
Abstract
Purpose
The aims of this review were to (1) examine the effectiveness of Internet-based interventions on cancer chemotherapy-related physical symptoms (severity and/or distress) and health-related quality of life (HRQOL) outcomes and (2) identify the design elements and processes for implementing these interventions in oncology practices.
Methods
A systematic review was performed. The Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials, EMBASE, MEDLINE, CINAHL, and PsycINFO were searched for studies dating from January 2000 through to October 2016. Based on pre-determined selection criteria, data was extracted from eligible studies. Methodological quality of studies was assessed using an adapted version of the Cochrane Collaboration Back Review Group checklist.
Results
The literature search yielded 1766 studies of which only six RCTs fulfilled the eligibility criteria. Although the content, duration, and frequency of interventions varied considerably across studies, commonly used elements included tailored information, education, self-management support, and communication with clinicians. Five studies measured symptom distress and four of them reported statistically significant differences between study groups. Of the three studies that measured HRQOL, two reported improvement (or no deterioration over time) for the intervention group. However, several methodological issues including high attrition rates, poor adherence to interventions, and use of non-validated measures affect confidence in the strength of evidence.
Conclusion
Despite the evidence in support of using the Internet as a worthwhile tool for effective patient engagement and self-management of chemotherapy-related symptoms outside clinic visits, methodological limitations in the evidence base require further well-planned and quality research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Major advances in different cancer treatment modalities have been made, and people are now living longer with cancer [1, 2]. However, cancer patients experience a range of symptoms or side effects during cancer treatment [3,4,5] that can impair daily functioning and lead to physical and/or psychological distress and worse health-related quality of life (HRQOL) [4, 6, 7]. While systemic chemotherapy is a highly effective treatment for cancer [8, 9], its administration may place patients at risk for potentially serious adverse treatment toxicities (TT) if these are not recognized early and managed effectively [3].
Ultimately, it is cancer patients who take responsibility for managing treatment side effects and TT outside of clinic visits with minimal supervision [10] and report poor quality of self-management support to do this effectively [11]. Also, poor quality of symptom management by clinicians is identified [12]. This leaves patients vulnerable to getting even sicker and may explain the high rates of cancer symptom distress [13], emergency room (ER) visits and hospitalization (ER + H) for patients receiving chemotherapy [14,15,16]. Such rates are costly to the health system [17] and concerning as poor symptom control is associated with higher morbidity, treatment non-adherence, and worse survival [18, 19].
Internet technology is proposed as a solution to provide better symptom monitoring and earlier intervention for TT [20, 21]. In this review, Internet technology refers to all web-enabled interventions or platforms and mobile devices such as smartphones. There is empirical evidence that substantiates the role of Internet-based interventions in the delivery of supportive care to people living with the complexities of chronic health conditions [22,23,24,25]. However, the effectiveness of Internet-based interventions specifically designed for managing chemotherapy-related symptoms or TT on symptom distress and/or quality of life (QoL) is less clear [26, 27]. Moreover, information on the design elements and features of these interventions and how they were planned and carried out and who benefited from these approaches is still required [28].
This systematic literature review was conducted to address this gap in empirical knowledge and aimed (1) to examine the effectiveness of Internet-based interventions on cancer chemotherapy-related physical (severity and/or distress) symptoms and HRQOL outcomes and (2) to identify the essential design elements and processes for implementing these interventions in oncology practices.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting the review [29]. We used the P.I.C.O.S. (Population, Interventions, Comparators, Outcomes, and Study Design) framework to identify relevant studies. Our focus was on adult (> 18 years) cancer patients receiving chemotherapy (P), interventions that were delivered via the Internet (I) compared with usual care or other active intervention (C-Comparison) on chemotherapy-related physical symptom severity or distress and/or HRQOL (O-Outcomes).
Search strategy
We searched databases recommended by Cochrane [30]. The search strategy was developed, in consultation with an information specialist, initially for Medline (PubMed), then adapted and applied to other databases used in this review including PsycINFO, CINAHL, Cochrane Database of Systematic Reviews, and Cochrane Central Registrar of Controlled Trials to identify studies. To retrieve other relevant publications, the reference lists of selected publications were hand searched. The main search strategy key terms included “cancer,” “self-management,” “Internet,” and “chemotherapy.” Each term included medical subject headings (MeSH) and search keywords using truncation (*) within title or abstract fields. Boolean terms “OR” and “AND” were used to combine searches within and between the key terms, respectively. The search was limited to all papers published in English from January 2000 to October 2016. The reasons for limiting the literature search from 2000 onwards were based on the initial date of publications testing the use of the Internet-based support programs in the delivery of supportive care within the past 15 years [28, 31].
Study selection
Based on the pre-determined study eligibility criteria, two authors (SM, NV) independently selected all studies retrieved from the databases. Any discrepancies between reviewers were resolved through discussion and/or the involvement of a third reviewer (DH), if necessary.
Eligibility criteria
All interventional studies including randomized or non-randomized controlled trials and pre/post or quasi-experimental intervention studies with a comparison group were considered. The primary outcomes of interest were chemotherapy-related physical symptom severity or distress and/or HRQOL. Only studies published in English were included. We excluded studies that only reported on the development or the usability and/or acceptability of interventions. We excluded studies that did not describe a sample size calculation (with power calculation), as a study with low statistical power has a reduced chance of detecting a true effect [32].
Quality assessment
A methodological quality assessment of studies was conducted following a checklist that was an adapted version of the Cochrane Collaboration Back Review Group [33] and was used previously in other systematic reviews of Internet-based interventions [31, 34]. The authors modified the Cochrane list to better suit the type of studies examined. For instance, one of the main components of Internet-based interventions that is highly valued and appeals to different patient populations is the ability to engage in direct or interactive communication with a clinician [35]. This precludes “blinding” of patients and clinicians. Also, “description of adverse events” may not be relevant to these interventions. To date, there are no studies indicating the occurrence of any adverse events resulting from use of these interventions in cancer care [36].
The final list of criteria can be found in Table 3 and includes the methodological quality assessment of studies in this review. The quality score could range from 0 to 13 points. For each study, all criteria were scored with yes, no, or unclear, resulting in a maximum quality score of 13. In line with other researchers [31, 34, 37], we considered studies obtaining at least two thirds of the total score (i.e., ≥ 8 points) to be of high quality. Studies scoring 4 to 7 points were rated as moderate quality, and studies scoring lower than 4 points were rated as low quality.
Results
Studies identified
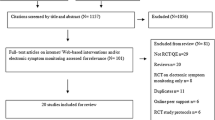
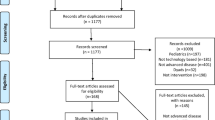
The PRISMA flow chart of the selection process is shown in Fig. 1. Of the initial 1766 titles identified, the following search results were obtained: Medline (n = 631), EMBASE (n = 1005), CINAHL (n = 98), Cochrane Central Registrar of Controlled Trials (n = 23), Cochrane Database of Systematic Reviews (n = 7), and PsychINFO (n = 2). Based on titles and abstracts, 56 publications were identified as potentially eligible. After reviewing the articles, only six publications met all the eligibility criteria. The main reasons for ineligibility were the study only measured patient satisfaction and not a symptom outcome; no comparison group to evaluate the intervention’s effectiveness; only examined the usability and/or acceptability of these interventions, not having a relevant outcome measure; and did not describe sample size calculation or not statistically powered (small sample size) to detect any true effects.

PRISMA flow diagram illustrating the systematic review process from electronic searching through to study inclusion
Study characteristics
Characteristics of the included studies are summarized in Tables 1 and 2. All studies were published in 2013 or later, with one exception of a study that was published in 2009 [41]. Four studies were conducted in Europe (Norway [n = 2], Finland [n = 1], and UK [n = 1]) and two in the USA. All studies were RCTs and sample sizes ranged from 90 to 766 participants. Two studies [40, 42] were focused on breast cancer patients. Four other studies were conducted in patients with various cancer types of which breast cancer patients constituted 18.7–62.5%. Only one trial [42] had three arms, and all other studies were two-arm studies with parallel assignment of patients to one of two groups. In four studies [38, 40,41,42], the control comparator was usual care while in two other studies [39, 43], the control comparator was educational support. Intervention and/or follow-up periods varied and ranged from one chemotherapy cycle to 12 months.
Effectiveness of the interventions in managing chemotherapy-related symptoms
Effectiveness of the interventions was evaluated by assessing the results of the studies on a priori outcomes of interest inclusive of chemotherapy-related physical symptoms and/or HRQOL-related outcomes. A number of other outcomes were identified for included studies such as psychological symptoms and frequency of ER visits, which are also abstracted and summarized in Table 2. Five studies measured symptom distress [39,40,41,42,43] with reduction in severity of symptoms and/or symptom distress reported in four of these studies [39, 41,42,43], whereas one study did not report any differences in presence and/or change in severity of symptom distress [40]. Of the three studies that measured HRQOL [38,39,40], two reported improvement (or no deterioration over time) for the intervention group [38, 39]. Three studies measured depression and/or anxiety [39, 40, 42] and two of them found a significant positive effect (reduced anxiety and/or depression) in favor of the intervention group [39, 42]. Only one study [38] reported patients receiving the intervention were less frequently admitted to the ER or hospitalized. Only one study [38] reported the effect size (a moderate effect size of 0.38).
Quality assessment
Table 3 shows the quality assessment criteria indicating that all the studies obtained a score of 8 or higher, representing moderately high methodological quality. All the studies specified participant eligibility criteria, clearly described the method of randomization and groups’ similarity at baseline, and employed a comparable timing of outcome assessment for the different groups. Also, all studies performed a power calculation and used an intention-to-treat approach for the data analysis. However, most studies did not clearly report the methods for concealing treatment allocation (i.e., sealed envelope) or any blinding.
Intervention designs and features
Table 2 shows the main design features of the interventions, and the functionalities of the interface or platform and outcome measures. Five studies [38, 39, 41,42,43] were focused on the remote monitoring of chemotherapy-related toxicity using patient-reported outcomes (PROs). In these studies, patients had the opportunity to communicate with clinicians. In two of these studies [39, 41], patients received tailored self-care advice and also could monitor their symptoms via a graph of symptoms over time. One study [40] focused on breast cancer patients’ empowerment used a patient education program to guide patients on how to manage side effects before therapy started.
Basch [38] applied a web-based interface design (STAR), which included questions adapted for PRO reporting from the National Cancer Institute’s Common Terminology Criteria for Adverse Events (PRO-CTCAE) [44, 45]. Tablet computers were used by patients for the reporting of 12 common symptoms (see Table 1) experienced during chemotherapy on a daily basis [46]. STAR triggered e-mail alerts to nurses whenever a patient-reported symptom worsened by ≥ 2 points or reached an absolute grade ≥ 3. STAR also sent e-mail reminders to participants weekly and/or informed participants if e-mails were not monitored (after business hours) and encouraged them to call the office at such times for symptoms of concern. No specific guidance was provided to clinicians about what actions to take in response to alerts. Change in HRQOL at 6 months compared with baseline was the primary outcome and declined by less in the intervention arm compared with usual care (see Table 2).
Ruland [39] examined an interactive health communication application (WebChoice) that allowed cancer patients to monitor their symptoms over time, provided them with individually tailored self-care advice and e-coaching to support them to manage their symptoms. The application contained self-management options, possibilities for e-communication with nurses, and an e-forum for group discussion with other cancer patients. Statistically significant differences between groups were shown for the Global Distress Index (see Table 2).
Ryhanen [40] tested a tailored patient educational program for breast cancer patients to increase the patient’s knowledge to better manage their treatment-related side effects. Outcomes of QoL, anxiety, and patient management of chemotherapy and radiotherapy-related side effects were measured. The researchers assessed 14 side effects of chemotherapy with instruments designed specifically by the investigators for the study. There were no significant differences in the QoL, anxiety, or side effects of treatment between the groups (see Table 2).
Kearney [41] employed a phone-based mobile device to monitor and support patient and clinician management of six chemotherapy-related symptoms (see Table 2). Patients were asked to complete an e-symptom questionnaire based on a PRO-CTCAE [46, 47]. After completing the questionnaire, patients immediately received written feedback on the mobile phone interface. An evidence-based risk assessment algorithm was integrated into the ASyMS© server software. This system alerted clinicians via a dedicated 24-h pager system of clinically important symptoms and advised the clinician to contact patients by telephone within a set time period. Study clinicians could access secure web pages to view the patients’ symptom reports to guide clinical decision-making and advice given to the patient.
Borosund [42] Internet intervention included an assessment component, tailored symptom self-management support, and interactive communication. Three arms were used to compare the effects of (1) an Internet-based patient-provider communication service (IPPC), compared with (2) the WebChoice intervention (including an IPPC), and (3) usual care on symptom distress, anxiety, depression, and self-efficacy after 6 months of follow-up. Twenty care providers (11 nurses, 6 physicians, and 3 social workers) were trained for online communication with patients. Patients in the IPPC group could ask questions, share experiences with, or get advice from clinicians. Patients in the WebChoice group, in addition to the IPPC service, could report occurrence and burden of symptoms and indicate if they needed help. IPPC alone significantly reduced depression compared with the usual care group. The multicomponent intervention WebChoice had additional positive effects on reductions in symptom distress, anxiety, and depression compared with the usual care group (see Table 2).
Berry [43] evaluated the effect of a self-report assessment and educational intervention on symptom distress during cancer therapy. Patients were asked to report severity of common symptoms and side effects of therapy at any time and received tailored self-care instruction that included on-screen, tailored coaching, and encouraged to describe the severity, pattern, and alleviating/aggravating factors related to their symptoms. The results indicated significantly lower symptom distress over the course of therapy in the intervention group (see Table 2), particularly among younger age participants (> 50 years) (P = .002).
Discussion
Principal findings
Despite the potential advantages of Internet technology, there are few rigorous prospectively designed studies of Internet-based interventions that target management of cancer chemotherapy-related symptom and TT. The low number of Internet-based intervention studies was a surprising finding of this review given the increasing use of the Internet by cancer patients for information and supportive care [48, 49]. However, a number of Internet-based interventions were in the development phase and primarily examined the usability, acceptability, and/or feasibility of these interventions and not efficacy.
The main design features of the Internet platforms identified in the studies reviewed included PRO reporting of symptoms, telephone counseling by clinicians in response to the PRO data, and e-messaging or interactive communication. However, several methodological issues were identified that may have influenced intervention effectiveness. These included differences in the components, design features, and functionalities of the Internet interventions, lack of standardization in PRO measures used across studies, and little attention paid to implementation or integration into oncology practices, i.e., clinician response to alerts or to patient adherence to the intervention and warrant further discussion below.
Design features and content of the interventions
Internet-based interventions may contribute to symptom improvement through capturing and monitoring symptom severity data, providing tailored information, and prompting clinicians to manage cancer patients’ symptoms remotely, among several other mechanisms [50]. Since these interventions are considered complex interventions, difficulty may arise in determining, which of the many features, functionalities, and interacting components of these interventions contribute to effectiveness [51, 52]. It was not clear which components of these interventions were most beneficial or used by either patients or how the alerts were implemented in clinical practice. Most of the studies provided a limited description of their study design features used to deliver the intervention. Only Borosund tracked and reported usage of different components of their intervention among patients [42].
One of the advantages of the Internet is its ability to provide interactive and tailored content to patients [53]. However, the essential factors that may contribute to effectiveness of Internet-based interventions need to be identified. Effectiveness may be improved by enhancing the design features of the interventions [54]. The core considerations when designing effective supportive care interventions are (1) to identify the influences of specific design features on effectiveness of the intervention and outcomes and (2) how each design feature is implemented [54, 55].
One of the main components of included interventions was self-reporting and capturing of PROs for symptoms related to cancer treatment. Basch [38] found that patients in intervention group experienced improved HRQOL compared with the usual care group. Also, four other studies [39, 41,42,43] reported patients in their intervention groups experienced less symptom distress. However, they did not clearly report how clinicians acted upon receiving PRO information or followed up on alerts or the level of adherence of clinicians in responding to these alerts.
Certain important domains for evaluating efficacy of interventions in cancer supportive care rely predominantly on patient-articulated feelings and experiences and thus depend on reliable and valid PRO measures [56]. The interpretation of effectiveness in these studies should be viewed with caution given that researchers developed their own outcome measures potentially leading to erroneous conclusions about statistical significance [28]. Using uniform valid PRO (rather than purpose-designed questionnaires) increases study credibility and generalizability and facilitates meta-analyses [31, 57].
Another common component offered in the Internet platform used in some studies was e-communication between patients and providers and was rated by patients as the most valuable component of the WebChoice intervention [58]. Patient-provider e-communication has been reported as useful in several other studies in terms of supporting patients in managing illness and enhancing health outcomes [59, 60], and enhancing QoL [59, 61]. However, rarely reported in the included studies was how this component was operationalized and strategies used for integration in work flow, routine care processes, and if any training was provided to clinicians. Only one study [42] reported how clinicians answered patients’ e-messages. However, the time spent on answering messages by clinicians was not measured to inform future implementation.
Implementation processes
Although, Internet-based interventions allow participants to access intervention content at their convenience and can be structured to provide tailored messages [62], implementation of these initiatives has often been problematic, with many failing to demonstrate predicted benefits [63]. Similarly, variability in effectiveness was also found in our review. Moreover, most studies mainly focused on outcomes and effectiveness and only one study [39] in another manuscript [64] reported on the factors relevant for successful implementation of their intervention in clinical practice. May et al. [65] suggest more attention needs to be paid to the implementation of technologies in oncology practices and specifically the “workability” of the intervention in practices or in the daily life of patients [66, 67]. The uptake of Internet-based interventions in routine management of symptoms requires determining from both the patients’ and clinicians’ perspective the workability of the intervention in care.
Clinicians’ readiness
Despite the growing evidence that Internet-based support programs have great potential to improve care, some studies report low adoption and acceptance rates of using such interventions among clinicians [68, 69]. Borosund et al. [42] reported that the number of e-messages in their study was moderate and manageable by nurses during regular working hours. However, they mentioned a need to obtain a deeper understanding of clinicians’ experience with the use of IPPC in routine care to guide future implementation processes. Clinicians express concerns that e-messages might disrupt existing workflows and increase workloads [70]. Previous research that has examined workability of such interventions in clinical care mostly focused on the “ease of use” of the new systems for clinicians, with the underlying assumption that clinicians would be deterred from or resistant to using systems that added complexity or required additional effort or time [71]. Implementation failure has been attributed to slow clinician behavior change and time constraints [72, 73]. To overcome some of these difficulties, the Medical Research Council (MRC) [45] recommends use of a phased approach to intervention design and engagement of end users in intervention development.
If clinicians recognize Internet-based interventions as effective and as facilitating their abilities to better manage symptoms and for providing standardized self-management support, they might be more receptive to these types of interventions [74]. However, cancer system resources are not yet aligned to receive “real-time” PRO symptom data except during scheduled ambulatory cancer clinic visits [42]. It is also not yet clear if patients are willing to use these devices on a daily basis to manage cancer treatment symptoms possibly leading to high study attrition [35].
Patients’ attrition
In all included studies, the observed level of attrition was more than anticipated. High attrition rates (up to 46%) were noted, which is common for Internet interventions [75]. One reason for high attrition rates in such interventions might be having an implicit pro-innovation bias on the part of the research, i.e., not expecting that an innovation will be rejected [76]. The characteristics of such interventions may influence attrition including (1) relative advantage, whether the innovation is perceived as superior to current practice, (2) compatibility with clinicians practice and if the technology is consistent with the patients’ values and their past experiences, (3) complexity (i.e., being difficult to understand and use), and (4) observability, the results are visible to others, i.e., they reduce symptom distress [77].
Patients’ adherence
Ruland et al. [39] reported that 23% of the participants in the experimental group never logged onto the interactive communication component of their intervention (WebChoice) and only 64% logged on more than once. Poor adherence to Internet-based interventions is common and has been reported in many other studies [78,79,80]. Inadequate adherence to the intervention may influence underestimation of intervention effects and account for the inconclusive findings. Adherence to symptom management is influenced by several factors, such as perceptions of relevance, convenience, and beliefs about the intervention [68]. In Borosund’s study, the main reasons for declining to participate were lack of experience with the Internet and patients reported that they had too much on their mind related to their illness. Patients do not have a strong preference for using techniques and methods that are not relevant to them [68, 69]. Moreover, patients are more likely to adhere to methods, techniques, and interventions that are simple and fit easily into their daily routines [70]. Thus, Internet interventions may not be entirely appropriate for all cancer populations, if they are perceived as difficult to use or a poor fit with the patients’ daily lives. Identifying specific patient characteristics and factors that may influence the use of interventions is crucial [81, 82]. Borosund [35] explored how patients’ demographic, disease-related, and psychosocial factors were associated with the use of different components of the WebChoice. They reported e-messages and self-care advice were the components most frequently used by patients with low levels of social support and high levels of symptom distress and depression. However, it could be that there are patient groups in whom it would be inappropriate to attempt to utilize e-technology in empowering them to manage their cancer treatment-related symptoms, an issue that the current evidence does not go far enough towards identifying or addressing. Nevertheless, knowing what patients are most likely to use Internet-based interventions but also who benefit is imperative to understanding effectiveness in future research [48].
Overall, while effectiveness was shown for some of the studies included in this review, heterogeneity in intervention design, features of the Internet platform, and in the outcomes measured makes it difficult to draw a firm conclusion regarding the effectiveness of the interventions for improving chemotherapy symptom management. Future trials require greater attention to implementation issues and employment of recommended strategies to minimize attrition and improve adherence, which may improve effectiveness on symptom outcomes.
Limitation
Given that health IT literature is relatively new and quite diverse, the current study focused exclusively on Internet-based interventions for supporting patients in managing chemotherapy-related symptoms. Despite this limitation, the current paper highlights the importance of continued study of this intervention method. Another limitation is that our literature search only includes articles in English; therefore, it is possible that some studies conducted in other parts of the world in other languages were missed.
Conclusion
Despite the evidence in support of using the Internet as a worthwhile tool in management of cancer TT outside of clinic visits, further research is required before these interventions can reach their full potential. The use of an appropriate theoretical framework (e.g., MRC) may help to guide future interventions and their uptake in routine clinical care and in the daily lives of patients.
References
Cella D, Fallowfield LJ (2008) Recognition and management of treatment-related side effects for breast cancer patients receiving adjuvant endocrine therapy. Breast Cancer Res Treat 107(2):167–180. https://doi.org/10.1007/s10549-007-9548-1
Bloechl-Daum B, Deuson RR, Mavros P et al (2006) Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol 24(27):4472–4478. https://doi.org/10.1200/jco.2006.05.6382
Rajapakse D (2010) Symptom management during chemotherapy. Paediatr Child Health 20(3):129–134. https://doi.org/10.1016/j.paed.2009.10.005
Breen SJ, Baravelli CM, Schofield PE et al (2009) Is symptom burden a predictor of anxiety and depression in patients with cancer about to commence chemotherapy? Med J Aust 190(7 Suppl):S99–104
Van Leeuwen FE, Ng AK (2016) Long-term risk of second malignancy and cardiovascular disease after Hodgkin lymphoma treatment. Hematology Am Soc Hematol Educ Program 1:323–330
Cleeland CS, Mendoza TR, Wang XS et al (2000) Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer 89(7):1634–1646
Stark L, Tofthagen L, Visovsky C et al (2012) The symptom experience of patients with cancer. J Hosp Palliat Nurs 14(1):61–70. https://doi.org/10.1097/NJH.0b013e318236de5c
Frei E (1985) Curative cancer chemotherapy. Cancer Res 45:6523–6537
Peterson DE, Lalla R (2010) Overview of complications of systemic chemotherapy. In Oral Complications of Cancer and its Management. Oxford University Press, Oxford
McCorkle R, Ercolano E, Lazenby M et al (2011) Self-management: enabling and empowering patients living with cancer as a chronic illness. CA Cancer J Clin 61(1):50–62
Kossert A, Howell D, Friedman A et al (2013) Characterization of symptom and disease self-management in Canadian Cancer Care: illness representations of sentinel disease sites. Ann Behav Med 45(2):S10 A028
Howell D, Liu G (2011) Can routine collection of patient reported outcome data actually improve person-centered health? Healthc Pap 11(4):42–47 discussion 55-48
Bultz BD, Holland JC (2006) Emotional distress in patients with cancer: the sixth vital sign. Commun Oncol 3(5):311–314
Enright K, Grunfeld E, Yun L et al (2015) Population-based assessment of emergency room visits and hospitalizations among women receiving adjuvant chemotherapy for early breast cancer. J Oncol Pract 11(2):126–132. https://doi.org/10.1200/JOP.2014.001073
Hassett MJ, O’Malley AJ, Pakes JR et al (2006) Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J Natl Cancer Inst 98(16):1108–1117
Vandyk AD, Harrison MB, Macartney G et al (2012) Emergency department visits for symptoms experienced by oncology patients: a systematic review. Support Care Cancer 20(8):1589–1599
Matthew-Maich N, Harris L, Ploeg J et al (2016) Designing, implementing, and evaluating mobile health technologies for managing chronic conditions in older adults: a scoping review. JMIR mHealth uHealth 4(2):e29
Trajkovic-Vidakovice M, de Graeff A, Voest EE (2012) Symptoms tell it all: a systematic review of the value of symptom assessment to predict survival in advanced cancer patients. Crit Rev Oncol Hematol 84:130–148
Puts MTE, Tu HA, Tourangeau A et al (2013) Factors influencing adherence to cancer treatment in older adults with cancer: a systematic review. Ann Oncol:1–14
Stone AA, Broderick JE (2007) Real-time data collection for pain: appraisal and current status. Pain Med 8(Suppl 3):S85–S93. https://doi.org/10.1111/j.1526-4637.2007.00372.x
Bender JL, Radhakrishnan A, Diorio C et al (2011) Can pain be managed through the Internet? A systematic review of randomized controlled trials. Pain 152(8):1740–1750. https://doi.org/10.1016/j.pain.2011.02.012
Chumbler NR, Neugaard B, Kobb R et al (2005) Evaluation of a care coordination/home-telehealth program for veterans with diabetes: health services utilization and health-related quality of life. Eval Health Prof 28(4):464–478. https://doi.org/10.1177/0163278705281079
Louis AA, Turner T, Gretton M et al (2003) A systematic review of telemonitoring for the management of heart failure. Eur J Heart Fail 5(5):583–590
Rasmussen LM, Phanareth K, Nolte H et al (2005) Internet-based monitoring of asthma: a long-term, randomized clinical study of 300 asthmatic subjects. J Allergy Clin Immunol 115(6):1137–1142. https://doi.org/10.1016/j.jaci.2005.03.030
Barnett TE, Chumbler NR, Vogel WB et al (2006) The effectiveness of a care coordination home telehealth program for veterans with diabetes mellitus: a 2-year follow-up. Am J Manag Care 12(8):467–474
Agboola SO, Ju W, Elfiky A et al (2015) The effect of technology-based interventions on pain, depression, and quality of life in patients with cancer: a systematic review of randomized controlled trials. J Med Internet Res 17(3):e65. https://doi.org/10.2196/jmir.4009
Dickinson R, Hall S, Sinclair JE et al (2014) Using technology to deliver cancer follow-up: a systematic review. BMC Cancer 14:311. https://doi.org/10.1186/1471-2407-14-311
Ventura F, Ohlen J, Koinberg I (2013) An integrative review of supportive e-health programs in cancer care. Eur J Oncol Nurs 17(4):498–507. https://doi.org/10.1016/j.ejon.2012.10.007
Moher D, Shamseer L, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4(1):1. https://doi.org/10.1186/2046-4053-4-1
Furlan AD, Pennick V, Bombardier C et al (2009) 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine 34(18):1929–1941. https://doi.org/10.1097/BRS.0b013e3181b1c99f
Kuijpers W, Groen WG, Aaronson NK et al (2013) A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: relevance for cancer survivors. J Med Internet Res 15(2):e37. https://doi.org/10.2196/jmir.2281
Button KS, Ioannidis JPA, Mokrysz C et al (2013) Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci 14(5):365–376. https://doi.org/10.1038/nrn3475
Dy SM, Roy J, Ott GE et al (2011) Tell Us: a web-based tool for improving communication among patients, families, and providers in hospice and palliative care through systematic data specification, collection, and use. J Pain Symptom Manag 42(4):526–534. https://doi.org/10.1016/j.jpainsymman.2010.12.006
Bouma G, Admiraal JM, de Vries EG et al (2015) Internet-based support programs to alleviate psychosocial and physical symptoms in cancer patients: a literature analysis. Crit Rev Oncol Hematol 95(1):26–37. https://doi.org/10.1016/j.critrevonc.2015.01.011
Børøsund E, Cvancarova M, Ekstedt M et al (2013) How user characteristics affect use patterns in web-based illness management support for patients with breast and prostate cancer. J Med Internet Res 15(3):e34. https://doi.org/10.2196/jmir.2285
Cox A, Lucas G, Marcu A et al (2017) Cancer survivors’ experience with telehealth: a systematic review and thematic synthesis. J Med Internet Res 19(1):e11. https://doi.org/10.2196/jmir.6575
van den Berg MH, Schoones JW, Vliet Vlieland TP (2007) Internet-based physical activity interventions: a systematic review of the literature. J Med Internet Res 9(3):e26. https://doi.org/10.2196/jmir.9.3.e26
Basch E, Deal A, Kris M et al (2016) Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol 34(6):557–565
Ruland CM, Andersen T, Jeneson A et al (2013) Effects of an internet support system to assist cancer patients in reducing symptom distress: a randomized controlled trial. Cancer Nurs 36(1):6–17. https://doi.org/10.1097/NCC.0b013e31824d90d4
Ryhanen AM, Rankinen S, Siekkinen M et al (2013) The impact of an empowering Internet-based Breast Cancer Patient Pathway program on breast cancer patients’ clinical outcomes: a randomised controlled trial. J Clin Nurs 22(7–8):1016–1025. https://doi.org/10.1111/jocn.12007
Kearney N, McCann L, Norrie J et al (2009) Evaluation of a mobile phone-based, advanced symptom management system (ASyMS) in the management of chemotherapy-related toxicity. Support Care Cancer 17(4):437–444. https://doi.org/10.1007/s00520-008-0515-0
Borosund E, Cvancarova M, Moore SM et al (2014) Comparing effects in regular practice of e-communication and web-based self-management support among breast cancer patients: preliminary results from a randomized controlled trial. J Med Internet Res 16(12):e295. https://doi.org/10.2196/jmir.3348
Berry DL, Hong F, Halpenny B et al (2014) Electronic self-report assessment for cancer and self-care support: results of a multicenter randomized trial. J Clin Oncol 32(3):199–205. https://doi.org/10.1200/jco.2013.48.6662
Basch E, Iasonos A, Barz A et al (2007) Long-term toxicity monitoring via electronic patient-reported outcomes in patients receiving chemotherapy. J Clin Oncol 25(34):5374–5380
Medical Research Council (2000) A framework for the development and evaluation of RCTs for complex interventions to improve health. Medical Research Council, London
National Cancer Institute, National Institutes of Health, U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. NIH publication # 09-7473. Published May 29, 2009; Revised Version 4.02 September 15, 2009. Available at http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf. Accessed 15 Sept 2017
Brown V, Sitzia J, Richardson A et al (2001) The development of the Chemotherapy Symptom Assessment Scale (C-SAS): a scale for the routine clinical assessment of the symptom experiences of patients receiving cytotoxic chemotherapy. Int J Nurs Stud 38(5):497–510
Eysenbach G (2003) The impact of the Internet on cancer outcomes. CA Cancer J Clin 53(6):356–371
Ryhanen AM, Siekkinen M, Rankinen S et al (2010) The effects of Internet or interactive computer-based patient education in the field of breast cancer: a systematic literature review. Patient Educ Couns 79(1):5–13. https://doi.org/10.1016/j.pec.2009.08.005
McLean S, Chandler D, Nurmatov U et al (2010) Telehealthcare for asthma. Cochrane Database Syst Rev 10. https://doi.org/10.1002/14651858.CD007717.pub2
Ekeland AG, Bowes A, Flottorp S (2010) Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform 79(11):736–771. https://doi.org/10.1016/j.ijmedinf.2010.08.006
Elbert NJ, van Os-Medendorp H, van Renselaar W et al (2014) Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: a systematic review of systematic reviews and meta-analyses. J Med Internet Res 16(4):e110. https://doi.org/10.2196/jmir.2790
Ritterband LM, Thorndike FP, Cox DJ et al (2009) A behavior change model for internet interventions. Ann Behav Med 38(1):18–27. https://doi.org/10.1007/s12160-009-9133-4
Morrison LG, Yardley L, Powell J et al (2012) What design features are used in effective e-health interventions? A review using techniques from critical interpretive synthesis. Telemed e-Health 18(2):137–144. https://doi.org/10.1089/tmj.2011.0062
Schofield P, Chambers S (2015) Effective, clinically feasible and sustainable: key design features of psycho-educational and supportive care interventions to promote individualised self-management in cancer care. Acta Oncol 54(5):805–812. https://doi.org/10.3109/0284186X.2015.1010016
Garcia SF, Cella D, Clauser SB et al (2007) Standardizing patient-reported outcomes assessment in cancer clinical trials: a patient-reported outcomes measurement information system initiative. J Clin Oncol 25(32):5106–5112. https://doi.org/10.1200/JCO.2007.12.2341
McAllister M, Dunn G, Payne K et al (2012) Patient empowerment: the need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res 12:157. https://doi.org/10.1186/1472-6963-12-157
Ruland CM, Maffei RM, Børøsund E et al (2013) Evaluation of different features of an eHealth application for personalized illness management support: cancer patients’ use and appraisal of usefulness. Int J Med Inform 82(7):593–603. https://doi.org/10.1016/j.ijmedinf.2013.02.007
Zhou YY, Kanter MH, Wang JJ et al (2010) Improved quality at Kaiser Permanente through email between physicians and patients. Health Aff (Millwood) 29(7):1370–1375. https://doi.org/10.1377/hlthaff.2010.0048
Goldzweig LC, Shekelle PG, Towfigh AA et al (2012) Systematic review: secure messaging between providers and patients, and patients’ access to their own medical record. Evid Based Synth Prog 39(1)
McGeady D, Kujala J, Ilvonen K (2008) The impact of patient-physician web messaging on healthcare service provision. Int J Med Inform 77(1):17–23. https://doi.org/10.1016/j.ijmedinf.2006.11.004
Strecher V (2007) Internet methods for delivering behavioral and health-related interventions (eHealth). Annu Rev Clin Psychol 3:53–76. https://doi.org/10.1146/annurev.clinpsy.3.022806.091428
Murray E, Burns J, May C et al (2011) Why is it difficult to implement e-health initiatives? A qualitative study. Implement Sci 6:6. https://doi.org/10.1186/1748-5908-6-6
Varsi C, Ekstedt M, Gammon D et al (2015) Using the consolidated framework for implementation research to identify barriers and facilitators for the implementation of an internet-based patient-provider communication service in five settings: a qualitative study. J Med Internet Res 17(11):e262. https://doi.org/10.2196/jmir.5091
May C, Sibley A, Hunt K (2014) The nursing work of hospital-based clinical practice guideline implementation: an explanatory systematic review using normalisation process theory. Int J Nurs Studs 51(2):289–299. https://doi.org/10.1016/j.ijnurstu.2013.06.019
Gallacher K, May CR, Montori VM et al (2011) Understanding patients’ experiences of treatment burden in chronic heart failure using normalization process theory. Ann Fam Med 9(3):235–243. https://doi.org/10.1370/afm.1249
May C, Finch T (2009) Implementing, embedding, and integrating practices: an outline of normalization process theory. Sociology 43(3):535–554. https://doi.org/10.1177/0038038509103208
Li J, Land L, Ray P (2008) Humanitarian Technology Challenge (HTC)-electronic health records perspective. A Report of Joint Project of IEEE and United Nations Foundation In
Li J, Talaei-Khoei A, Seale H et al (2013) Health care provider adoption of eHealth: systematic literature review. Interact J Med Res 2(1):e7
Nijland N, van Gemert-Pijnen J, Boer H et al (2008) Evaluation of internet-based technology for supporting self-care: problems encountered by patients and caregivers when using self-care applications. J Med Internet Res 10(2):e13. https://doi.org/10.2196/jmir.957
Mair FS, May C, O’Donnell C et al (2012) Factors that promote or inhibit the implementation of e-health systems: an explanatory systematic review. Bull World Health Organ 90:357–364. https://doi.org/10.2471/BLT.11.099424
Asua J, Orruño E, Reviriego E et al (2012) Healthcare professional acceptance of telemonitoring for chronic care patients in primary care. BMC Med Informat Decis Mak 12(1):139. https://doi.org/10.1186/1472-6947-12-139
Lin C, Lin IC, Roan J (2012) Barriers to physicians’ adoption of healthcare information technology: an empirical study on multiple hospitals. J Med Syst 36(3):1965–1977. https://doi.org/10.1007/s10916-011-9656-7
Curry SJ (2012) eHealth research and healthcare delivery. Am J Prev Med 32(5):S127–S130. https://doi.org/10.1016/j.amepre.2007.01.026
Bennett G, Glasgow R (2009) The delivery of public health interventions via the Internet: actualizing their potential. Annu Rev Public Health 30:273–292. https://doi.org/10.1146/annurev.publhealth.031308.100235
Rogers E (2003) Diffusion of innovations. Free Press, New York
Eysenbach G (2005) The law of attrition. J Med Internet Res 1(e11). https://doi.org/10.2196/jmir.7.1.e11
Gustafson DH, Hawkins RP, Boberg EW et al (2002) CHESS: 10 years of research and development in consumer health informatics for broad populations, including the underserved. Int J Med Inform 65(3):169–177
Murray E, Burns J, See TS et al (2005) Interactive health communication applications for people with chronic disease. Cochrane Database Syst Rev 4:CD004274. https://doi.org/10.1002/14651858.CD004274.pub4
Ruland CM, Holte HH, Roislien J et al (2010) Effects of a computer-supported interactive tailored patient assessment tool on patient care, symptom distress, and patients’ need for symptom management support: a randomized clinical trial. J Am Med Inform Assoc 17(4):403–410. https://doi.org/10.1136/jamia.2010.005660
Eysenbach G (2005) The law of attrition. J Med Internet Res 7(1):e11. https://doi.org/10.2196/jmir.7.1.e11
Williamson K (2005) Where one size does not fit all: understanding the needs of potential users of a portal to breast cancer knowledge online. J Health Commun 10(6):567–580. https://doi.org/10.1080/10810730500228961
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
We have full control of all primary data and agree to allow the journal to review our data if requested.
Rights and permissions
About this article

Cite this article
Moradian, S., Voelker, N., Brown, C. et al. Effectiveness of Internet-based interventions in managing chemotherapy-related symptoms in patients with cancer: a systematic literature review. Support Care Cancer 26, 361–374 (2018). https://doi.org/10.1007/s00520-017-3900-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-017-3900-8