Pooled outcome of three studies revealed no significant difference between the two groups (p = 0.20)
Discussion
Outcomes of the present study demonstrate that TKA patients who receive ACB can achieve similar or even better recovery of quadriceps strength and mobilization ability than those treated by FNB. In addition, we found no significant differences between the two methods regarding pain scores both at rest and after mobilization, opioid consumption, opioid-associated adverse effects, length of hospital stay, patient satisfaction, or success rate of blockade. Therefore, ACB may be a better analgesia strategy after TKA at present.
The greater achievement of ACB in terms of quadriceps strength and mobilization ability is probably associated with the different anatomical backgrounds of the two blocks. The femoral nerve, which consists of many independent nerve fibers from the lumbar plexus, is frequently approached just at or below the level of the inguinal ligament. Nerve blocking here can provide post-operative analgesia to the following sites: the entire front of the upper thigh down to and including the patella, and the medial side of the lower leg to approximately the medial malleolus of the femur. Therefore, FNB can be used for procedures of the anterior thigh and knee. As another block type of the femoral nerve, ACB is conducted further down the thigh, where much of the motor innervation of the quadriceps group has already departed the nerve. Therefore, ACB preserves much of the quadriceps strength, rendering early mobilization and rehabilitation safer.
The current controversy regarding the recovery of quadriceps strength lies in whether ACB can provide better or just similar outcomes to that achieved by FNB. After analyzing the included studies, we considered that this dispute probably originated from different scales or systems for evaluation among different studies. With regard to the adductors strength, no statistical MVIC difference was found between ACB and FNB based on two studies of 98 patients. Considering that the data provided were unavailable to pool for meta-analysis, we just described the outcomes. Mobilization ability is an indicator that reflects the recovery of muscle strength, and two of the included studies [15, 17] found that patients who received ACB may have better outcomes of mobilization ability. However, Jaeger et al. [19] indicated no significant difference in the time to perform the TUG test between the two groups. We thought that this dispute may be caused by the use of different time points for assessment. In addition, sample size is another important factor that may affect the outcomes.
Comparisons of pain scores at rest or after mobilization revealed that the analgesic effect of ACB is equivalent to that of FNB. RCTs included in our study used different time points to assess pain scores. Outcomes regarding the pain scores at rest based on four studies [14, 17–19] showed no statistical difference between the two methods at 24 h postoperatively. Likewise, the outcome of pain scores at or after knee flexion from three RCTs [14, 17, 19] also revealed insignificant differences between ACB and FNB at 24 h postoperatively. However, the heterogeneity among the three studies [14, 17, 19] was high (I 2 = 76 %), which was probably associated with different strategies (anesthetic type, dose, and concentration) for analgesia (Table 3) as well as different modes of knee flexion (flexion angle, passive or active flexion). In addition to the pooled studies at a time point of 24 h postoperatively, several studies also reported comparison outcomes at 2 h [15] and 48 h [14, 16, 17] postoperatively. However, none of these RCTs reported significant differences in pain scores between the two strategies.
With respect to the secondary outcomes, no significant differences of opioid consumption were found between the ACB group and FNB group, neither at 24 h postanesthesia [18, 19], nor at 48 h [18]. Similarly, no statistical difference was identified regarding the opioid-associated adverse effects between the two groups (ACB: 14.89 % vs FNB: 12.37 %, p = 0.60) (Fig. 9). The most frequent adverse effects reported by the included RCTs were nausea and sedation. In addition, Kim et al. [18] reported that a total of three patients suffered from buckled knee on postoperative day 1 in the FNB group and none of the three patients fell. However, no such adverse effects were reported in ACB group. Therefore, patients should be fully informed about this aspect before receiving FNB for analgesia after TKA. Although the outcome of our pooled analysis of two studies [17, 18] showed no significant difference for the length of hospital stay between the two groups (Fig. 7), a dispute still existed between the two studies. Kim et al. [18] reported that the average length of hospital stay for ACB and FNB group was 3.7 and 3.6 days, respectively (p = 0.735). However, Shah et al. [17] found a significantly longer period in the FNB group (3.92 vs 3.08 days, p < 0.001). Although the authors did not provide specific reasons for this statistical difference, we inferred that this may be associated with the fact that patients who received ACB may have a faster postoperative recovery than those by FNB. Outcomes regarding patient satisfaction revealed that similar scores were obtained between ACB and FNB groups at 6–8, 24, and 48 h postoperatively. With regard to success rates of the blockade, the outcome of the pooled analysis also revealed no statistical difference (ACB: 95.76 % vs FNB: 99.18 %, p = 0.20). Kim et al. [18] reported that the success rates for ACB and FNB were 93.6 and 97.9 %, respectively, while Shah et al. [17] found a success rate of 96 % for ACB and 100 % for FNB. Outcomes of the above success rates of the blockades imply that it may be more difficult to perform ACB, and of course, the experience of anesthetists may also affect the outcomes.
The present study had several limitations. Firstly, the number of included RCTs as well as the sample size of these studies was limited, which may cause biases. Therefore, on one hand, cautious attitude should be taken toward the outcomes. On the other hand, future studies with a larger sample size are necessary. Secondly, another source of bias and high heterogeneity among studies pooled for analysis may have originated from different strategies for both ACB and FNB. It should be noted that motor block can occur in a concentration-dependent manner. Moreover, the use of higher amount of bupivacaine and the use of continuous infusion in some of the included studies may also affect the outcomes. Therefore, more efforts should be put toward finding an optimal analgesia strategy. Finally, different assessment systems and different time points for assessment can also result in an elevated risk of biases. Therefore, future investigations should use consistent evaluation systems and adequate follow-up time to better evaluate the efficacy of the two analgesia methods.
In summary, the current study demonstrates that TKA patients who received ACB can achieve similar or even better recovery of quadriceps strength and mobilization ability than those by FNB. In addition, ACB can also achieve similar clinical efficacy as FNB does in adductors strength, pain scores, opioid consumption, opioid-associated adverse effects, length of hospital stay, patient satisfaction, and success rate of blockade. Taken as a whole, ACB may be a better strategy for analgesia after TKA at present.
References
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991–2010. JAMA. 2012;308:1227–36.
Andersen LO, Gaarn-Larsen L, Kristensen BB, Husted H, Otte KS, Kehlet H. Subacute pain and function after fast-track hip and knee arthroplasty. Anaesthesia. 2009;64:508–13.
Hebl JR, Kopp SL, Ali MH, Horlocker TT, Dilger JA, Lennon RL, Williams BA, Hanssen AD, Pagnano MW. A comprehensive anesthesia protocol that emphasizes peripheral nerve blockade for total knee and total hip arthroplasty. J Bone Joint Surg Am. 2005;87(Suppl 2):63–70.
Allen HW, Liu SS, Ware PD, Nairn CS, Owens BD. Peripheral nerve blocks improve analgesia after total knee replacement surgery. Anesth Analg. 1998;87:93–7.
Paul JE, Arya A, Hurlburt L, Cheng J, Thabane L, Tidy A, Murthy Y. Femoral nerve block improves analgesia outcomes after total knee arthroplasty: a meta-analysis of randomized controlled trials. Anesthesiology. 2010;113:1144–62.
Bauer M, Wang L, Onibonoje OK, Parrett C, Sessler DI, Mounir-Soliman L, Zaky S, Krebs V, Buller LT, Donohue MC, Stevens-Lapsley JE, Ilfeld BM. Continuous femoral nerve blocks: decreasing local anesthetic concentration to minimize quadriceps femoris weakness. Anesthesiology. 2012;116:665–72.
Charous MT, Madison SJ, Suresh PJ, Sandhu NS, Loland VJ, Mariano ER, Donohue MC, Dutton PH, Ferguson EJ, Ilfeld BM. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. 2011;115:774–81.
Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg. 2010;111:1552–4.
Kwofie MK, Shastri UD, Gadsden JC, Sinha SK, Abrams JH, Xu D, Salviz EA. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med. 2013;38:321–5.
Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor canal block versus femoral nerve block and quadriceps strength: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Anesthesiology. 2013;118:409–15.
Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand. 2011;55:14–9.
Jenstrup MT, Jaeger P, Lund J, Fomsgaard JS, Bache S, Mathiesen O, Larsen TK, Dahl JB. Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. Acta Anaesthesiol Scand. 2012;56:357–64.
Jaeger P, Grevstad U, Henningsen MH, Gottschau B, Mathiesen O, Dahl JB. Effect of adductor-canal-blockade on established, severe post-operative pain after total knee arthroplasty: a randomised study. Acta Anaesthesiol Scand. 2012;56:1013–9.
Memtsoudis SG, Yoo D, Stundner O, Danninger T, Ma Y, Poultsides L, Kim D, Chisholm M, Jules-Elysee K, Valle AGD, Sculco TP. Subsartorial adductor canal vs femoral nerve block for analgesia after total knee replacement. Int Orthop. 2015;39:673–80.
Grevstad U, Mathiesen O, Valentiner LS, Jaeger P, Hilsted KL, Dahl JB. Effect of adductor canal block versus femoral nerve block on quadriceps strength, mobilization, and pain after total knee arthroplasty. Reg Anesth Pain Med. 2015;40:3–10.
Zhang W, Hu Y, Tao Y, Liu X, Wang G. Ultrasound-guided continuous adductor canal block for analgesia after total knee replacement. Chin Med J (Engl). 2014;127:4077–81.
Shah NA, Jain NP. Is continuous adductor canal block better than continuous femoral nerve block after total knee arthroplasty? Effect on ambulation ability, early functional recovery and pain control: a randomized controlled trial. J Arthroplasty. 2014;29:2224–9.
Kim DH, Lin Y, Goytizolo EA, Kahn RL, Maalouf DB, Manohar A, Patt ML, Goon AK, Lee YY, Ma Y, Yadeau JT. Adductor canal block versus femoral nerve block for total knee arthroplasty: a prospective, randomized, controlled trial. Anesthesiology. 2014;120:540–50.
Jæger P, Zaric D, Fomsgaard JS, Hilsted KL, Bjerregaard J, Gyrn J, Mathiesen O, Larsen TK, Dahl JB. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty. Reg Anesth Pain Med. 2013;38:526–32.
Oremus M, Wolfson C, Perrault A, Demers L, Momoli F, Moride Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement Geriatr Cogn Disord. 2001;12:232–6.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62:e1–34.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Acknowledgments
The authors thank Prof. Allen P. Liang for revising this manuscript. The authors are also grateful for the support of the National Natural Science Foundation of China (Grant No. 81272052, 81572165).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors certify that they, or any members of their immediate families, have no funding or commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Additional information
Zhao X. Q. and Jiang N. contributed equally to this study.
About this article

Cite this article
Zhao, Xq., Jiang, N., Yuan, Ff. et al. The comparison of adductor canal block with femoral nerve block following total knee arthroplasty: a systematic review with meta-analysis. J Anesth 30, 745–754 (2016). https://doi.org/10.1007/s00540-016-2194-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-016-2194-1