
Summary
Background
In literature, there are conflicting clinical data regarding the incidence of subsequent fracture after balloon kyphoplasty (BK); moreover, the risk of adjacent vertebral fractures has not been well established because there are limited comparative data available with conservatively treated control groups.
Purpose
The purpose of this prospective nonrandomized comparative study was to analyze the incidence and possible risk factors of adjacent level fracture comparing BK with conservative therapy.
Methods
Consecutive patients satisfying the inclusion criteria of acute vertebral fracture pain (occurring within 1–6 weeks of the event and not relieved by oral analgesia) and imaging criteria of acute fracture activity were enrolled. All patients meeting the inclusion criteria were offered BK. The patients who declined BK and agreed to longitudinal evaluation were treated conservatively and constituted the control group.
Results
In 3 out of 46 patients (6.5 %) treated with BK and in 10 out of 61 patients treated conservatively (16.4 %), the adjacent level fracture occurred within 1 year. The degree of local kyphosis and bone mineral density (BMD) were identified as important predictive factors for adjacent level fracture.
Conclusion
These results indicated that BK carries a low risk of adjacent level fractures. Lower BMD values and altered biomechanics in the treated area of the spine due to resistant kyphosis are possible predictive factors for adjacent level fractures. A positive effect of BK over conventional treatment was observed upon reduction of the incidence of adjacent level fracture, vertebral morphology, and pain reduction.
Zusammenfassung
Grundlagen
In der veröffentlichten Literatur bestehen gegensprüchliche Fakten bezüglich Brüchen der Nachbarwirbel nach eingesetzter Ballonkyphoplastie (BK), darüber hinaus steht eine begrenzte Zahl vergleichbarer Untersuchungen zwischen BK und der konservativen Behandlung zur Verfügung.
Ziel
Ziel der präsentierten prospektiven nicht‐randomisierten Studie war es, Häufigkeit und mögliche Risikofaktoren für Frakturen angrenzender Wirbelkörper nach eingesetzter BK im Vergleich mit einer konservativen Therapie einzuschätzen.
Methodik
In Studie eingeschlossen waren Patienten mit klinischen und röntgenologischen Zeichen eines osteoporotischen Wirbelbruches (Alter des Bruches < 6 Wochen), sowie starken Schmerzen trotz Analgesie. Allen Patienten, die Schlüsselkriterien erfüllt haben, wurde die Möglichkeit einer BK‐Therapie als alternative Heilung vorgestellt. Patienten, die sich nicht für die operative Therapie entschieden haben, wurden mit deren Zustimmung weiter konservativ behandelt und repräsentierten die Kontrollgruppe der Patienten.
Ergebnisse
In der Gruppe der Patienten nach durchgeführter BK kam es innerhalb 1 Jahres bei 3 von 36 Patienten (6,5 %) zum Bruch eines angrenzenden Wirbelkörpers. Unter Patienten, welche konservativ behandelt wurden, erlitten innerhalb 1 Jahres 10 von 61 Patienten (16,4 %) einen Bruch eines angrenzenden Wirbelkörpers. Gefunden wurde ein möglicher Zusammenhang zwischen der Häufigkeit von Brüchen angrenzender Wirbelkörper mit lokaler Kyphose und der Mineraldichte der Knochen.
Schlussfolgerung
Die Ergebnisse zeigen, dass die BK eine Methode mit geringem Risiko für Brüche der angrenzenden Wirbelkörper ist. Es besteht ein möglicher Zusammenhang zwischen der Häufigkeit angrenzender Wirbelkörperfrakturen bei Osteoporose und der Häufigkeit angrenzender Wirbelkörperfrakturen bei veränderter Biomechanik der Wirbelsäule aufgrund einer lokalen Kyphose. Bei Patienten, behandelt mit BK, gab es im Vergleich mit konservativ therapierten Patienten nach 1 Jahr im Durchschnitt weniger‐ausgeprägte Deformationen der Wirbel, weniger Brüche angrenzender Wirbelkörper und schnellere Schmerzlinderung.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Surgical treatment for symptomatic osteoporotic painful vertebral compression fractures (VCFs) was in the past usually reserved for fractures with neurological impairment. Results have often been compromised due to extensive nature of the intervention and the poor bone quality secondary to osteoporosis, resulting in poor implant fixation and subsequent patient outcomes.
As minimal invasive spinal surgery techniques evolved, VCFs were targeted for treatment through percutaneous procedure [1]. Balloon kyphoplasty (BK) has been shown to provide benefit to patients with painful VCF in terms of both pain control and disability resolution. The patients typically demonstrate rapid and durable pain relief and often regain lost function.
Despite the demonstrated benefit, there is a great deal of debate about whether BK also increases fracture morbidity by either inducing or facilitating subsequent vertebral fractures. Investigators have attempted to explore this issue through both clinical and biomechanical studies. Published literature on adjacent fractures after BK consists of a single center experience with no control groups. The percentage of subsequent fractures varies from 1 to 26 % [2,3]. It remains unclear whether new vertebral body fractures are simply the result of the natural progression of osteoporosis or if they should be regarded as a consequence of augmentation with bone cement.
Therefore, the purpose of this study was to quantify adjacent VCFs and to analyze any influential factors that could affect them.
Materials and methods
The study protocol was approved by the National Medical Ethics Committee of Slovenia. Written informed consent was obtained from all participating individuals.
In this prospective nonrandomized, nonblinded, controlled study, undertaken between January 2007 and December 2008, 107 consecutive patients with painful osteoporotic VCFs were enrolled.
Male and female patients with painful osteoporotic VCF requiring hospitalization were considered for study enrolment. Inclusion criteria were: osteoporotic VCF; pain lasting < 6 weeks; localized spinal pain that worsened with percussion over the spinal process of the fractured vertebra; no technical reasons why BK could not be done; and suitability for general anesthesia. Exclusion criteria were: presence of a neurological deficit; an osteoporotic vertebral collapse higher than 90 %; an uncooperative patient; bleeding disorders; unstable fractures due to involvement of posterior elements; malignant diseases; and systemic or spinal infection.
The patients with kyphotic deformity > 30°, subsequent sintering at follow up (progressive loss of vertebral height), and pain resistance to analgesics (assessed by a visual analog scale (VAS) score of > 5 points) were offered BK (after being informed of risks and benefits of BK and conservative management). Given sufficient information, patients then decided whether they wanted to undergo BK or conventional treatment. The patients who declined BK and who agreed to longitudinal evaluation constituted our control group.
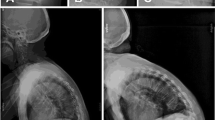
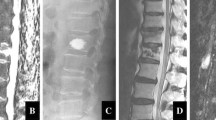
The diagnosis of VCF was established by clinical examination and radiographic evaluation. All patients underwent radiographic evaluation and CT. If needed, the activity of osteoporotic VCF was additionally confirmed by the evaluation of the bony edema in the fat-suppressed sequences (STIR) of MRI. Concomitant laboratory analysis and bone biochemical markers were used to exclude other bone diseases.
The patients were evaluated for pain by using the VAS score, i.e., a scale of 0–10 (with 10 indicating the extreme pain). VAS score of all patients was evaluated at the time of hospital admission and in the BK group on the first day after the procedure to evaluate their clinical response to the procedure. The final assessment of the VAS score was done 1 year after inclusion in the study.
The height of the fractured vertebral body and kyphotic angle of all the patients were measured before treatment and during the follow up. In the fractured vertebral body, vertical heights at their most compressed site were measured and compared to the vertical heights at the same site of both the nearest normal vertebral bodies. We thus calculated the compression rate. We used Cobb’s technique to calculate the segmental kyphotic angle across the fractured level. The measurement was taken from the superior endplate of the vertebra one level above the treated vertebra to the inferior endplate of the vertebral body one level below the treated vertebra [4].
Conservative treatment consisted of a period of relative bedrest and analgesia, with application of a thoracolumbar extension orthosis while standing. The duration of bedrest was restricted to that necessary to achieve a reasonable control of pain upon mobilization.
For patients undergoing BK, a standard preoperative procedure was undertaken. BK procedures were done under general anesthesia. The patients were placed in a prone position with a bolster placed under the sternum and pelvis. Two cannulae were inserted transpedicularly into the crushed vertebral body. Then the two inflatable bone tamps were inserted through cannulae and balloons were dilated simultaneously under C-arm fluoroscopic monitoring. Ballooning pressures did not exceed 200 psi, and a balloon cavity was made in the vertebral body with 3–4 ml per cavity. Then, bone cement containing 1.5 ml of polymethylmethacrylate (PMMA) was injected through the filler. From each side, 2–4 ml of PMMA was injected into most patients. After the PMMA become hard, the bone filler was removed.
The follow up was at 24 h, 6 weeks, 12 weeks, and 1 year after therapy. These time periods were calculated from the day of BK or the day of enrolment into the study in the control group. Visits during the 6th and 12th weeks were not considered in the present analysis.
At the final follow-up examination that is 1 year after study inclusion, we measured bone mineral density (BMD) at the lumbar spine (L1–L4) by dual energy radiograph absorptiometry. A mean value of BMD was calculated for each subject by averaging values from L1–L4, excluding those vertebrae where the augmentation procedure had been carried out.
New vertebral fractures of the thoracic and lumbar spine adjacent to the treated vertebrae were assessed on standing radiographs at follow up. New vertebral fractures were defined as a decrease (compared with baseline radiographs) of 20 % or more, and > 4 mm in any of the three vertebral heights (anterior, middle, or posterior) on follow up.
To investigate the relationship between possible predictors of new vertebral body fracture and the incidence of new vertebral fractures, we included the factors of age, sex, BMD, kyphotic deformity and, in the BK group also the amount of PMMA injected per vertebral body (cement volume) and extravasation of cement (cement leakage).
Statistical analyses
Basic demographic and clinical numerical data are mean ± SD. Outcome measures are mean ± standard error, and analyzed by unpaired t-test. Categorical data are expressed as proportions and analyzed by Pearson’s chi-squared test or Fisher’s exact test.
Changes in VAS score, compression rate, and kyphotic angle from pretreatment to postoperative status and from pretreatment to 1 year after VCF status were analyzed by matched-pairs t-tests or repeated measures analysis of variance. For post-hoc comparisons, the Bonferroni correction (at the alpha level) was used.
The relationship between possible risk factors and adjacent level fractures was analyzed using Pearson’s chi-squared test or Fisher’s exact test. For the purpose of analyses, the variables of patient age, cement volume, pretreatment kyphotic angle, postoperative kyphotic angle, improvement in kyphotic angle, and BMD were dichotomized according to the second quartile.
Thep < 0.05 was considered significant. Data were analyzed using PASW 18 software (SPSS Inc., Chicago, IL, USA).
Results
Out of 107 patients suffering from symptomatic osteoporotic VCF, 46 patients with 51 levels were treated surgically with BK and 61 patients with 64 levels were treated conservatively (control group). Among the patients in the BK group, 41 (89.1 %) had a single vertebral fracture and 5 (10.9 %) had multiple lesions. The level of fracture was distributed between T7 and L3, and was most prevalent on the thoracolumbar junction. Of the 61 patients treated conservatively, 58 (95.1 %) had single vertebral fracture and 3 (4.9 %) had multiple fractures. Fractures were distributed between T7 and L4 and were most prevalent at the thoracolumbar junction.
Table 1 summarizes the demographic and baseline characteristics of treated patients. Significant differences between BK and control group were not observed when comparing results with respect to gender. However, patients in control group were on average older (73.8 vs. 67.8) with lower vertical body height deformity (mean pretreatment compression rate 71.4 vs. 59.4), lower pretreatment local kyphotic angle (6.0 vs. 11.8), and lower pretreatment VAS score (6.7 vs. 8.8) compared with the BK group.
The clinical and radiological characteristics of patients after the BK procedure are presented in Table 2. The mean (± standard error) volume of PMMA cement per body was 5.5 ± 1.1 ml. The proportion of cases with cement extravasation was 8.7 % and intradisc cement leakage was detected in 1 out of 4 patients with cement extravasation. We found a significant improvement in mean compression rate immediately after the BK procedure (81.1 vs. 59.4,p < 0.001). A similar trend was seen for the mean kyphotic angle (4.1 vs. 11.8,p < 0.001). The mean VAS score fell dramatically from the baseline (preoperative) value of about 9 to a value of about 2 immediately after surgery (p < 0.001).
After 1 year, the mean VAS score was slightly lower in the BK group compared with the control group (2.0 vs. 3.8, respectively; Table 3).
No significant difference was found in the mean BMD in the BK and control group (2.7 vs. 2.6, respectively), measured 1 year after the procedure. At the same final visit, patients were examined for new vertebral fractures. In the BK group, three fractures developed in three patients (6.5 %). All of these subsequent fractures were asymptomatic and all were found in patients with a BMD T score equal to, or higher than, − 2.9 SD (mean T score = − 3.3 SD) below the mean of young healthy reference population of the same gender. Postoperative mean local kyphosis in these patients was 11.2° (ranging from 8 to 14°).
In the control group, new vertebral fractures at adjacent levels were detected in ten (16.4 %) patients. In two patients, the adjacent vertebral fracture was symptomatic, making the patients attain control earlier (4 and 7 months after onset of treatment). For the other eight patients, adjacent vertebral fracture was asymptomatic and detected on routine follow up (in three patients after three months and in five patients at the final visit after 1 year).
The changes in VAS score, compression rate and local kyphotic angle through the follow-up period are shown for both groups in Fig. 1. In the BK group the mean VAS score fell dramatically from the baseline (preoperative) value of about 9 to the value of about 2 immediately after surgery. After one year, the VAS score was lower in the BK group compared with the control group (2.0 vs. 3.8,p < 0.001), respectively. At one year, the mean increase in local kyphotic angle was significantly lower in patients treated with BK compared to the control group (5.4° vs. 10.6°,p < 0.001).

Mean VAS score, mean compression, and mean local kyphotic angle in theBK andcontrol group at first visit (pretreatment), after the surgical procedure (post-OP), and at final visit (after 1 year). Mean values ± standard error are shown.a ‘Post-OP’ and ‘after 1 year’ compared to ‘pretreatment’ inBK group (p < 0.001).b ‘After 1 year’ compared to ‘pretreatment’ incontrol group (p < 0.001).c ‘After 1 year’ compared to ‘post-OP’ inBK group (p < 0.001)
The relationship between possible risk factors and adjacent level fractures for both groups is presented in Table 4. In BK group and control group, the local kyphotic angle (p = 0.056 andp = 0.079, respectively) and BMD (p = 0.162 andp = 0.044, respectively) seemed to be related to adjacent level fractures.
Adjacent level fractures occurred in 9 out of 39 (23 %) conservatively treated patients with local kyphosis ³ 5.0° following first vertebral fracture and only in 1 out of 22 (5 %) patients with local kyphosis < 5.0° following first vertebral fracture (p = 0.079). Among patients with BMD greater than or equal to − 2.6, 8 out of 31 (26 %) patients had an adjacent level fracture, while among patients with BMD less than − 2.6 only 2 out of 30 (7 %) patients had an adjacent level fracture (p = 0.044).
Discussion
One of the main concerns in patients treated with BK is that new fractures can develop at nontreated levels following augmentation with bone cement [2].
There are several explanations for adjacent fractures after augmentation of the vertebral body. Rigid cement fixation could theoretically induce degenerative changes in adjacent bone, and the augmented vertebra is likely much stiffer than the adjacent vertebra [5]. It has been suggested that relatively stiff bone cement injected into the osteoporotic bone causes stress peaks on the endplates, leading to fractures at the adjacent levels [6]. Baroud et al. [7] developed biomechanical models to examine cement augmentation on the loading in adjacent vertebrae. In-depth analysis of the model demonstrated that the cement in the treated vertebra acts as pillar, reducing the physiologic inward bulge of the endplates. As a result of this effect, the pressure in the adjacent intervertebral disc increase by up to 19 %. The authors theorized that this shift in adjacent loading is one of the reasons for adjacent fractures.
The clinical results of BK, however, are somewhat confusing. On the one hand, it appears that BK increases the risk for new fractures in adjacent levels. On the other hand, in some studies the BK resulted in a decreased incidence of subsequent vertebral body fractures [8,9]. As neither study had a control group, it was not possible to determine whether the new fractures reflected the natural history of the disease [9] or if they should be regarded as the consequence of stiffness by augmentation with bone cement [10–13].
In biomechanical study, Villarraga et al. [12] showed that the stress and strain of spinal levels adjacent to BK were minimal and were less than the injury tolerance limits of cancellous and cortical bones. Ananthakrishnan et al. [10] reported that BK allowed the disc to generate higher nuclear pressure but that the pressure did not increase above the level of the intact state.
In this comparative study, during follow up, the patients treated conservatively had a higher fracture rate (16.4 %) of adjacent vertebra than patients treated with BK (6.5 %). Therefore, it can be reasonably assumed that fractures that occurred after BK would have occurred if a percutaneous vertebral augmentation procedure had not been done.
Our data indicate that one of the most important factors for a vertebral fracture adjacent to augmented vertebra is the degree of osteoporosis. These results suggest that the BK procedure is usually done in a part of the spine that is already weakened. Hence, adjacent vertebrae are more likely to fail even if the percutaneous augmentation procedure had not been done.
Studies have reported a four times greater risk of developing additional VCFs after the initial VCF than in the population with no VCFs [13]. Hence, the combination of a low lumbar spine BMD and prevalent fractures is a good predictor of an increased fracture risk for adjacent level fractures [14].
It also seems that the occurrence of new VCFs after the percutaneous augmentation procedure is due to altered biomechanics in the treated area of the spine [6]. A kyphotic deformity of the vertebral body, after sustained VCF, increases the anterior stresses in adjacent levels by changing biomechanical loads as they are transferred through the spine. Therefore, a vertebral fracture is a potential increased risk for subsequent fracture in adjacent vertebrae [15]. Height restoration has the potential benefit of reducing post fracture kyphosis, decreased pulmonary-related mortality, and possibly decreasing the incidence of adjacent level fracture [11]. For this reason, BK was developed after the use of vertebroplasty in an attempt to restore vertebral body height in addition to strengthening the body from its previous state.
While the magnitude of benefit obtained with BK over simple stabilization with vertebroplasty continues to be debated, a study by Grohs et al. [16] showed that BK provided a mean correction of the kyphotic angle of 6°, while no significant reduction was achieved with vertebroplasty. It was also reported that at follow-up, they noticed progress in kyphosis (reduction of the height augmented vertebrae) in the BK group in comparison with the VP group where the kyphosis (augmented vertebrae heights) remained practically unchanged. We hypothesize that the repetitive loading crushes the weak cancellous bone between the endplates and cement bolus formed with BK. In contrast, in VP, the cement is injected under more pressure, allowing it to interdigitate in the cancellous bone and to form a continuous cement network between endplates and thus better resist further compression.
We found a significant improvement in mean compression rate immediately after the BK procedure (21.7 %). The mean local kyphotic angle improvement was 7.7°. We also found out that the risk of adjacent level fracture in both groups was higher in patients with higher rates of local kyphosis than in patients with lower rates of local kyphosis. Restoring vertebral height and spinal alignment is thus believed to be important in the treatment of long-term increased morbidity and mortality that arises from VCFs and spinal deformity.
A serious complication of all vertebral augmentation techniques is PMMA cement leakage. It was also reported [17] that cement leakage into the disc increased the risk of new fractures in adjacent vertebral bodies. In the present study, no cement extravasation into the spinal canal or the neural foramen occurred. We found radiographically confirmed cement leakage in 8.7 % of all patients treated with the BK procedure. These results are below average, but cement leakage was only identified on plain radiographs. CT scans identified more leaks than radiographs by a factor of 1.5 [15].
We found cement leakage to be within the disc in one of seven patients with cement leakage. Komemushi et al. [18] found cement leakage into the disc to be a significant predictor of adjacent VCF. In the present study, in cases with intradiscal cement leakage, we did not find any new adjacent fractures. Therefore, we did not find a connection between disk leakage and new adjacent compression fractures.
The mechanism of pain relief after percutaneous augmentation of VCF with PMMA is most commonly through fracture stabilization (although thermal and chemical ablation of nerve endings in the vertebral body may also contribute to pain relief). Pain relief is expected within 24 h after the procedure. Our results confirmed a clear decrease in pain within 24 h after the BK procedure. Typically, the patients in BK group experienced improved mobility within 24 h, and most could bear weight soon after the procedure. The amount and type of pain medication could either be reduced or stopped. It appears that the magnitude of pain relief following a percutaneous augmentation procedure is higher in individuals with acute fractures and shorter periods of fracture-related pain compared to patients with older fractures or long duration of pain. Significant improvement in pain relief in the majority of patients and avoidance of the side effects of long-term analgesic medication are some of the benefits of an early intervention. However, there were no additional significant improvements with regard to pain after 1 year, and differences in improvement between BK and control group diminished in 1 year. A more recent randomized controlled trial confirmed our results that in patients with acute and painful vertebral fractures, BK improved the quality of life, function, mobility, and pain more rapidly than did nonsurgical management, with significant differences in improvement between the groups at one month [19]. In contrast to our results and previously mentioned study in randomized trials that included a control group undergoing a sham procedure, no beneficial effects of vertebroplasty over sham procedure at 1 week or at 1, 3, or 6 months among patients with painful VCFs were found [20,21].
Our study had several limitations. First, only patients who had a new compression fracture on x-ray received the MR imaging in the follow-up period. Asymptomatic new compression fractures with only MR imaging signal intensity change may have been missed. The other drawbacks of the present study included the nonrandomized and nonblinded design, which might have allowed bias and confounding. There were an unequal number of subjects in the two groups, recruited on the basis of consenting or refusing to have BK and a relatively short follow-up period. Therefore, it seems logical that patients in control group were on average older, with lower vertical body height deformity (lower kyphotic angle) and lower pretreatment VAS score compared with the BK group. Unfortunately, in the absence of the ideal dataset, it is difficult to make strong conclusions about the causal relationship between kyphoplasty and adjacent fractures. Ideally randomized, controlled, and prospective trials comparing kyphoplasty with conservative therapy would be performed to explore many of the issues addressed in this article.
In conclusion, comparing BK with nonsurgical care, the present study indicated that the most important factors for adjacent level fractures after an osteoporotic vertebral fracture were the degree of osteoporosis and altered biomechanics of the spine due to local kyphosis. Correction of the vertebral morphology and prevention of further deterioration achieved with BK probably has a positive effect on the spinal biomechanics and thus reduces the incidence of subsequent fracture. Starting antiosteoporosis therapy is essential and is one of the most effective measure in reducing the occurrence of further fracture.
References
Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine (Phila Pa 1976). 2001;26(14):1511–5.
Fribourg D, Tang C, Sra P, Delamarter R, Bae H. Incidence of subsequent vertebral fracture after kyphoplasty. Spine (Phila Pa 1976). 2004;29(20):2270–6; discussion 2277.
Hillmeier J, Grafe I, Da Fonseca K, Meeder PJ, Noldge G., Libicher M, et al. The evaluation of balloon kyphoplasty for osteoporotic vertebral fractures. An interdisciplinary concept. Orthopade. 2004;33(8):893–904.
Kuklo TR, Polly DW, Owens BD, Zeidman SM, Chang AS, Klemme WR. Measurement of thoracic and lumbar fracture kyphosis: evaluation of intraobserver, interobserver, and technique variability. Spine (Phila Pa 1976). 2001;26(1):61–5; discussion 66.
Pflugmacher R, Schroeder RJ, Klostermann CK. Incidence of adjacent vertebral fractures in patients treated with balloon kyphoplasty: two years’ prospective follow up. Acta Radiol. 2006;47(8):830–40.
Polikeit A, Nolte LP, Ferguson SJ. The effect of cement augmentation on the load transfer in an osteoporotic functional spinal unit: finite-element analysis. Spine (Phila Pa 1976). 2003;28(10):991–6.
Baroud G, Nemes J, Heini P, Steffen T. Load shift of the intervertebral disc after a vertebroplasty: a finite-element study. Eur Spine J. 2003;12(4):421–6.
Taylor RS, Taylor RJ, Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine (Phila Pa 1976). 2006;31(23):2747–55.
Movrin I, Vengust R, Komadina R. Adjacent vertebral fractures after percutaneous vertebral augmentation of osteoporotic vertebral compression fracture: a comparison of balloon kyphoplasty and vertebroplasty. Arch Orthop Trauma Surg. 2010;130(9):1157–66.
Ananthakrishnan D, Berven S, Deviren V, Cheng K, Lotz JC, Xu Z, et al. The effect on anterior column loading due to different vertebral augmentation techniques. Clin Biomech (Bristol, Avon). 2005;20(1):25–31.
Belkoff SM, Mathis JM, Fenton DC, Scribner RM, Reiley ME, Talmadge K. An ex vivo biomechanical evaluation of an inflatable bone tamp used in the treatment of compression fracture. Spine (Phila Pa 1976). 2001;26(2):151–6.
Villarraga ML, Bellezza AJ, Harrigan TP, Cripton PA, Kurtz SM, Edidin AA. The biomechanical effects of kyphoplasty on treated and adjacent nontreated vertebral bodies. J Spinal Disord Tech. 2005;18(1):84–91.
Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA 3rd, Berger M. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res. 2000;15(4):721–39.
Movrin I. Prevalence of adjacent level fractures after osteoporotic vertebral compression fractures: a prospective nonrandomized trial comparing percutaneous vertebroplasty with conservative therapy. Acta Medico-Biotechnica. 2011;4(2):34–44.
Yuan HA, Brown CW, Phillips FM. Osteoporotic spinal deformity: a biomechanical rationale for the clinical consequences and treatment of vertebral body compression fractures. J Spinal Disord Tech. 2004;17(3):236–42.
Grohs JG, Matzner M, Trieb K, Krepler P. Minimal invasive stabilization of osteoporotic vertebral fractures: a prospective nonrandomized comparison of vertebroplasty and balloon kyphoplasty. J Spinal Disord Tech. 2005;18(3):238–42.
Lin EP, Ekholm S, Hiwatashi A, Westesson PL. Vertebroplasty: cement leakage into the disc increases the risk of new fracture of adjacent vertebral body. AJNR Am J Neuroradiol. 2004;25(2):175–80.
Komemushi A, Tanigawa N, Kariya S, Kojima H, Shomura Y, Komemushi S, et al. Percutaneous vertebroplasty for osteoporotic compression fracture: multivariate study of predictors of new vertebral body fracture. Cardiovasc Intervent Radiol. 2006;29(4):580–5.
Wardlaw D, Cummings SR, Van Meirhaegghe J, et al. Efficacy and safety of balloon kyphoplasty compared with nonsurgical care for vertebral compression fracture (FREE): a randomized controlled trial. Lancet. 2009;373:1016–24.
Buchbinder R, Osborne RH, Ebeling PR, Wark JD, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med. 2009;361:557–68.
Kallmes DF, Comstock BA, Heagerty PJ, Turner JA, Wilson DJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009;361:569–79.
Conflict of interest
The author declares that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Movrin, I. Adjacent level fracture after osteoporotic vertebral compression fracture: a nonrandomized prospective study comparing balloon kyphoplasty with conservative therapy. Wien Klin Wochenschr 124, 304–311 (2012). https://doi.org/10.1007/s00508-012-0167-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-012-0167-4
Keywords
- Adjacent vertebral fracture
- Balloon kyphoplasty
- Conservative treatment
- Local kyphosis
- Bone mineral density