
Abstract
Purpose
The methods for pain control after total knee arthroplasty (TKA) vary and have been extensively studied in recent years. Femoral nerve block (FNB) is used as the standard method due to its effective pain control following TKA, but it may weaken the quadriceps strength. Adductor canal block (ACB) is a newly developing analgesic protocol with fast functional recovery and good pain control after TKA. A meta-analysis was conducted to try to find out if ACB is better than FNB in pain treatment and joint functional recovery after TKA.
Methods
The databases PubMed, Web of Science, Embase, and Cochrane Library were systematically searched. Of 66 records identified, eight randomised controlled trials (RCT) involving 434 patients (504 knees) were eligible for data extraction and meta-analysis according to criteria included.
Results
Meta-analysis showed that ACB can significantly decrease visual analogue scale (VAS) score at rest within eight hours (p < 0.001) and at 24 hours (p < 0.001) after operation compared to FNB after TKA, and improve quadriceps strength (p < 0.001) and mobilization ability (p < 0.001). However, the differences in VAS score at rest at 48 hours, VAS score with activity within two days after operation, opioid consumption, hip adductor strength, patient satisfaction, and tourniquet times were not significant between the two groups.
Conclusion
ACB provide better ambulation ability, faster functional recovery and better pain control at rest after TKA compared to FNB. The use of ACB post TKA is worthy of being recommended to replace FNB as a standard analgesic protocol for pain treatment after TKA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is an effective and satisfactory surgery to treat end-stage knee arthritis [1]. However, patients following TKA usually suffer a lot from undesirable pain [2]. Analgesia used for patients with TKA post-operatively are various, such as neuraxial procedures, local anaesthetic infiltration, nerve blockade and so on. Femoral nerve block (FNB) is one of the most commonly used nerve blockade methods, which has been proven to be effective in reducing the usage rate of opioid painkiller and shortening hospital stays [3]. However, FNB may lower the quadriceps strength, delay patients’ post-operative activity time and increase the risk of falling [4].
Adductor canal block (ACB) is another analgesia and has developed gradually in recent years, which attracted extensive attention due to its higher successful pain control rate and lower complication incidence after TKA in the latest studies [5–7]. The adductor canal is a cavity surrounded by the sartorius muscle, medial femoral muscle, and the adductor muscles. ACB could relieve pain without compromising motor function through blocking the saphenous nerve which is the terminal sensory branch of the femoral nerve [5, 6]. Several recent randomized controlled trials (RCT) found that patients with ACB could suffer less pain at rest or during knee flexion, and were at decreased risk of compromising quadriceps strength and consumed less opioid painkiller after operation [7, 8].
Choosing an effective and safe analgesia is necessary to accelerate patients’ recovery after the surgery. Therefore, in the present study, we are aimed at determining whether ACB makes a better performance for post-operative pain control and functional recovery for patients after TKA compared with FNB.
Materials and methods
Search strategy
We identified randomized controlled trials from 1974 to 2nd May 2015 by searching databases including PubMed, Web of Science, Embase and Cochrane Library using the following terms: (total knee arthroplasty or total knee replacement) AND (adductor canal block or saphenous nerve block) AND (femoral nerve block). In addition, the reference lists of review articles, all reports and additional trials are also included by manual search.
Inclusion criteria
RCTs that compared the analgesic effect of ACB with FNB for TKAs were included. Given that ACB was also sometimes mentioned as saphenous nerve block, RCTs which compared saphenous nerve block with FNB were also included. The dosages and types of anaesthesia drug administrated were not limited. Eligible studies were selected based on criteria aforementioned by two reviewers. Any disagreement between them was resolved by consensus.
Data extraction
We extracted the following data from the included articles: publishing date, location of study, numbers of patients in each group, demographic data of participants including age, gender, indication for TKA, dosages and kinds of anaesthesia drug administrated, primary outcomes including visual analog scale (VAS) scores at rest and at an active flexion of knee which were evaluated within the first post-operative 48 hours; secondary outcomes containing opioid consumption within the first post-operative 24 hours; third outcomes including the quadriceps strength and hip adductor strength within the first post-operative 24 hours and mobilization ability (TUG test); and fourth outcomes containing patient satisfaction and tourniquet times. If necessary, we attempted to contact the author of the original reports to obtain further details. The data extraction was made by two reviewers. Likewise, any disagreement between them was resolved by consensus.
Study quality
Each study that was included in the analysis was assessed independently by each author. The assessment was performed using the modified Jadad scale for systematic reviews [9]. Studies achieving a score of ≥4 points were considered to be of high quality.
Statistical analysis
Review Manager Software (Revman 5.3, Cochrane Collaboration, Oxford, United Kingdom) was used for the meta-analysis. The continuous variable outcomes (VAS pain scores within the first post-operative 48 hours, opioid usage within the first post-operative 24 hours, the quadriceps strength and hip adductors within the first post-operative 24 hours and TUG test within the first post-operative 24 hours) for meta-analysis were presented as mean difference (MD) and with 95 % confidence interval (95 % CI) while dichotomous outcomes presented as odds ratio (OR) with 95 % CI. Heterogeneity among the studies was evaluated using the I² statistic and chi-squared test. Sensitivity analysis was performed to explore the impact of an individual study by deleting one study each time. Publication bias was visually examined by funnel plots.
Results
Search results
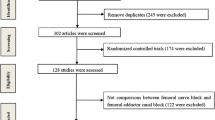
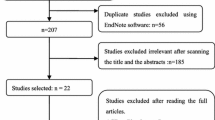
Initially, 66 records were identified from databases. Among them, 45 articles were excluded from primary screening. The remaining 21 were screened secondly to obtain potentially eligible articles. Finally, only 13 RCTs comparing ACB or saphenous nerve block with FNB were included. Unexpectedly, two works were excluded because of lack of original data and another three articles were excluded for being case control studies [10–12]. At last, eight articles were found to fulfill the inclusion criteria [13–20] (Fig. 1), which were similar to each other concerning basic characteristics (Table 1). A total of 434 patients (504 knees) were included in the eight trials: 249 patients (249 knees) in the ACB group, and 255 patients (255 knees) in the FNB group. The eight articles were assessed independently using the modified Jadad scale (minimum of four points and maximum of seven points, the average score was 6.5 points, Table 2).

Flow chart of study selection
VAS score at rest
Five studies with 418 knees showed VAS score within 8 h post-operatively, and a significant difference was found between the ACB and the FNB groups (MD = −0.17; 95 %CI, −0.27 to −0.07; Fig. 2). Five studies with 418 knees showed VAS score at 24 hours post-operatively. Meta-analysis showed that ACB had lower VAS score than the FNB group (MD = −0.41; 95 % CI, −0.53 to −0.29; Fig. 2). Only four studies with 369 knees reported the VAS score at 48 hours post-operatively. Meta-analysis revealed no significant differences between the two groups (MD= −0.06; 95 %CI, −0.15 to 0.03; Fig. 2).

Forest plot analyses of VAS pain scores at rest within post-operative 48 hours
VAS score with activity
Only three studies with 227 knees showed VAS score with activity within six hours post-operatively. No significant difference was found between the ACB and the FNB group (MD = 0.00; 95 %CI, −0.09 to 0.09; Fig. 3). Three studies with 226 knees reported VAS score at 24 hours with activity post-operatively and the results were similar in the two groups (MD = 0.04; 95 % CI, −0.11 to 0.20; Fig. 3). We included three studies with 276 knees that reported VAS score at 48 hours with activity post-operatively. The difference showed no statistical significance in the two groups (MD = −0.08; 95 % CI, −0.18 to 0.03; Fig. 3).

Forest plot analyses of VAS pain scores with activity within post-operative 48 hours
Opioid consumption
Three studies with 190 knees assessed opioid consumption at 24 hours post-operatively. The combined data showed no significant difference between the two groups (MD= −1.42; 95 %CI, − 8.41 to 5.58; Fig. 4).

Forest plot analyses of opioid consumption within post-operative 24 hours
Muscle strength
We use the quadriceps maximum voluntary isometric contraction (MVIC) to evaluate the quadriceps strength. Four studies with 135 knees showed quadriceps MVIC post-operatively. But the age of the patients revealed a big difference, so we divided patients into two subgroups: a younger group (<60 years old) and an older group (>60 years old). Meta-analysis showed that degree of knee flexion in the ACB group was much bigger than in the FNB group in both the younger group (MD = 37.46; 95 % CI, 12.27–62.24; Fig. 5) and the older group ((MD = 32.63; 95 % CI, 6.72–58.99; Fig. 5).

Forest plot analyses of quadriceps strength. Quadriceps maximum voluntary isometric contraction was used to test quadriceps strength
Four studies with 135 knees showed hip adductor strength post-operatively and we also divided them into a younger and an older group. Meta-analysis showed that the degrees abducted in the operated leg were not significantly different in the younger group (MD = 1.51; 95 % CI, –0.12 to 3.15; Fig. 6) and older group (MD = −4.87; 95 % CI, −16.13 to 6.38; Fig. 6).

Forest plot analyses of hip adductors muscle strength. The degrees abducted in the operated leg were used to test adductors muscle strength
Mobilization ability (TUG test)
Four studies with 217 knees showed TUG test post-operatively. But the age of the patients also revealed a big difference so we divided them into a younger and an older group. We found that the time cost in the ACB group was less than the FNB group both in the younger group (MD = −5.1; 95 % CI, −6.65 to −3.35; Fig. 7) and the older group (MD = −15.84; 95 %CI, −29.24 to −2.43; Fig. 7).

Forest plot analyses of mobilization ability. TUG test(s) was used to test mobilization ability
Patient satisfaction
Two studies with 211 knees assessed patient satisfaction at eight hours and at 24 hours post-operatively. The combined data showed no significant difference at eight hours between the two groups (MD = 0.17; 95 %CI, − 0.09 to 0.43), while the difference at 24 hours had statistical significance (MD = −0.63; 95 % CI, −1.18 to −0.07; Table 3).
Tourniquet time
Another two studies with 167 knees reported the tourniquet times post-operation. Meta-analysis revealed no significant differences between the two groups (MD = −0.28; 95 %CI, −4.07 to 4.63; Table 3).
Discussion
This meta-analysis was conducted try to find out if ACB is better than FNB in pain treatment and joint functional recovery, and it analyses which one is more available to be used after TKA. In the previous studies, the ACB was proven to be equivalent to the saphenous block [5, 21]. A recent meta-analysis [6] showed that saphenous nerve block has a good effect on pain relief both during activity and at rest after knee surgery. The FNB, which was supposed to be the standard method for post-operative pain treatment after TKA, had some severe side effects, such as reducing quadriceps muscle strength, delaying mobilization [13, 20] and being associated with the risk of falling [22]. The ACB, however, was not shown to have these side effects.
In our meta-analysis, the ACB group had lower pain scores in the early period of post-operation (<24 h) at rest compared to the FNB group, but the difference at 48 hours had no statistical significance. In forest plot, the I² was greater than 50 %, which means heterogeneity test shows a statistical significance. From the related trials [13–17], the heterogeneity may be caused by several reasons. First, the different race of the cases. Two trials came from Asia and six were from Europe or America. Second, two trials were bilateral TKA, while six trials were unilateral TKA, which may have an effect on the VAS scores. Third, mean age was different in the included articles. Fourth, in some of the studies, we need to estimate the mean and variance from the median, range, and the size of a sample (range= maximum–minimum). In the study of Hozo et al. [23], median can be used to estimate mean when the sample size is larger than 25. When sized samples were moderate (15 < n ≤ 70), the formula range/4 is the best estimator for the standard deviation. For large samples (n > 70), the formula range/6 gives the best estimator for the standard deviation; thus, it may influence our results.
The quadriceps strength and TUG(s) test results in the ACB group after operation were much better than that in the FNB group both in the younger group and the older group. In fact, there were many other comparisons used in the articles that can evaluate the quadriceps strength and mobilization ability. For example, quadriceps strength can be estimated by using a manual muscle test with a standardised 0–5 motor-strength scale, and the quadriceps strength was better in the ACB group [14, 17]. Furthermore, in the study of Kim et al. [15], the patient’s quadriceps strength was assessed by a neurologic exam, based on a 12-point scale, and the results were also better in the ACB group.
According to Jenstrup et al. [24], the ACB may provide unwanted analgesia by blocking these obturator fibres in addition to the femoral articular branches. But, in our meta-analysis, there were no differences in the two subgroups. Our results suggested that the ACB would not weaken the adductor muscle.
Besides the TUG test, there were many other methods for evaluating mobilization ability and similarly better results were seen in the ACB group too, with methods such as a ten metre walk test (s), 30 second chair test [20] and ambulation distance at discharge [10–12, 25].
VAS scores with activity in the two groups were similar and the opioid consumption also showed no difference. Patient satisfaction score in the two groups at eight hours after operation had no difference, while the score in the FNB group was higher at 24 hours. But only two trials were analysed and the combined data may produce bias, so we can’t consider the FNB as better. What’s more, FNB didn’t show any advantage compared with ACB for the rate of complications [15], hospital stays [15], and tourniquet times. These results may be influenced by the limited cases, but in our study, we can’t support the hypothesis that the FNB has any advantages in these fields.
According to Lund et al. [20, 26], ACB is a sensory block and theoretically it has no adverse effects on the motor function of joint. Our results demonstrate that patients with ACB had better post-operative outcomes of ambulation ability and early functional recovery such as the quadriceps strength and TUG test, in comparison to FNB after TKA. Traditionally, FNB is considered as the standard for analgesia, providing optimal pain relief after TKA [27, 28]. However, in our study, the difference in VAS scores with activity between the FNB group and the ACB group was not significant, while the VAS scores at rest were better in ACB. So, adopting ACB for patients undergoing TKA could achieve better satisfactory pain control compared with FNB.
There are several limitations to our study. First, there were only eight trials and 504 knees were included in our study, which seemed relatively small and may be the reason that there were no differences in several results of comparison, such as the VAS score with activity and opioid consumption. Furthermore, funnel plots were not available because of limited eligible studies, which haven’t shown any significance because of the limited cases. Second, the anaesthesia methods in these trials were different, which may influence the post-operative pain scores. Third, besides the ACB or FNB, many other analgesia methods were used in different trials, which may produce some bias too. Fourth, we just analysed the short-term effects after operation and didn’t know what the difference may be in the long run. Thus, further research should be done.
Conclusion
ACB provide better ambulation ability, faster functional recovery and better pain control at rest after TKA compared to FNB. The use of ACB post TKA is worthy of being recommended to replace FNB as a standard method for post-operative pain treatment after TKA.
References
Yang Z, Liu H, Xie X, Kang P et al (2014) The influence of diabetes mellitus on the post-operative outcome of elective primary total knee replacement: a systematic review and meta-analysis. Bone Joint J 96:1637–1643
Xie X, Pei F, Huang Z, Tan Z, Yang Z, Kang P (2015) Does patellar denervation reduce post-operative anterior knee pain after total knee arthroplasty? Knee Surg Sports Traumatol Arthrosc 23:1808–1815
Paul JE, Arya A, Hurlburt L, Cheng J (2010) Femoral nerve block improves analgesia outcomes after total knee arthroplasty: a meta-analysis of randomized controlled trials. Anesthesiology 113:1144–1162
Atkinson HD, Hamid I, Gupte CM (2008) Post-operative fall after the use of the 3-in-1 femoral nerve block for knee surgery: a report of four cases. J Orthop Surg (Hong Kong) 16:381–384
Andersen HL, Zaric D (2014) Adductor canal block or midthigh saphenous nerve block same but different name! Reg Anesth Pain Med 39:256–257
Jin SQ, Ding XB, Tong Y (2015) Effect of saphenous nerve block for post-operative pain on knee surgery: a meta-analysis. Int J Clin Exp Med 8:368–376
Hanson NA, Allen CJ, Hostetter LS, Nagy R (2014) Continuous ultrasound-guided adductor canal block for total knee arthroplasty: a randomized, double-blind trial. Anesth Analg 118:1370–1377
Jæger P, Koscielniak-Nielsen ZJ, Schrøder HM (2014) Adductor canal block for post-operative pain treatment after revision knee arthroplasty: a blinded, randomized, placebo-controlled study. PLoS One 9:e111951
Oremus M, Wolfson C, Perrault A, Demers L, Momoli F, Moride Y (2001) Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement Geriatr Cogn Disord 12:232–236
Rasmussen M, Kim E, Kim T et al (2015) A retrospective comparative provider workload analysis for femoral nerve and adductor canal catheters following knee arthroplasty. J Anesth 29:303–307
Patterson ME, Bland KS, Thomas LC et al (2015) The adductor canal block provides effective analgesia similar to a femoral nerve block in patients undergoing total knee arthroplasty--a retrospective study. J Clin Anesth 27:39–44
Mudumbai SC, Kim TE, Howard SK et al (2014) Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res 472:1377–1383
Grevstad U, Mathiesen O, Valentiner LS, Jaeger P, Hilsted KL, Dahl JB (2015) Effect of adductor canal block versus femoral nerve block on quadriceps strength, mobilization, and pain after total knee arthroplasty: a randomized, blinded study. Reg Anesth Pain Med 40:3–10
Memtsoudis SG, Yoo D, Stundner O, Danninger T et al (2015) Subsartorial adductor canal vs femoral nerve block for analgesia after total knee replacement. Int Orthop 39:673–680
Kim DH, Lin Y, Goytizolo EA, Kahn RL et al (2014) Adductor canal block versus femoral nerve block for total knee arthroplasty: a prospective, randomized, controlled trial. Anesthesiology 120:540–550
Shah NA, Jain NP (2014) Is continuous adductor canal block better than continuous femoral nerve block after total knee arthroplasty? Effect on ambulation ability, early functional recovery and pain control: a randomized controlled trial. J Arthroplast 29:2224–2229
Zhang W, Hu Y, Tao Y et al (2014) Ultrasound-guided continuous adductor canal block for analgesia after total knee replacement. Chin Med J (Engl) 127:4077–4081
Jæger P, Zaric D, Fomsgaard JS et al (2013) Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med 38:526–532
Kwofie MK, Shastri UD, Gadsden JC et al (2013) The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med 38:321–325
Jaeger P, Nielsen ZJ, Henningsen MH et al (2013) Adductor canal block versus femoral nerve block and quadriceps strength a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Anesthesiology 118:409–415
Lund J, Jenstrup MT, Jaeger P, Sørensen AM, Dahl JB (2011) Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand 55:14–19
Ilfeld BM, Duke KB, Donohue MC (2010) The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg 111:1552–1554
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13
Jenstrup MT, Jæger P, Lund J et al (2012) Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. Acta Anaesthesiol Scand 56:357–364
Perlas A, Kirkham KR, Billing R et al (2013) The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg Anesth Pain Med 38:334–9
Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB (2011) Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand 55:14–19
Campbell A, McCormick M, McKinlay K et al (2008) Epidural vs. lumbar plexus infusions following total knee arthroplasty: randomized controlled trial. Eur J Anaesthesiol 25:502
Fowler SJ, Symons J, Sabato S et al (2008) Epidural analgesia compared with peripheral nerve blockade after major knee surgery: a systematic review and meta-analysis of randomized trials. Br J Anaesth 100:154
Author information
Authors and Affiliations
Corresponding author
Additional information
Donghai Li and Zhouyuan Yang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Li, D., Yang, Z., Xie, X. et al. Adductor canal block provides better performance after total knee arthroplasty compared with femoral nerve block: a systematic review and meta-analysis. International Orthopaedics (SICOT) 40, 925–933 (2016). https://doi.org/10.1007/s00264-015-2998-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2998-x