
Abstract
Purpose
Insomnia is highly prevalent in people who are affected by cancer. However, options available to receive support for insomnia are limited. Telephone-based help services, such as cancer helplines, may be ideally placed to meet unmet needs regarding insomnia after cancer. The present study describes the prevalence and predictors of insomnia in patients and caregivers who call cancer helplines seeking support.
Methods
Participants (N = 500 patients, N = 234 caregivers) were recruited through an Australian state-based telephone-delivered cancer helpline. In addition to routine screening with the Distress Thermometer, participants were administered the Insomnia Severity Index.
Results
Most participants were female, older than 50 years of age, and were three (caregivers) to four (patients) months post-diagnosis. Insomnia symptoms were reported by 59.4 % of patients and 62.9 % of caregivers, with moderate to severe levels of insomnia reported by 27 % of patients and 30 % of caregivers. Insomnia was predicted by distress level for both patients (β = .31, p < .001) and caregivers (β = .32, p < .001) and age for patients only (β = −.13, p < .01).
Conclusions
Insomnia symptoms are common in patients and caregivers who call cancer helplines and appear to be related to distress. Telephone-based helplines have the potential to act as the first line of support in a stepped care approach addressing insomnia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A cancer diagnosis is a major life event negatively impacting not only the person diagnosed but also the people close to them. Cancer patients and caregivers can have a number of unmet needs that continue long after treatment has ended, influencing long-term cancer survivorship [3, 12, 13, 30]. Accessible information and self-management advice is crucial to helping individuals learn strategies to self-managed cancer-related problems [23]. The National Cancer Institute’s Cancer Information Service (CIS) was established to provide telephone-based access to cancer information, and this type of service has since extended to many other countries often supported by non-government cancer control agencies [6, 23]. In Australia these services are delivered through cancer helplines located in each state that provide a low-intensity but high-volume service providing brief informational support [11, 15], as well as psychosocial support and referral [8, 16, 17]. As such, telephone-based services, such as cancer helplines, may have the capacity to provide support for other problems that patients and caregivers face after a diagnosis of cancer.
One concern that has recently been shown to impact post-diagnosis adjustment for people affected by cancer is sleep disturbance and/or insomnia [4, 20, 27]. Insomnia is characterised by a cluster of symptoms including sleep onset latency, frequent waking, waking too early and deficits in daytime functioning due to lack of sleep [2, 19]. The prevalence of insomnia has been shown to range from 19 to 63 % for cancer patients [19, 27] and 40 to 50 % for caregivers [7, 20]. These rates of insomnia in cancer patients are two to three times higher than that found in the general population [28]. For cancer patients, the post-diagnosis experience is marked by a series of stressors that can act as a trigger for insomnia. In particular, the period after initial surgery soon after diagnosis is associated with high levels of insomnia [28]. However, insomnia can continue to be a significant issue long after cancer treatments have ceased [27]. Factors associated with sleep disturbance in cancer patients include hospitalisation, physical discomfort and pain, treatment side effects and immune system and physiological changes [19]. For example, patients reporting post-chemotherapy nausea and vomiting report a higher rate of insomnia [25], and anti-oestrogen treatments that aggravate menopausal symptoms can interfere with sleep [9]. Sleep disturbance is also associated with depression, anxiety and distress, with long-term negative impacts on quality of life [19]. Although studies investigating insomnia and sleep disturbances in caregivers of people diagnosed with cancer are scarce, the few studies that do exist suggest that moderate to severe sleep disturbance is highly prevalent and associated with a decreased quality of life [20]. Furthermore, the economic burden of untreated insomnia is high, with cost-effective treatments being considerably less costly than not treating this affliction [10].
In sum, insomnia is an important target for intervention with cancer patients and caregivers. Given cancer helplines have been shown to be an efficacious first point of contact in addressing cancer-related distress [17], a similar model may have a potential for identifying and treating insomnia in people affected by cancer. However, it is not yet known whether insomnia is a prevalent concern for the people who call cancer helplines. The primary aim of this study was to assess the prevalence of insomnia in patients and caregivers calling a cancer helpline, and the secondary aim to describe the predictors of insomnia.
Method
Participants and procedure
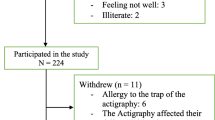
Ethical approval to conduct this study was obtained from the Human Research Ethics Committee at Griffith University (PSY/E2/12/HREC). Participants were recruited through the Cancer Council Queensland Cancer Helpline from 11th December 2012 to 26th March 2013. Eligible participants were callers to the cancer helpline who had been diagnosed with cancer or a caregiver of someone diagnosed with cancer and were at least 18 years of age. In total N = 500 patients and N = 234 caregivers agreed to participate from 1144 (43.71 %) patient and 809 (28.92 %) caregiver callers. Most patients and caregivers were female, older than 50 years of age, and had a high school education (Table 1). Median time since cancer diagnosis was 4 months for patients and 3 months for caregivers. Participant’s reason for calling the cancer helpline were predominantly practical issues (54.8 % of patients, 36.8 % of caregivers), psychological/emotional support (17.0 % of patients, 32.1 % of caregivers), treatment and management (14.8 % of patients, 14.1 % of caregivers) or general information (8.8 % of patients, 10.7 % of caregivers).
Materials
Information regarding demographics, cancer-related factors and distress levels are routinely collected during all calls to the cancer helpline, including, age, gender, cancer type, stage of diagnosis (patients only), months since diagnosis, reason for call and level of distress using the Distress Thermometer [24]. In addition, participants were administered the Insomnia Severity Index during the helpline call [21].
Distress
The single item Distress Thermometer (DT) [24] is routinely used in the cancer helpline in Queensland to screen callers’ levels of distress. Participants are asked to rate how much distress they have been experiencing in the past week including the current day using a scale of 0 to 10. Higher scores are indicative of greater distress, with the DT showing good sensitivity and specificity for detecting heightened psychological distress with a cut-off point of ≥4 [18].
Insomnia severity
The Insomnia Severity Index (ISI) is a seven-item measure of the nature, severity and impact of insomnia [2, 21, 29]. Participants are asked to consider the previous two weeks and rate their severity of 1) sleep onset, 2) sleep maintenance, 3) early morning awakening on a 5-point Likert scale (0 = not at all to 4 = very severe), 4) their level of sleep dissatisfaction on a 5-point Likert scale (0 = very satisfied to 4 = very dissatisfied), 5) the level of interference caused by sleep patterns on daily functioning, 6) noticeability of sleep problems by others and 7) distress caused by sleep patterns on a 5-point Likert scale (0 = not at all to 4 = very much). The ISI is validated as both a screening and outcome measure, and categories are defined by 0–7 = no clinically significant insomnia, 8–14 = subthreshold insomnia, 15–21 = clinical insomnia (moderate) and 22–28 = clinical insomnia (severe) [21]. In this study internal reliability was excellent for this measure (α = .91).
Statistical analysis
Descriptive statistics were calculated for demographic and cancer-related variables. Means and standard deviations were reported for normally distributed variables, with the exception of a median value reported for the highly skewed variable of time since diagnosis. Frequencies were examined for the levels of insomnia and levels of distress, with chi-square analyses determining potential differences between patients and caregivers as well as across cancer sites. Bivariate correlations were conducted to describe the relationships between predictor and outcome variables (Table 2). Hierarchical linear regression determined if insomnia was associated with demographic characteristics (gender, age and level of education; step 1), disease stage (patients only; step 2) and level of distress (step 3). Categorical variables of gender, age, level of education and stage of disease were coded dichotomously for the analysis. Independent sample t-tests assessed potential differences between patients and caregivers on distress, ISI total score and ISI items.
Results
Prevalence of insomnia
The presence of insomnia symptoms was evident in 59.4 % of patients and 62.9 % of caregivers as defined by a score of 8 or above on the ISI. Moderate to severe levels of insomnia were reported by 27 % of patients and 30 % of caregivers as defined by a score of 15 or above on the ISI. Prevalence rates of insomnia levels did not differ between patients and caregivers, χ 2(3, N = 734) = 1.957, p = .581. Scores of 4 and above on the DT were reported by 62 % of patients and 83 % of caregivers (see Table 3 for frequencies). Prevalence rates of high distress (DT ≥ 4) were significantly different between patients and caregivers, χ 2(1, N = 689) = 31.668, p < .001. When examining rates of insomnia levels and scores of 4 and above on the DT across cancer sites, prevalence rates only differed significantly between cancer sites for patients in relation to insomnia (Fisher’s exact test, p < .01; Table 4). Post-hoc Fisher’s exact tests with a Bonferroni correction revealed that the difference was between the insomnia levels of no clinically significant insomnia and subthreshold insomnia, where patients with prostate cancer were more likely to have no clinically significant insomnia compared to breast and other cancer patients (p < .001 and p < .002, respectively).
Predictors of insomnia
Table 2 presents bivariate correlations between predictor variables and insomnia level. Moderate positive correlations were found between distress level and insomnia level for both patients and caregivers, and modest positive correlations were found between insomnia level, gender and age for patients only.
Tables 5 and 6 present hierarchical multiple regressions for patients and caregivers, respectively. For patients, the combination of age, gender and education in step 1 of the hierarchical multiple regression explained 6 % of the variance in insomnia level, with patient age as the significant predictor. The inclusion of disease stage in step 2 did not increase the explained variance. In step 3, the level of distress contributed an additional 9 % to the explained variance in insomnia level. At this final step, being younger in age (sr2 = .02) and reporting higher distress (sr2 = .09) significantly predicted insomnia level for patients, with the total model explaining 14.8 % of the variance in insomnia level (Adj. R 2 = .14), F(5, 365) = 12.673, p < .001.
For caregivers, the combination of age, gender and education in step 1 did not explain a significant proportion of variance in insomnia level. Inclusion of distress in step 2 of the model increased the explained variance by 10.2 %, with distress emerging as the significant predictor. In the final model, the only significant predictor of a greater insomnia level for caregivers was higher distress (sr2 = .10), with the total model explaining 11.1 % of the variance in insomnia level (Adj. R 2 = .09), F(4,197) = 6.137, p < .001.
Differences in distress and insomnia between patients and caregivers
Descriptive statistics for distress and insomnia scores, including individual ISI items, are presented in Table 7. Caregivers reported significantly higher levels of distress than patients (p < .001). No other significant differences between patients and caregivers were evident.
Discussion
Approximately 60 % of patients and caregivers who called the cancer helpline reported insomnia symptoms, with 28 % of patients and 32 % of caregivers indicating moderate to severe insomnia. Consistent with previous research, these rates are higher than those seen in the general population [5], highlighting an important concern for people calling cancer helplines. Insomnia has been shown to be a pervasive problem that can continue long after cancer treatment ends [27]. However, previous researchers have proposed that cancer patients may believe that their sleep difficulties are due to cancer treatment and will dissipate or may not be aware of existing services and therefore may not seek help [1]. As insomnia has been shown to reduce quality of life and increase psychological distress for a substantial number of people, a mechanism is needed to firstly identify and then treat this disorder.
In a review of the prevalence and non-pharmacological treatment of insomnia in cancer patients, Savard and Savard [28] suggest a stepped care approach to overcoming insomnia, in which initial self-administered education material is the first level of care, with more intense levels of support provided by health professionals if needed [28]. The current study suggests that telephone-based cancer information and support services could potentially address insomnia applying a similar approach by providing self-management materials as a first step, with further referral for in depth insomnia intervention as needed. Specifically, cancer helplines and other related services available around the world could act as the initial point of contact and assessment in a stepped care framework for both distress and insomnia, a proposal that is further supported by findings that these problems appear to be interrelated [23].
Strengths, limitations and implications
The present study demonstrates for the first time that insomnia is prevalent in patients and caregivers calling a cancer helpline. However, owing to study limitations, some caution is needed in generalising from these results. Specifically, we report a low recruitment rate, particularly for caregivers that reflects the challenges of recruiting for research in service-oriented environments. A further limitation may be that while the ISI [22] has been shown to be a reliable and valid tool for assessing the severity of insomnia, more detailed assessment methods such as sleep wake diaries and actigraphy were not possible [14], and we also were not able to assess in depth possible outcomes of sleep disturbance such as daytime sleepiness or fatigue. As well, the cross-sectional nature of the study means that causality cannot be inferred. These are areas for future research.
At present, there is limited evidence about the efficacy of insomnia interventions for people affected by cancer [20], although cognitive behavioural therapy has shown promise in this area [28]. In addition, it has been proposed that existing stress management interventions for cancer patients could be enhanced to treat insomnia through the addition of sleep and fatigue-specific content [31]. Problematically, accessibility of such programmes is limited, and further research is needed to examine ways to integrate interventions for insomnia into standard supportive care after cancer [28]. There may be a potential for insomnia interventions to be provided in a cost-effective manner through telephone-based or internet-based services [26], although we do acknowledge that telephone-based cancer information services may not be available in low resource settings. Finally, caregivers who are spouses of patients are susceptible to insomnia due to a shared sleeping environment, and this is also an area for future research [20].
Conclusion
This study highlights the current concern of insomnia in patients and caregivers calling cancer helplines. The prevalence of insomnia after cancer appears to be higher than in the general population, indicating a burden that could be targeted with appropriate interventions. The association between insomnia and distress in these callers is a pressing issue, and telephone-based services have the potential to address both concerns through brief screening tools such as the Distress Thermometer [24] and Insomnia Severity Index [21] and then applying a stepped care approach [28]. Telephone help services for cancer patients and caregivers, such as those based in non-government organisations, could act as the first line of support for people affected by insomnia and provide a cost-effective approach alleviating already overburdened health services.
References
Ancoli-Israel S (2009) Recognition and treatment of sleep disturbances in cancer. J Clin Oncol 27:5864–5866
Bastien CH, Vallières A, Morin CM (2001) Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med 2:297–307
Beesley VL, Price MA, Webb PM, O'Rourke P, Marquart L, Australian Ovarian Cancer Study Group, Investigators AOCSQoLS (2013) Changes in supportive care needs after first-line treatment for ovarian cancer: identifying care priorities and risk factors for future unmet needs. Psycho-Oncol 22:1565–1571
Berger AM, Sankaranarayanan J, Watanabe-Galloway S (2007) Current methodological approaches to the study of sleep disturbances and quality of life in adults with cancer: a systematic review. Psycho-Oncol 16:401–420
Bin YS, Marshall NS, Glozier N (2012) The burden of insomnia on individual function and healthcare consumption in Australia. Aust NZ J Publ Heal 36:462–468
Bright MA (2007) The national cancer institute’s cancer information service: a premiere cancer information and education resource for the nation. J Cancer Educ 22S:S2–S7
Carney S, Koetters T, Cho M, West C, Paul SM, Dunn L, Aouizerat BE, Dodd M, Copper B, Lee K, Wara W, Swift P, Miaskowski C (2011) Differences in sleep disturbance parameters between oncology outpatients and their family caregivers. J Clin Oncol 29:1001–1006
Chambers SK, Girgis A, Occhipinti S, Hutchison S, Turner J, Morris BA, Dunn J (2012) Psychological distress and unmet supportive care needs in cancer patients and carers who contact cancer helplines. Eur J Cancer Care 21:213–223
Couzi RJ, Helzlsouer KJ, Fetting JH (1995) Prevalence of menopausal symptoms among women with a history of breast cancer and attitudes toward estrogen replacement therapy. J Clin Oncol 13:2737–2744
Daley M, Morin CM, LeBlanc M, Grégoire J, Savard J (2009) The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep 32:55–64
Ekberg K, McDermott J, Moynihan C, Brindle L, Little P, Leydon GM (2014) The role of helplines in cancer care: intertwining emotional support with information or advice seeking needs J Psychsoc Onc
Finney Rutten LJ, Arora NK, Bakos AD, Aziz N, Rowland J (2005) Information needs and sources of information among cancer patients: a systematic review of research (1980–2003). Patient Educ Couns 57:250–261
Girgis A, Lambert SD, McElduff P, Bonevski B, Lecathelinais C, Boyes A, Stacey F (2013) Some things change, some things stay the same: a longitudinal analysis of cancer caregivers’ unmet supportive care needs. Psycho-Oncol 22:1557–1564
Hauri P, Wisbey J (1992) Wrist actigraphy in insomnia. Sleep 15:293–301
Hawkes AL, Hughes KL, Hutchison SD, Chambers SK (2010) Feasibility of brief psychological distress screening by a community-based telephone helpline for cancer patients and carers. BMC Cancer 10:14
Hutchison S, Sargeant H, Morris BA, Hawkes A, Clutton S, Chambers S (2011) A community-based approach to cancer counselling for patients and carers: a preliminary study. Psycho-Oncol 20:897–901
Hutchison SD, Steginga SK, Dunn J (2006) The tiered model of psychosocial intervention in cancer: community based approach. Psycho-Oncol 15:541–546
Jacobsen PB, Donovan KA, Trask PC, Fleishman SB, Zabora J, Baker F, Holland JC (2005) Screening for psychologic distress in ambulatory cancer patients. Cancer 103:1494–1502
Kvale EA, Shuster JL (2006) Sleep disturbance in supportive care of cancer: a review. J Palliat Med 9:437–450
Langford DJ, Lee K, Miaskowski C (2012) Sleep disturbance interventions in oncology patients and family caregivers: a comprehensive review and meta-analysis. Sleep Med Rev 16:397–414
Morin CM (1993) Insomnia: psychological assessment and management. Guilford, New York
Morin CM, Barlow DH, Dement WC (1993) Insomnia: psychological assessment and management. Guilford, New York
Morra ME, Thomsen C, Vezina A, Akkerman D, Bright MA, Dickens C, Hill DJ, Jefford M (2007) The international cancer information service: a worldwide resource. J Cancer Educ 22:S61–S69
National Comprehensive Cancer Network (2002) Practice guidelines in oncology—V.1.2002: distress management (Rep. No. Version 1). In: Editor (ed)^(eds) Book Practice Guidelines in Oncology- V.1.2002: Distress Management (Rep. No. Version 1), City
Osoba D, Zee B, Warr D, Latreille J, Kaizer L, Pater J (1997) Effect of postchemotherapy nausea and vomiting on health-related quality of life. Support Care Cancer 5:307–313
Ritterband LM, Bailey ET, Thorndike FP, Lord HR, Farrell-Carnahan L, Baum LD (2012) Initial evaluation of an Internet intervention to improve the sleep of cancer survivors with insomnia. Psycho-Oncol 21:695–705
Savard J, Ivers H, Villa J, Caplette-Gingras A, Morin CM (2011) Natural course of insomnia comorbid with cancer: an 18-month longitudinal study. J Clin Oncol 29:3580–3586
Savard J, Savard M (2013) Insomnia and cancer: prevalence, nature, and nonpharmacologic treatment. Sleep Med Clin 8:373–387
Savard M-H, Savard J, Simard S, Ivers H (2005) Empirical validation of the Insomnia Severity Index in cancer patients. Psycho-Oncol 14:429–441
Swash B, Hulbert-Williams N, Bramwell R (2014) Unmet psychosocial needs in haematological cancer: a systematic review. Support Care Cancer 22:1131–1141
Vargas S, Antoni MH, Carver CS, Lechner SC, Wohlgemuth W, Llabre M, Blomberg BB, Glück S, DerHagopian RP (2013) Sleep quality and fatigue after a stress management intervention for women with early-stage breast cancer in southern Florida international. J Behav Med :1–11
Acknowledgments
Prof. Chambers is supported by the Australian Research Council Future Fellowship. We gratefully acknowledge the support of Robert McDowall for his assistance with data analysis.
Conflict of interest
Dr Morris, Prof. Glozier, Prof. Dunn and Prof Chambers have no conflict of interest. Prof. Chambers has full control of all the primary data and agrees to allow the journal to review it on request. Drs. Ritterband and Thorndike have equity ownership in BeHealth Solutions, LLC, a company disseminating online interventions, including one for insomnia. The terms of Drs. Ritterband and Thorndike’s arrangement with BeHealth Solutions have been reviewed and approved by the University of Virginia in accordance with its conflict of interest policy.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Morris, B.A., Thorndike, F.P., Ritterband, L.M. et al. Sleep disturbance in cancer patients and caregivers who contact telephone-based help services. Support Care Cancer 23, 1113–1120 (2015). https://doi.org/10.1007/s00520-014-2458-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-014-2458-y