
Abstract
Background
The prognosis of pancreatic cancer patients with metastatic para-aortic lymph node (PALN) has been reported to be extremely poor. In general, PALN metastasis has been considered as a contraindication for pancreatic resection. The aim of this study was to reevaluate the postoperative prognostic value of PALN metastasis in pancreatic cancer and to determine the validity of pancreatic surgery.
Methods
Retrospective multicenter analysis of 882 patients who have undergone curative-intent pancreatic resection with pathological evaluation of PALNs for pancreatic ductal adenocarcinoma between 2001 and 2012 was conducted. Clinicopathological data and outcomes were evaluated with univariate and multivariate analysis.
Results
In total, 102 (12.4 %) patients had positive metastasis in PALN. Patients with metastatic PALN had significantly poorer survival than those without (17 vs. 23 months; p < 0.001). Multivariable analysis of 822 patients identified adjuvant chemotherapy, primary tumor status, regional lymph node metastasis, portal vein invasion, pre- and post-operative serum CA19-9 levels, and tumor grade as independent prognostic factors. In contrast, PALN metastasis did not have a significant prognostic value. Furthermore, the multivariate prognostic analysis in patients with PALN metastasis revealed that adjuvant chemotherapy and the number of metastatic PALN were significantly associated with long-term survival. Lung metastasis as initial recurrence was observed more often in patients with PALN metastasis in comparison with those without.
Conclusions
Some pancreatic cancer patients with metastatic PALN may survive for longer than expected after pancreatectomy. Adjuvant chemotherapy and the number of metastatic PALN were critical factors for long-term survival of those patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pancreatic cancer has been increasing in incidence, and it is one of leading causes of cancer-related deaths worldwide [1, 2]. Despite significant progress in the treatment, the overall survival of patients remains extremely poor [3, 4]. Although surgery offers the only chance for cure or long-term survival, the majority of patients were found to be unresectable at diagnosis [5–7]. Common reasons for unresectability include vascular invasion excluding limited portal vein invasion that can be reconstructed, distant lymph node metastases, hepatic metastases, peritoneal metastases, and extra-abdominal metastases including pulmonary metastases. These surgical indications have not been much changed for many years [5, 8].
According to the TNM classification for pancreatic cancer, para-aortic lymph node (PALN) is regarded as distant lymph node and PALN metastasis is classified as distant metastasis [9, 10]. Therefore, if PALN metastasis in pancreatic cancer is suspected by preoperative images or defined by intraoperative pathological examination, pancreatic surgery is generally contraindicated. In fact, several previous studies have emphasized that the patients with metastatic PALN often had early recurrence after surgery and had extremely poor survival [11–16]. Therefore, they concluded that surgical resection did not provide survival benefit in such patients. They also discussed the need for adjuvant treatment or alternative therapeutic strategies for longer survival. However, the number of clinical studies on this issue is limited and the number of patients evaluated in each study is relatively small. Thus, there is limited clinical evidence that PALN metastasis without other distant metastasis is an absolute contraindication to pancreatic resection. In addition, due to treatment advancement including the introduction of new chemotherapeutic agents for pancreatic cancer, we occasionally see unexpected favorable outcome in daily clinical practice [17–20]. Therefore, pancreatic surgery may provide survival benefits to patients with PALN metastasis in some cases.
To address various clinical questions in the surgical treatment for pancreatic cancer including surgical indication, postoperative complications, as well as predictions of recurrence and prognosis, we have recently established a common database of seven high-volume surgical centers in Japan (Multicenter Study Group of Pancreatobiliary Surgery: MSG-PBS). By using this large-scale database, we reevaluate the postoperative prognosis of pancreatic cancer patients with PALN metastasis as a collaborative study. We further investigated risk factors for PALN metastasis and also analyzed the possibility of long-term survival in patients with metastatic PALN.
Patients and methods
Study design and data collection
This study was approved by the institutional review board of each center. We collected and registered consecutive patients who had undergone R0 or R1 pancreatic resection between 2001 and 2012 for pancreatic ductal adenocarcinoma in the database. Patients with R2 resection were not included in the database. Furthermore, patients with distant metastasis such as liver or peritoneal metastasis were also excluded from the database, even if the combined resection of metastatic sites with the primary lesion was performed. From 1,414 patients registered in the database, 592 whose PALNs had not been sampled for pathological examination were excluded. The data of a total of 822 patients with pathological proof of PALN status were collected from the database.
Para-aortic lymph nodes were sampled by harvesting the lymphocellular aortocaval tissue from the upper part of the celiac trunk to the upper part of the origin of the inferior mesenteric artery [11–13]. These lymph nodes were classified as No. 16, according to the Japanese classification [21].
Clinical data included gender, age, body mass index (BMI), neoadjuvant treatment, adjuvant chemotherapy, pre- and post-operative serum CA19-9 level, tumor location, and operation type. For tumors, pathological data included T and N status according to the 7th AJCC/UICC TNM classification, tumor size, histological type, surgical margin status, and portal vein invasion [9, 10]. Some patients received neoadjuvant treatment using chemotherapy or chemoradiotherapy depending on each institution’s decision with informed consent. Postoperative adjuvant treatment of gemcitabine- or S-1-based chemotherapy was employed depending on the physicians’ choice or the patients’ condition.
The primary endpoint of this study was to evaluate the postoperative prognosis of pancreatic cancer patients with PALN metastasis in comparison with those without. Secondary endpoints included the assessment of risk factors for PALN metastasis and the analysis of prognostic factors in patients with PALN metastasis.
Statistical analysis
The clinicopathological parameters were compared between patients with and without PALM metastasis using Student’s t test, the Chi-square test, or Fisher’s exact test as appropriate. Continuous variables were expressed as mean values ± standard deviation. The median survival was estimated using the Kaplan–Meier method, and the difference was tested using the log-rank test. Patients alive at the time of follow-up point were censored. Date of last follow-up was June 2013. Univariate and multivariate analyses were performed by the Cox proportional hazards model to evaluate significant prognostic predictors and their relative role. Statistical analyses were performed using JMP statistical discovery software (JMP version 11.0, SAS Institute, Cary, NC, USA). A p value < 0.05 was considered statistically significant.
Results
Correlations of clinicopathological factors with para-aortic lymph node metastasis
Among a total of 822 patients, pancreatoduodenectomies were performed in 617 patients (75.1 %), distal pancreatectomies in 161 patients (19.6 %), and total pancreatectomies in 44 patients (5.3 %). The 30-day and 90-day mortality rates were 0.7 and 2.9 %, respectively. The mean and median numbers of PALNs sampled for pathological examination were 4.3 (standard deviation, 4.2) and 3 (range, 1–27), respectively. As a result, while PALNs were negative for metastasis in 720 patients, they were positive in 102 patients (12.4 %). The mean and median numbers of metastatic PALNs were 1.9 (standard deviation, 1.6) and 1 (range, 1–11), respectively. Sixty patients (58.8 %) had single metastasis in PALNs, while 42 (41.2 %) had multiple metastasis.
Between patients with and without PALN metastasis, there were no significant differences in various clinicopathological factors including gender, age, BMI, neoadjuvant treatment, adjuvant chemotherapy, tumor size, tumor location, tumor differentiation, and portal vein invasion (Table 1). In contrast, PALN metastasis significantly correlated with R1 resection, advanced primary tumor status, regional lymph node metastasis, and elevated pre- and post-operative serum CA19-9 levels. In patients with metastatic PALN, only three patients had T1 tumor and/or no regional lymph node metastasis. While approximately two-thirds (72.3 %) of the patients without PALN metastasis had normal CA19-9 levels after surgery, more than half (55.0 %) of patients with PALN metastasis still had elevated CA19-9 levels.
Survival of patients according to para-aortic lymph node metastasis status
There was a significant difference in overall survival between patients with and without PALN metastasis (p < 0.001; Fig. 1a). The median survival time (MST) for patients with and without PALN metastasis were 16.9 and 22.6 months, respectively. The 1-, 2-, 3-, and 5-year survival rates were for patients with PALN metastasis were 63.8, 30.0, 16.7, and 6.8 %, respectively, compared with 74.6, 48.4, 35.6, and 25.4 % for patients without PALN metastasis.

Kaplan–Meier analysis of overall survival. a Patients with para-aortic lymph node (PALN) metastasis (n = 102) had worse survival compared to those without (n = 720). b Postoperative survival of patients with PALN metastasis operated in the year of 2006–2010 (n = 58) was better than that in 2001–2005 (n = 25)
To evaluate the change and improvement of treatment outcome during the study period, we compared the prognosis of patients with PALN metastasis treated in the first 5 years of 2001–2005 with that in the latter 5 years of 2006–2010. For data accuracy, we excluded patients operated on between 2011 and 2012 with a follow-up of less than 30 months from this analysis. The survival of patients with PALN metastasis treated in the latter period was significantly better than that of patients in the first half period (p < 0.001; Fig. 1b). The MST for patients treated in the first and latter half period were 9.3 and 18.2 months, respectively.
Univariate and multivariate survival analyses
Using the Cox proportional hazards model, we examined prognostic factors in 822 patients with pancreatic adenocarcinoma. In univariate analysis, factors associated with better patient survival included the administration of adjuvant chemotherapy, R0 resection, T1-2 tumor, negative regional lymph node metastasis, no portal vein invasion, a preoperative value of CA19-9 ≤100 units/ml, normal level of postoperative CA19-9, high-grade differentiation of tumor, and negative PALN metastasis (Table 2). On the other hand, gender, age, neoadjuvant treatment, and tumor location did not correlate with prognosis. Multivariable analysis indicated that adjuvant chemotherapy, T status, N status, portal vein invasion, and pre- and post-operative CA19-9 level, and tumor grade had significant prognostic value (Table 2). In contrast, not only R status but also PALN metastasis did not have prognostic value.
Factors for long-term survival in patients with para-aortic lymph node metastasis
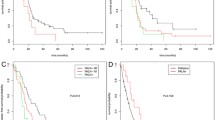
Among 102 patients with PALN metastasis, 39 (38.2 %) died within 1 year after surgery. On the other hand, 63 patients (61.8 %) survived for over 1 year, 26 (25.5 %) for over 2 years, 13 (12.7 %) for over 3 years, and two (2.0 %) for over 5 years. To investigate predictive factors for long-term survival in patients with PALN metastasis, we further performed survival analysis in these patients. As a result, adjuvant chemotherapy and the number of metastatic PALN were found to be significant independent predictors of long-term survival (Table 3). In contrast, the total number of metastatic regional lymph nodes and postoperative CA19-9 level did not have significant prognostic value in patients with PALN metastasis. The MST of patients with adjuvant chemotherapy was 23.6 months, while that without adjuvant chemotherapy was 10.6 months (Fig. 2a). In addition, the MST of patients with single PALN metastasis was 22.1 months, while that with multiple PALN metastasis was 12.8 months. Furthermore, MST of patients with two metastatic PALNs was 11.7 months, and that with more than two metastatic PALNs was 16.9 months. Although the difference between these two groups was not significant, both were significantly worse that that of patients with single PALN metastasis (Fig. 2b).

Kaplan–Meier analysis of overall survival in patients with para-aortic lymph node (PALN) metastasis. a Patients with adjuvant chemotherapy (n = 44) had better survival than those without (n = 58) (p < 0.001). b Patients with single PALN metastasis (n = 60) had better survival than those with two metastatic PALNs (p = 0.001, n = 23) or more than two metastatic PALNs (p = 0.018, n = 19)
Postoperative recurrence pattern according to para-aortic lymph node metastasis status
At the time of analysis, 516 patients (71.7 %) without PALN metastasis had recurrence. On the other hand, there were significantly more recurrences in patients with PALN metastasis (n = 91, 89.2 %, p < 0.001). Finally, we compared the initial recurrence pattern between patients with PALN metastasis and those without (Table 4). There were no significant differences in the frequency of hepatic, local, and peritoneal recurrence as initial recurrence. In contrast, lung metastasis was observed more often in patients with PALN metastasis than those without (p = 0.012).
Discussion
In the past several years, some progress has been made in the treatment for pancreatic cancer [5]. However, patient prognosis remains extremely poor and surgical indication has not been greatly changed. In general, pancreatic cancer with distant metastasis such as liver, lung, and peritoneal metastasis is thought to be systemic and incurable disease. Therefore, even if clinically apparent distant metastasis is a single lesion, surgery has usually been contraindicated. Para-aortic lymph nodes have been classified as non-regional lymph nodes and cancer cells existing in PALN are recognized as distant metastasis [9, 10]. To date, there are only a limited number of studies on the postoperative prognosis in patients with PALN metastasis [11–16]. These previous studies reported that the median survival time of patients with metastatic PALN was only between 5.1 and 15.7 months. Furthermore, early recurrence and little benefit of surgery have been described [11, 13]. These clinical data have supported that PALN metastasis is a common reason for unresectability in pancreatic cancer. However, this large-scale collaborative study has demonstrated that the prognosis of pancreatic cancer patients with PALN metastasis in the current study seems to be better than that in previous studies (Table 5). Furthermore, this study also clarified that the prognosis of those patients has been improved during the study period. The median overall survival was approximately 9 months in patients treated between the years 2001 and 2005. This is comparable to that shown in previous reports. In contrast, the median overall survival is up to 18 months in patients treated in the most recent 5 years. In fact, whereas Doi et al. reported that PALN metastasis was the only independent prognostic factor for resectable pancreatic cancer, multivariable analysis of this study demonstrates that it no longer has an independent prognostic value [13]. Recent clinical trials to evaluate new chemotherapeutic regimens including FOLFILINOX or nab-paclitaxel plus gemcitabine have demonstrated significantly improved survival for metastatic pancreatic cancer with the median survival times of 11.1 and 8.5 months, respectively [22, 23]. Even in comparison with these latest data for metastatic pancreatic cancer, the median overall survival of about 18 months is likely to be better, suggesting that there may be some differences in the tumor behavior of pancreatic cancer between PALN metastasis and other types of distant metastasis.
The precise reasons for the improved survival of patients with PALN metastasis are not fully elucidated. One of the major reasons is most likely to perform adjuvant chemotherapy. In Japan, gemcitabine was approved in 2001 and S-1 in 2006 for the treatment of pancreatic cancer. These chemotherapeutic reagents occasionally bring unexpectedly favorable clinical outcomes. In addition, recent randomized clinical trials indicating the efficacy of gemcitabine in adjuvant settings encourage surgeons and oncologists to employ adjuvant chemotherapy more actively than before [24, 25]. In this study, approximately 20 % of patients with PALN metastasis received neoadjuvant treatment and 43 % received adjuvant chemotherapy. Other various efforts in an adjuvant setting and after postoperative recurrence might have contributed to improve patient survival [20, 26, 27].
Preoperative diagnosis of PALN metastasis is not always easy, even when using the latest imaging technology [28, 29]. In daily clinical practice, enlarged PALNs suspicious of metastasis or inflammation are sometimes encountered. The enlarged PALN may be thought to be a distant metastasis and the reason for unresectability in some institutions, even if it is not pathologically proven. In the United States and Europe, the sampling of PALNs does not seem a routine procedure during surgery. Therefore, the actual rate of metastatic PALN in pancreatic cancer is unknown. However, even with the small number of PALN sampling of 4.3, the metastatic rate in PALN of 12 % in this analysis is not low and cannot be ignored. Previous studies have demonstrated that several factors including tumor size, surgical margin, postoperative CA19-9 level, extrapancreatic nerve invasion, age, and portal vein invasion were associated with PALN metastasis [11, 12, 30]. Our data, including R status, pre- and post-operative CA19-9 levels, corroborate some of the previous reports. On the other hand, Nagai et al. have reported that even T1 and T2 primary tumors of pancreatic cancer had a relatively high rate of PALN metastasis [31]. In this series, two T1 primary tumors had PALN metastasis. Furthermore, Hirono et al. have reported that there is a direct lymphatic drainage pathway from the pancreatic head to the PALN area [32]. Taken together, although PALN metastasis is a common feature of pancreatic cancer, it may occur at a relatively early stage before metastasizing to other distant organs.
Previous studies have shown that there were no or very few long-term survivors after pancreatic resection for the patients with PALN metastasis [11–13]. In contrast, 26 out of 102 patients with metastatic PALN survived for over 2 years and 13 for over 3 years. We then analyzed the conditions for long-term survival after pancreatic resection for patients with PALN metastasis. As a result, adjuvant chemotherapy and the number of metastatic PALNs were independent prognostic factors in patients with PALN metastasis. Data suggested that multimodal treatment including surgery and chemotherapy might lead to long-term survival in some patients, especially with single PALN metastasis. To consider future strategy, we analyzed the initial recurrence pattern. The pattern did not differ much between patients with PALN metastasis and those without. However, only lung metastasis was observed more often in patients with PALN metastasis, although the underlying mechanism is unclear at present. Data suggested that a more effective systemic anticancer treatment was needed. As demonstrated in recent clinical trials, several promising chemotherapy regimens may further improve postoperative prognosis of PALN-positive patients [22, 23].
There are several limitations in this study. Firstly, the sampling of PALNs was performed based on the surgeon’s decision at each institution. Furthermore, massive PALN metastases even in patients without any other distant metastases might be considered to be contraindications in most cases. Therefore, actual status of PALN remained unknown in all patients. Secondly, this study is retrospective and the true significance of pancreatic resection remains unknown. Thirdly, since this is multi-institutional study, each institution has different treatment strategies including neoadjuvant and adjuvant treatment. Such inter-institutional differences can affect the analyzed data. Therefore, in order to obtain medical evidence and to evaluate surgical indications precisely, prospective clinical studies, especially under current circumstances, need to be done. However, since this study is the largest as well as the first multicenter investigation to explore the postoperative prognosis of patients with PALN metastasis, our data may provide useful information on surgical indications and multimodal treatment for advanced pancreatic cancer.
In conclusion, some pancreatic cancer patients with PALN metastasis may survive for longer than expected after pancreatectomy. To expect long-term survival in those patients, adjuvant chemotherapy and single PALN metastasis are critical factors.
References
Ma J, Siegel R, Jemal A. Pancreatic cancer death rates by race among US men and women, 1970–2009. J Natl Cancer Inst. 2013;105:1694–700.
Egawa S, Toma H, Ohigashi H, Okusaka T, Nakao A, Hatori T, et al. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas. 2012;41:985–92.
Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clin Oncol. 2013;31:1640–8.
Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–6.
Paulson AS, Tran Cao HS, Tempero MA, Lowy AM. Therapeutic advances in pancreatic cancer. Gastroenterology. 2013;144:1316–26.
Konstantinidis IT, Warshaw AL, Allen JN, Blaszkowsky LS, Castillo CF, Deshpande V, et al. Pancreatic ductal adenocarcinoma: is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a “true” R0 resection? Ann Surg. 2013;257:731–6.
Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg. 2008;247:456–62.
Tamm EP, Balachandran A, Bhosale PR, Katz MH, Fleming JB, Lee JH, et al. Imaging of pancreatic adenocarcinoma: update on staging/resectability. Radiol Clin North Am. 2012;50:407–28.
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471–4.
Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors. 7th ed. New York: Wiley; 2010.
Shimada K, Sakamoto Y, Sano T, Kosuge T. The role of paraaortic lymph node involvement on early recurrence and survival after macroscopic curative resection with extended lymphadenectomy for pancreatic carcinoma. J Am Coll Surg. 2006;203:345–52.
Murakami Y, Uemura K, Sudo T, Hashimoto Y, Yuasa Y, Sueda T. Prognostic impact of para-aortic lymph node metastasis in pancreatic ductal adenocarcinoma. World J Surg. 2010;34:1900–7.
Doi R, Kami K, Ito D, Fujimoto K, Kawaguchi Y, Wada M, et al. Prognostic implication of para-aortic lymph node metastasis in resectable pancreatic cancer. World J Surg. 2007;31:147–54.
Kanda M, Fujii T, Nagai S, Kodera Y, Kanzaki A, Sahin TT, et al. Pattern of lymph node metastasis spread in pancreatic cancer. Pancreas. 2011;40:951–5.
Sakai M, Nakao A, Kaneko T, Takeda S, Inoue S, Kodera Y, et al. Para-aortic lymph node metastasis in carcinoma of the head of the pancreas. Surgery. 2005;137:606–11.
Schwarz L, Lupinacci RM, Svrcek M, Lesurtel M, Bubenheim M, Vuarnesson H, et al. Para-aortic lymph node sampling in pancreatic head adenocarcinoma. Br J Surg. 2014;101:530–8.
Satoi S, Yamaue H, Kato K, Takahashi S, Hirono S, Takeda S, et al. Role of adjuvant surgery for patients with initially unresectable pancreatic cancer with a long-term favorable response to non-surgical anti-cancer treatments: results of a project study for pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci. 2013;20(6):590–600.
Aristu J, Canon R, Pardo F, Martinez-Monge R, Martin-Algarra S, Manuel Ordonez J, et al. Surgical resection after preoperative chemoradiotherapy benefits selected patients with unresectable pancreatic cancer. Am J Clin Oncol. 2003;26:30–6.
Bickenbach KA, Gonen M, Tang LH, O’Reilly E, Goodman K, Brennan MF, et al. Downstaging in pancreatic cancer: a matched analysis of patients resected following systemic treatment of initially locally unresectable disease. Ann Surg Oncol. 2012;19:1663–9.
Masui T, Kubota T, Aoki K, Nakanishi Y, Miyamoto T, Nagata J, et al. Long-term survival after resection of pancreatic ductal adenocarcinoma with para-aortic lymph node metastasis: case report. World J Surg Oncol. 2013;11:195.
Japan Pancreas Society. Classification of pancreatic carcinoma (2nd English edition). Japan Pancreas Society e: Kanehara & Co.; 2003.
Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–703.
Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–77.
Ueno H, Kosuge T, Matsuyama Y, Yamamoto J, Nakao A, Egawa S, et al. A randomised phase III trial comparing gemcitabine with surgery-only in patients with resected pancreatic cancer: Japanese Study Group of Adjuvant Therapy for Pancreatic Cancer. Br J Cancer. 2009;101:908–15.
Sho M, Tanaka T, Yamada T, Nomi T, Akahori T, Doh J, et al. Novel postoperative adjuvant strategy prevents early hepatic recurrence after resection of pancreatic cancer. J Hepatobiliary Pancreat Sci. 2011;18:235–9 (discussion 9–40).
Murakami Y, Uemura K, Sudo T, Hashimoto Y, Nakashima A, Kondo N, et al. Long-term results of adjuvant gemcitabine plus S-1 chemotherapy after surgical resection for pancreatic carcinoma. J Surg Oncol. 2012;106:174–80.
Imai H, Doi R, Kanazawa H, Kamo N, Koizumi M, Masui T, et al. Preoperative assessment of para-aortic lymph node metastasis in patients with pancreatic cancer. Int J Clin Oncol. 2010;15:294–300.
Matsumoto I, Shirakawa S, Shinzeki M, Asari S, Goto T, Ajiki T, et al. 18-Fluorodeoxyglucose positron emission tomography does not aid in diagnosis of pancreatic ductal adenocarcinoma. Clin Gastroenterol Hepatol. 2013;11:712–8.
Yamada S, Nakao A, Fujii T, Sugimoto H, Kanazumi N, Nomoto S, et al. Pancreatic cancer with paraaortic lymph node metastasis: a contraindication for radical surgery? Pancreas. 2009;38:e13–7.
Nagai H, Kuroda A, Morioka Y. Lymphatic and local spread of T1 and T2 pancreatic cancer. A study of autopsy material. Ann Surg. 1986;204:65–71.
Hirono S, Tani M, Kawai M, Okada K, Miyazawa M, Shimizu A, et al. Identification of the lymphatic drainage pathways from the pancreatic head guided by indocyanine green fluorescence imaging during pancreaticoduodenectomy. Dig Surg. 2012;29:132–9.
Conflict of interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sho, M., Murakami, Y., Motoi, F. et al. Postoperative prognosis of pancreatic cancer with para-aortic lymph node metastasis: a multicenter study on 822 patients. J Gastroenterol 50, 694–702 (2015). https://doi.org/10.1007/s00535-014-1005-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-014-1005-4