
Abstract
This study aims to systematically review epidemiological studies that evaluate the relationship between meteorology and the incidence of hip fracture (HF). After a search in Scopus, PubMed, and Embase, two independent authors assessed the relevance of studies and extracted data for description. From each study, we extracted the geographic and temporal scope, design, study variables (meteorological and related to HF), statistical analysis, and estimated associations. Of a total of 134 works, 20 studies were selected. All use an ecological design but one case-crossover. Most studies have been conducted in northern latitudes. The analysis methodology did not take into account the temporal structure of the data in 10 studies (regression and linear correlations); the rest used Poisson regression (7) and ARIMA model (3). Most studies showed significant positive associations with rainfall, especially in the form of snow: HF relative risk (RR) on days with precipitation vs. days without precipitation that ranged from 1.14 (95 % confidence interval (CI)1.04 to 1.24) to 1.60 (95 % CI 1.06 to 2.41), the temperature, with RR by one degree Celsius decline from 1.012 (95 % CI 1.004 to 1.020) to 1.030 (95 % CI 1.023 to 1.037), and wind (3) RR FC windiest days vs. calm days: 1.32 (95 % CI 1.10 to 1.58) to 1.35 (95 % CI 0.88 to 2.08). This review shows that analytic methods are very heterogeneous and poorly adapted to the temporary nature of the data. Studies confirm a certain seasonality, with more fractures in winter and meaningful relationships with meteorological conditions typical of this season.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hip fractures constitute a major public health problem (Romley et al. 2013; Kanis et al. 2013), with the mortality rate 1 year after fracture reported as being approximately 20 % (Schneider and Guralnik 1990, R), comparable with that of cardio-infarction. Initially, it was thought that a therapy consisting of moderate exercise and dietary supplements would be effective in preventing hip fractures, and there is still evidence of the effectiveness of these preventive measures (Morgan 2013; Carter and Hinton 2014). However, these mono-therapies have proven insufficient, forcing researchers to rethink the idea that hip fracture prevention can be accomplished without the use of medication. This has spawned the development of numerous drugs for preventing osteoporosis, such as bisphosphonates, female hormone-like drugs, and PTHs, among others. Many countries have thus updated their guidelines for osteoporosis prevention accordingly (NAMS 2010; BCMA 2013).
In contrast, the role of climate in the incidence of hip fracture has received much less attention, so that its real impact has yet to be fully elucidated. The aim of this paper is to examine the evidence gathered thus far to determine which of the various hypotheses on the role of climate in hip fracture incidence (HFi) is the most accurate.
Hip fracture incidence has been analyzed in numerous studies carried out in various geographic areas. The underlying cause of the vast majority of hip fractures is osteoporosis, a metabolic disease. Almost all studies published to date have found a higher HF incidence in women compared to men as well as an increasing incidence associated with the aging of the populations under study (Dennison et al. 2006). In various countries located at different latitudes, increases in HFi seem to correlate with seasonal changes throughout the year, with a greater incidence of HFs in winter (Douglas 1993; Lau et al. 1995; Chiu et al. 1996; Levy et al. 1998; Bulajic-Kopjar 2000; Crawford and Parker 2003; Lin and Xiraxagar 2006).
The role of climate as a determining factor in HFi has been studied for over 30 years, with conclusive research finding changes in bone tissue quality compatible with osteomalacia at certain times of the year in cases of femoral neck fractures (Aaron et al. 1974).
Nevertheless, studies providing empirical evidence for this association using original data, both on climatic conditions and HFi, are fairly recent. In fact, the first such study, published by Caniggia et al., was conducted in Tuscany, Italy, between 1975 and 1985 (Caniggia and Morreale 1989).
Among the hypotheses that attempt to explain the role of seasonal weather patterns in HFi, two have captured special attention in the past few years. Although not mutually exclusive, they represent different causal models. In the first model, the seasonality of HFi is viewed as a consequence of the influence of climate on bone metabolism. Bolstering this hypothesis are the seasonal changes in vitamin D and parathyroid hormone (PTH) levels (Pasco et al. 2004; Bischoff-Ferrari et al. 2008; Cinar et al. 2014), which may be related to the hours of sun exposure. The other hypothesis centers on short-term associations and maintains that HFs are a consequence of the greater risk of suffering a fall in unfavorable weather conditions. This hypothesis explains the positive and significant association found between HF and weather phenomena such as snow or ice in studies conducted in several northern countries (Parker et al. 1996; Levy et al. 1998). Ascertaining which of the two hypotheses better explains the seasonality of HF or calculating the weight of each factor in contributing to this health problem is not a minor issue since they involve vastly different prevention measures. The prevalence of metabolic changes in the coldest seasons and/or the lower sun exposure would favor dietary supplementation or drug therapy to improve metabolic bone status in adults with an increased risk for HF. The hypothesis which views weather as a physical phenomenon that leads to increased risk of falling calls for information campaigns about avoiding situations in which a fall is more likely in the colder seasons.
To date, no systematic review of the evidence on the relationship between weather conditions and hip fracture incidence has been published. It is thus important to review the literature on this subject, not only in search of scientific evidence, but also to ascertain whether the studies that have been conducted can answer relevant questions about the association between seasonal changes and weather patterns and hip fractures.
In this paper, we have systematically collected, evaluated, and summarized those original studies that have linked various climate variables with the incidence of hip fracture.
Material and methods
This is a systematic review which follows specifically the procedure recommended by the MOOSE (meta-analysis of observational studies in epidemiology) protocol for systematic reviews of observational studies (Stroup et al. 2000) and is generally in accordance with PRISMA (preferred reporting items for systematic reviews and meta-analyses) statement (Moher et al. 2009).
Search criteria and study selection
A search was carried out in all the major relevant databases, with the last review taking place in September, 2103. To this end, we selected information sources appropriate for cataloging this type of study: Medline, Embase, and Scopus. We also manually reviewed the list of references in the selected articles in order to find related citations. Finally, we used the Web of Knowledge page to consult the list of articles that shared references with the articles included in the study.
Search strategies and identification of relevant documents
We used the thesauri from Medline (Mesh) and EMBASE (EMTREE). In addition, we used free text searches with truncations (Hip fracture; Climate; Weather; Meteo*).
We included observational studies that analyzed and reported the association between HFi and at least one weather variable. The latter were defined as the principal variables included in the study of meteorology and commonly collected by weather stations, namely temperature, barometric pressure, wind direction and speed, humidity, and precipitation. The search included studies from any geographic location with no restrictions with regard to language.
The resulting search listings included the title and/or abstract (in most articles), which were used to carry out an initial identification of relevant documents.
Two independent researchers participated in this phase of the study. A document was considered relevant if at least one of the observers viewed it as such. The intra-observer agreement was also calculated, giving a Kappa index value of 0.87. The full text of all articles deemed to be relevant was then retrieved.
Data extraction and assessment of methodological quality
Methodological quality was assessed independently by two observers according to CASPe templates (Critical Appraisal Skills Programme—Spanish) for cohort studies and/or with Osteba checklists for case series.
For each article retrieved, we extracted data related to geographic location and time (latitude, longitude, study period), sample data (cause of HF, diagnostic method, number of patients, percentage of women, and average age), HF incidence, meteorological data (data sources, weather variables), analytical methods (statistical methods), and outcomes (measures of association).
Data analysis
Information was also collected on the association between HFi and the climatic variables used in each study. In cases where results were available from three or more studies, we conducted a meta-analysis using estimates of associations.
Results
Of a total of 134 studies retrieved, 20 were selected as relevant (Fig. 1). The main features of the selected studies are summarized in Table 1.

Flow chart of studies retrieved and finally included in the systematic review
Study periods and geographic location
The earliest study was published in 1989 (Caniggia and Morreale 1989), but analyzed the association between climate and HF from a much earlier period, namely 1975. The study examining the most recent period is that by Murray et al. (Murray et al. 2011), which includes the first part of 2010.
Study period durations differ between studies, from 1 year (Parker and Martin 1994; Lofthus et al. 2001; Atherton et al. 2005) to up to more than 10 years of follow-up (Levy et al. 1998; Caniggia and Morreale 1989; Jacobsen et al. 1995; Mirchandani et al. 2005; Tenías et al. 2009; Modarres et al. 2012). Longer study periods may not only give a more accurate picture of the role of weather phenomena in this health problem, but also serve to distinguish the cyclical component of seasonality.
The studies were conducted in 18 different locations, 16 of which are situated in the Northern Hemisphere. The latitudes of the study locations in the Northern Hemisphere ranged from 59.91° (Oslo) to 22.40° (Hong Kong), while in the Southern Hemisphere, they ranged from −31,25° to −33,87° both in New South Wales, Australia. (Lau et al. 1995; Turner et al. 2011).
The studies collected were mainly conducted in northern countries such as the UK (Parker and Martin 1994; Chesser et al. 2002; Atherton et al. 2005; Murray et al. 2011), Scandinavia (Lauritzen et al. 1993; Lofthus et al. 2001; Frihagen et al. 2011), Central Europe (Burget et al. 2012), and North America [Jacobsen et al. 1995; Levy et al. 1998; Mirchandani et al. 2005; Bischoff-Ferrari et al. 2007; Modarres et al. 2012]. Studies from southern countries remain scarce (Caniggia and Morreale 1989; Tenías et al. 2009; Furelos et al. 2001). We also identified two studies carried out in Asia (Chiu et al. 1996; Lin and Xiraxagar 2006) and another two in Australia (Lau et al. 1995; Turner et al. 2011).
Identification of hip fracture cases
Identification of cases of HF was performed with the aid of emergency room or hospital admission records when the admission diagnosis was listed as hip fracture with either an ICD-9 code 820 or ICD-10 code S72 classification (Turner et al. 2011). Most studies specified the exclusion criteria used, which included high velocity trauma (traffic accidents), pathological fractures (tumor or infectious disease), no history of a fall (Parker and Martin 1994), subtrochanteric fractures (Lofthus et al. 2001; Mirchandani et al. 2005), or readmissions (Lin and Xiraxagar 2006).
The studies used various cutoff points to classify the age of the subjects. These ranged from groups of subjects aged 40 and over to groups of subjects aged 65 and over. Four studies collected data on HF in younger subjects (Lauritzen et al. 1993; Lofthus et al. 2001; Atherton et al. 2005; Frihagen et al. 2011) while one study did not specify subject age (Murray et al. 2011).
Weather variables analyzed
In all cases, the sources of information on meteorological variables were official weather stations close to the respective study areas.
A total of 15 weather variables were analyzed in the various studies, with the most commonly analyzed being (in descending order): temperature (18 studies), precipitation (10), snow (10), icy weather (7), wind (5), relative humidity (5), and sunshine (5).
Statistical methods
The majority of studies utilized regression analysis, with Poisson regression (Douglas 1993) and linear regression (Chiu et al. 1996) predominating. Only two studies used ARIMA modeling (Lin and Xiraxagar 2006; Modarres et al. 2012). Modarres et al. (2014) reanalyzes the series with a nonlinear time series modeling approach (ARMAX-GARCH).
The remaining studies analyzed data using Pearson linear correlation coefficients (Chiu et al. 1996) or other types of tests of comparisons (Levy et al. 1998), e.g., an ANOVA or a t test. One of the studies did not specify which type of analytical method was used.
The unit of analysis used in 12 studies was one day while in the remaining studies it was one month.
Associations
The results obtained are quite heterogeneous, although there is an observable trend in the results for temperature, snow, ice, and sun exposure.
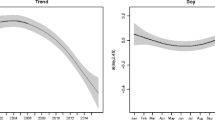
For temperature, despite the different methods, variables, and units of analysis used, most studies show a negative association with the incidence of hip fracture. Thus, of the 18 papers analyzing the relationship between temperature and the incidence of hip fracture, 10 found a significant association while 8 did not. Figure 2 shows the estimates of association found in those studies that quantified this relationship.

Hip fracture risk ratios associated to 1 °C temperature increase (left panel). Correlation coefficients between temperature and hip fracture incidence (right panel)
Almost without exception, snow and ice showed a positive association with the occurrence of HF at all latitudes where studies were conducted.
Studies analyzing some indicator of sun exposure generally used monthly aggregates and showed a negative association with HFi.
The associations between the remaining indicators (precipitation, wind, fog, and atmospheric pressure) and HFi were less consistent, giving both positive and negative associations, usually close to the null value.
Discussion
For this systematic review, we identified and analyzed the relevant empirical evidence published to date examining the relationship between weather conditions and HFi.
The selected studies differ greatly in their design and analysis strategy, making it difficult to compare results. Nevertheless, there is a consistent relationship between HFi and several of the climate variables examined, including temperature, snow, ice, and sun exposure, regardless of location, study design, and analysis strategy used.
Overall, there was an increase in the incidence of HF in the colder months.
Air temperature was perhaps the first meteorological variable to be measured using standardized methods, with reasonably reliable instrumental records of surface temperature with almost global coverage dating from 1850. Temperature is also the variable that best represents seasonal changes. It is partly for this reason that associations between temperature and HFi mostly encompass the seasonal changes observed in HFi time series. It remains unclear if the relationship between temperature and HF is direct or whether it is mediated by other closely related variables, such as sun exposure. In the short term, cold temperatures can cause, among other effects, numbness, which can in turn lead to clumsiness or a lack of coordination in the elderly, increasing the risk of falls. It has been suggested that the underlying cause of HF in patients who have suffered a fall may be a subclinical hypothermia that impairs motor coordination (Bastow et al. 1983). Several authors even point to the influence that an excess of clothing can have on mobility and balance in the elderly (Chiu et al. 1996).
The causal mechanism associated with snow and ice has a simpler, more direct explanation. Falls are more frequent under these conditions (Morency et al. 2012; Beynon et al. 2011), with the increased risk of HF and other types of fractures being frequently observed (Lauritzen et al. 1993; Parker and Martin 1994; Jacobsen et al. 1995; Levy et al. 1998; Bischoff-Ferrari et al. 2007; Frihagen et al. 2011; Modarres et al. 2012).
Sun exposure appears to be an important determinant for bone metabolism (Lips 2001; Bischoff-Ferrari et al. 2011; Bischoff-Ferrari 2012). Indeed, a relationship between sun exposure and levels of vitamin D, PTH, and other bone metabolic indicators has been observed and documented. Furthermore, these associations have been analyzed in the medium term, with monthly (not daily) time aggregates, which makes the relationship more plausible due to the necessary induction period.
Wind, described in several classic epidemiological treatises (Rothman 2012) as an example of an immediate precipitating cause of HFs, has been analyzed in very few studies (Jacobsen et al. 1995; Lau et al. 1995; Mirchandani et al. 2005; Tenías et al. 2009; Modarres et al. 2012). Although a positive association has generally been observed between HFi and both wind duration (Tenías et al. 2009) and speed (Jacobsen et al. 1995; Lau et al. 1995; Mirchandani et al. 2005; Modarres et al. 2012), the small number of studies renders the results inconclusive.
The associations found for the rest of the variables included in our systematic review are much more inconsistent. Either they have been analyzed only sporadically, as is the case with atmospheric pressure, or the results have been so heterogeneous that no general conclusions can be made (relative humidity, precipitation, fog, and other weather conditions).
Particularly striking is the variety of methodological approaches and, above all, of analytical methods used. Virtually, all the publications we found are ecological time series studies, with aggregated measurements (ecological) of both the exposure (weather phenomenon) and the outcome (fracture). Ecological studies have several well-known limitations, including the so-called ecological fallacy (Morgenstern 1995), although time series designs are somewhat less vulnerable to this type of bias than geographic studies. The only exception to this is the study conducted by Tenías et al. (2009), which used a mixed design including ecological methods for exposure and individual analysis for the outcome point. Most studies (Bischoff-Ferrari et al. 2008) use 1 day as the unit of analysis, whereas the rest (Lin and Xiraxagar 2006) use 1 month. The former would be the ideal unit of analysis to study short-term associations while the latter would be better for those that occur in the medium to long-term.
Unfortunately, in many cases, the statistical analysis used is ill suited to the nature of the data. Serial autocorrelation, typical of time series, cannot be adequately controlled for in the absence of specific methods of analysis (e.g., ARIMA) or regression models in which the main components of the time series (trend, seasonality) are controlled for. Even in these cases, the possibility of residual overdispersion would speak for the use of other models that take this phenomenon into account, such as negative binomial regression. The consequence of using a method of analysis that does not take into account the nature of the data may be reflected primarily in the estimates of the standard errors of the regression coefficients, with an overestimation of statistical significance. Recently, nonlinear time series modeling shows that climate variables and HFi doesn’t change linearly with time, and increase exponentially when weather conditions are more adverse (Modarres et al. 2014).
Other possible sources of heterogeneity are subject age, the use of different cutoff points, the type of register used to identify HF cases, and the various exclusion criteria applied (pathological fractures, traffic accidents, etc.). For this reason, we have avoided the temptation of showing results that are solely the product of a meta-analysis, opting instead for a narrative interpretation of the results.
Implications for clinical practice and public health
The ability to intervene with regard to exposure is limited (except for measures that can be put in place to influence climate change), but various preventive measures of a different nature can be implemented. These could include, in the long term, the introduction of alternative therapies to improve bone metabolism (e.g., vitamin D supplementation) at certain times of the year while short-term measures could include information campaigns to lower the risk of falls in elderly patients.
As mentioned in the introduction, there are two main hypotheses explaining the relationship between atmospheric conditions and hip fracture incidence. Although the evidence to date does not allow us to fully rule out either of them in order to confirm one hypothesis over the other, our systematic review of the data supports the idea of short-term associations and the hypothesis that HFs are a consequence of the greater risk of suffering a fall in unfavorable weather conditions.
Advice for future research
Above all, it is necessary to implement multicenter studies with a commonly agreed upon methodology in order to analyze the relationship between weather patterns and HFi in different representative locations. A paradigmatic example of this approach is the European project APHEA, which has managed to conduct a multicenter study of the association between air pollution and various health indicators in various European cities (Katsouyanni et al. 1996).
References
Aaron JE, Gallagher JC, Nordin BE (1974) Seasonal variation of histological osteomalacia in femoral-neck fractures. Lancet 2:84–85
Atherton WG, Harper WM, Abrams KR (2005) A year’s trauma admissions and the effect of the weather. Injury 36:40–46
Bastow MD, Rawlings J, Allison SP (1983) Undernutrition, hypothermia, and injury in elderly women with fractured femur: an injury response to altered metabolism? Lancet 1:143–146
BCMA B. C. M. A. (2013) Osteoporosis: diagnosis, treatment and fracture prevention, p 17. Retrieved from http://www.bcguidelines.ca/pdf/osteoporosis.pdf
Beynon C, Wyke S, Jarman I et al (2011) The cost of emergency hospital admissions for falls on snow and ice in England during winter 2009/10: a cross sectional analysis. Environ Health 10:60
Bischoff-Ferrari HA (2012) Vitamin D and fracture prevention. Rheum Dis Clin North Am 38:107–113
Bischoff-Ferrari HA, Orav JE, Barrett JA, Baron JA (2007) Effect of seasonality and weather on fracture risk in individuals 65 years and older. Osteoporos Int 18:1225–1233
Bischoff-Ferrari HA, Can U, Staehelin HB et al (2008) Severe vitamin D deficiency in Swiss hip fracture patients. Bone 42:597–602
Bischoff-Ferrari HA, Dawson-Hughes B, Whiting SJ (2011) Vitamin D supplementation and fracture risk. Arch Intern Med 171:265
Bulajic-Kopjar M (2000) Seasonal variations in incidence of fractures among elderly people. Inj Prev 6:16–19
Burget F, Pleva L, Kudrna K, Kudrnová Z (2012) Incidence of proximal femur fractures in relation to seasons of the year and weather. Acta Chir Orthop Traumatol Cech 79:140–143
Caniggia M, Morreale P (1989) Epidemiology of hip fractures in Siena, Italy, 1975–1985. Clin Orthop Relat Res 131–138
Carter MI, Hinton PS (2014) Physical activity and bone health. Mo Med 111:59–64
CASPe. Critical Appraisal Skills Programme Español. http://www.redcaspe.org/drupal/. Accessed 3 June 2013
Chesser TJS, Howlett I, Ward AJ, Pounsford JC (2002) The influence of outside temperature and season on the incidence of hip fractures in patients over the age of 65. Age Ageing 31:343–348
Chiu KY, Ng TP, Chow SP (1996) Seasonal variation of fractures of the hip in elderly persons. Injury 27:333–336
Cinar N, Harmanci A, Yildiz BO, Bayraktar M (2014) Vitamin D status and seasonal changes in plasma concentrations of 25-hydroxyvitamin D in office workers in Ankara, Turkey. Eur J Intern Med 25:197–201
Crawford JR, Parker MJ (2003) Seasonal variation of proximal femoral fractures in the United Kingdom. Injury 34:223–225
Dennison E, Mohamed MA, Cooper C (2006) Epidemiology of osteoporosis. Rheum Dis Clin North Am 32:617–629
Douglas AS (1993) Seasonality of hip fracture and haemorrhagic disease of the newborn. Scott Med J 38:37–40
Frihagen F, Pleva L, Kudrna K, Kudrnova Z (2011) Ice and snow in Oslo gave a marked increase in distal radius fractures, but not hip fractures. Osteoporos Int 22:S169–S170
Furelos M, Colino AL, Trobajo JE, Quevedo LA (2001) Hip fractures, seasonal variations and influence of climatological parameters. Rev Ortop Traumatol 45:384–388
Jacobsen SJ, Sargent DJ, Atkinson EJ et al (1995) Population-based study of the contribution of weather to hip fracture seasonality. Am J Epidemiol 141:79–83
Kanis JA, Borgström F, Compston J et al (2013) SCOPE: a scorecard for osteoporosis in Europe. Arch Osteoporos 8:144
Katsouyanni K, Schwartz J, Spix C et al (1996) Short term effects of air pollution on health: a European approach using epidemiologic time series data: the APHEA protocol. J Epidemiol Community Health 50(Suppl 1):S12–S18
Lau EM, Gillespie BG, Valenti L, O’Connell D (1995) The seasonality of hip fracture and its relationship with weather conditions in New South Wales. Aust J Public Health 19:76–80
Lauritzen JB, Schwarz P, McNair P et al (1993) Radial and humeral fractures as predictors of subsequent hip, radial or humeral fractures in women, and their seasonal variation. Osteoporos Int 3:133–137
Levy AR, Bensimon DR, Mayo NE, Leighton HG (1998) Inclement weather and the risk of hip fracture. Epidemiology 9:172–177
Lin H-C, Xiraxagar S (2006) Seasonality of hip fractures and estimates of season-attributable effects: a multivariate ARIMA analysis of population-based data. Osteoporos Int 17:795–806
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
Lofthus CM, Osnes EK, Falch JA et al (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29:413–418
Mirchandani S, Aharonoff GB, Hiebert R et al (2005) The effects of weather and seasonality on hip fracture incidence in older adults. Orthopedics 28:149–155
Modarres R, Ouarda TBMJ, Vanasse A et al (2012) Modeling seasonal variation of hip fracture in Montreal, Canada. Bone 50:909–916
Modarres R, Ouarda TBMJ, Vanasse A et al (2014) Modeling climate effects on hip fracture rate by the multivariate GARCH model in Montreal region, Canada. Int J Biometeorol 58:921–930
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151:264–269
Morency P, Voyer C, Burrows S, Goudreau S (2012) Outdoor falls in an urban context: winter weather impacts and geographical variations. Can J Public Health 103:218–222
Morgan SL (2013) Dietary supplements and medical foods for osteopenia and osteoporosis. J Clin Densitom 16:394–401
Morgenstern H (1995) Ecologic studies in epidemiology: concepts, principles, and methods. Annu Rev Public Health 16:61–81
Murray IR, Howie CR, Biant LC (2011) Severe weather warnings predict fracture epidemics. Injury 42:687–690
(NAMS), N. A. M (2010) Management of osteoporosis in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause (New York, NY) 17(1):25–54. doi:10.1097/gme.0b013e3181c617e6
Parker MJ, Martin S (1994) Falls, hip fractures and the weather. Eur J Epidemiol 10:441–442
Parker MJ, Twemlow TR, Pryor GA (1996) Environmental hazards and hip fractures. Age Ageing 25:322–325
Pasco JA, Henry MJ, Kotowicz MA et al (2004) Seasonal periodicity of serum vitamin D and parathyroid hormone, bone resorption, and fractures: the Geelong Osteoporosis Study. J Bone Miner Res 19:752–758
Romley JA, Jena AB, O'Leary JF, Goldman DP (2013) Spending and mortality in US acute care hospitals. Am J Manag Care 19:e46–e54
Rothman KJ (2012) What is causation? In: Rothman KJ (ed) Epidemiology: an introduction. Oxford University Press, Oxford, p 282
Schneider EL, Guralnik JM (1990) The aging of America. Impact on health care costs. JAMA 263:2335–2340
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Tenías JM, Estarlich M, Fuentes-Leonarte V et al (2009) Short-term relationship between meteorological variables and hip fractures: an analysis carried out in a health area of the Autonomous Region of Valencia, Spain (1996–2005). Bone 45:794–798
Turner RM, Hayen A, Dunsmuir WTM, Finch CF (2011) Air temperature and the incidence of fall-related hip fracture hospitalisations in older people. Osteoporos Int 22:1183–1189
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Román Ortiz, C., Tenías, J.M., Estarlich, M. et al. Systematic review of the association between climate and hip fractures. Int J Biometeorol 59, 1511–1522 (2015). https://doi.org/10.1007/s00484-014-0945-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-014-0945-y