
Abstract
Summary
Observation-driven Poisson regression models were used to investigate mean daily air temperature and fall-related hip fracture hospitalisations. After adjustment for season, day-of-week effects, long-term trend and autocorrelation, hip fracture rates are higher in both males and females aged 75+ years when there is a lower air temperature.
Introduction
This study investigated whether there was an association between fall-related hip fracture hospitalisations and air temperature at a day-to-day level, after accounting for seasonal trend and autocorrelation.
Methods
Observation-driven Poisson regression models were used to investigate mean daily air temperature and fall-related hip fracture hospitalisations for the period 1 July 1998 to 31 December 2004, inclusive, in the Sydney region of New South Wales, Australia, which has a population of 4 million people.
Results
Lower daily air temperature was significantly associated with higher fall-related hip fracture hospitalisations in 75+-year-olds: men aged 75–84 years, rate ratio (RR) for a 1°C increase in temperature of 0.98 with 95% confidence interval (0.96, 0.99), men 85+ years RR = 0.98 (0.96, 1.00), women 75–84 years RR = 0.99 (0.98, 1.00), women 85+ years RR = 0.98 (0.97, 0.99). Moreover, there were fewer hospitalisations on weekends compared to weekdays ranging from RR = 0.81 (0.73, 0.90) in women aged 65–74 years to RR = 0.89 (0.80, 0.98) in men aged 85+ years.
Conclusions
After adjustment for season, day-of-week effects, long-term trend and autocorrelation, fall-related hip fracture hospitalisation rates are higher in both males and females aged 75+ years when there is a lower air temperature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hip fractures in older people result in substantial loss of quality of life and represent a high cost burden to the health care system [1]. Understanding seasonal trends in hip fracture hospitalisations and their associated causes will lead to improved falls risk management and the development of appropriately targeted interventions. Seasonal trends in hip fracture hospitalisation counts have previously been reported in a number of countries, including the USA [2] and Australia [3]. Collectively, these studies have shown increased hip fracture rates during the winter, though this pattern is not consistent across all regions or countries [4, 5].
More recent studies have suggested that the observed seasonal pattern in hip fracture hospitalisation counts may be related to weather patterns, particularly temperature [6–8]. In cooler climates, there also appears to be a link between extreme weather, such as snow or ice, and increased hip fracture rates [6, 7]. Unfortunately, all of these previous studies are methodologically flawed because they did not assess the impact of weather conditions, above and below the normal seasonal pattern and, as such, they relied on assessing correlations through seasonal patterns in the weather series and the hip fracture data series. In other words, the reported associations between the hip fractures and weather data have been driven by the seasonal component and not the day-to-day variability in hip fracture hospitalisation counts.
A recent study assessed the impact of average temperature above and below seasonal norms on hip fracture rates using ARIMA modelling to account for seasonal trend [9]. That study found that a decreased monthly average of mean daily temperature was associated with increased hip fracture rates. The analysis was based on monthly data, which provides weaker evidence than a day-to-day association because it averages out the daily fluctuations above and below climatic mean levels, thereby reducing the power to detect any impact on hip fractures. Further, the use of averaged monthly hip fracture rates does not allow for different numbers of weekend days across the calendar. Use of daily data avoids both of these issues.
This paper overcomes the limitations of previous studies by exploring the relationship between daily hip fracture hospitalisation incidence and air temperature in Sydney, Australia, after adjustment for both seasonality and autocorrelation, that is correlation from one day to the next, within the time series.
Methods
Data
Data were obtained from the New South Wales Admitted Patients Data Collection, a financial year census of all inpatient hospital separations in New South Wales, Australia, commencing during the period 1 July 1998 to 31 December 2004, inclusive. The collection also includes hospitalisations of New South Wales residents in other states. Separations occur when an episode of in-hospital care is completed, that is, when a patient is discharged, transferred, or dies, or has a type-change separation (e.g. when the patient changes from an acute to a rehabilitation patient). Because date of injury is not recorded in the Admitted Patients Data Collection, we have used admission date as a proxy for the date of injury.
Cases were selected with a primary International Classification of Diseases Australian Modification (ICD-10-AM) diagnosis code of hip fracture (S72.0–S72.2) and a first external cause code indicating a fall (W00–W19). As there is no unique patient identifier in the Admitted Patients Data Collection, we attempted to eliminate multiple counting of hip fracture separations for the same case by excluding admissions for which the source of referral was a transfer from another hospital, or for a type-change admission. Only people aged 65+ years at admission were included. We restricted the analysis to people living in the Sydney statistical division [10] to allow direct comparison with available air temperature data. The Sydney statistical division has a population of 4.2 million people, accounting for around 60% of the population of New South Wales.
Population estimates by sex and age group for people aged 65+ years living in the Sydney statistical division were obtained from the Australian Bureau of Statistics. The estimated residential populations at 30 June and 31 December for each year during the study period were interpolated using cubic spline curves to obtain daily values of the estimated population aged 65+ years.
Daily temperature data from all weather stations in the Sydney statistical division were obtained from the Bureau of Meteorology for the period 1 July 1998 to 31 December 2004. Sydney is located at latitude 34°S and longitude 151°E and has a moderate climate. The 22 stations were spread across the most populated parts of the statistical division; only two areas to the north and south west of the region lacked any weather stations and corresponded to the least populated part of the statistical division. Stations with at least 90% of records quality controlled as acceptable by the Bureau of Meteorology were averaged to obtain the mean daily temperature for the Sydney statistical division based on the daily average temperature at each station. To confirm that the daily fluctuations in temperature were similar across the Sydney statistical division, the correlation and cross-correlation coefficients were calculated. The minimum Pearson correlation between any two weather stations was 0.900 and the maximum 0.993 showing that the daily temperature fluctuations were similar across stations and that averaging across the weather stations did not lose important variability.
Statistical analysis
The daily fall-related hip fracture hospitalisation counts were modelled using Poisson regression and the R statistical software package [11]. To account for seasonal trends, 1-year and 6-month periodic sine and cosine terms were included. Temperature was de-seasoned using sine and cosine terms with periods of 1 year, 6 months, 4 months, 3 months and 2 months before inclusion in the Poisson regression model. Preliminary analysis showed a Saturday/Sunday decrease in fall-related hip fracture hospitalisation counts compared to weekdays, so an indicator term representing weekdays/weekends was also included in the model. Linear and quadratic functions of time were included as covariates to represent changes over time in the fall-related hip fracture hospitalisation counts. To account for the autocorrelation in the time series, moving average terms up to lag 7, representing autocorrelations of up to 1 week, were included in the model [12]. This means that the fall-related hip fracture hospitalisation counts on a given day were modelled as being related to what had happened in the previous week, with most emphasis given to the previous day. We fitted separate models by sex and age group (65–74 years, 75–84 years, 85+ years) to allow the relationships to vary across strata and to assess the impact of temperature within each age and sex group.
We modelled the number of fall-related hip fracture hospitalisations in all age–sex groups, using different values of the regression and serial dependence parameters in each group, on day t, denoted by Y t , using the Poisson distribution with mean μ t whose logarithm is
in which a population offset adjusts for any changes to the population with time, the first term is used to model the rate of fall-related hip fracture hospitalisations in the population belonging to the age–gender group, the terms other than the last are the regression effects and the last term allows for serial dependence in the hip fracture hospitalisation counts through the Pearson residuals at previous times, t − 1, t − 7, corresponding to the day before and the week before
This is an observation-driven Poisson regression model [12]. The rate ratios are the exponentiated coefficients in the model and indicate the relative increase or decrease in the fall-related hip fracture hospitalisation counts for a unit increase in a continuous covariate (in our case mean daily temperature) or compared to a reference category for a categorical covariate.
Results
On average, there were more fall-related hip fracture hospitalisations per day for females than males, and this daily average generally increased with age (Table 1). Using Poisson regression, for both males and females aged 65–74 years, there was little evidence of seasonal trend (p > 0.05). In contrast, there was strong evidence of a seasonal trend in all other groups (p < 0.001). Moving average terms were only important and included in the model for males (lag 1 week p = 0.017) and females aged 85+ years (lag 1 day p = 0.048, lag 1 week p = 0.004).
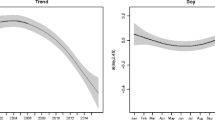
In Table 2, fall-related hip fracture rate ratios and their 95% confidence intervals are shown for the variables of interest. Across all age/sex strata there is a significant weekend effect, with decreased rates on Saturdays and Sundays compared to weekdays. For males aged 65–74 years, there is a significant decrease in counts across the follow-up period. Females of the same age had curvature in the hip fracture hospitalisation counts over the same time comprised of a linear and quadratic component. For all 75- to 84-year-old males and females, there was a significant relationship of fall-related hip fracture hospitalisation counts with mean air temperature. A 1°C decrease in temperature is associated with a 1–2% increase in hip fracture rates, regardless of season. This age group did not show any significant trend with time.
People aged 85+ years had the highest fall-related hip fracture hospitalisation rates. They showed a decrease in fall-related hip fracture hospitalisation rates on the weekends and a temperature effect similar to that for the 75- to 84-year-olds. There was evidence of a decrease in the fall-related hip fracture rate with time for the females in this age group but not the males. Figure 1 shows the fitted model values against the original (raw) hip fracture hospitalisations count data for the females aged 85+ years to demonstrate some of the model aspects. The seasonal variation is evident with a decrease in fall-related hip fracture hospitalisation counts from November through March (summer in Sydney). A long-term trend is not evident in this figure as only 1 year of the data is being presented.

Example of the observed daily hip fracture hospitalisation counts and fitted values from model for females aged 85+ years from July 2003 to July 2004. Source of the hospital data: NSW Admitted Patient Data collection (HOIST), Centre for Epidemiology and Research, NSW Department of Health
The models developed related daily variation in temperature to the fall-related hip fracture hospitalisation rates above and below seasonal norms. It was also important to assess whether the seasonal trend in the hip fracture rates coincided with the seasonal trend in air temperature. This was assessed by plotting the seasonal components from the hip fractures model against the negative of the seasonal trend from the air temperature data as air temperature is lower in winter but the fall-related hip fracture hospitalisation rates are high in winter. Figure 2 shows the seasonal trend in the fall-related hip fracture hospitalisations data overlaid with the negative of the seasonal trend in the temperature data for the males and females aged 75+ years; only 1 year is plotted to highlight the relationships. The peak in the fall-related hip fracture hospitalisation rates follows shortly after the peak in the negative of the temperature, indicating that the maximum fall-related hip fracture rate lags behind the minimum temperature; this can be seen in Fig. 2.

Seasonal trend components for the air temperature (°C) and hip fracture rates demonstrated for 1 year (July 2003 to July 2004). Source of the hospital data: NSW Admitted Patient Data collection (HOIST), Centre for Epidemiology and Research, NSW Department of Health
Discussion
This study is the first to show a relationship between mean daily air temperature and fall-related hip fracture hospitalisations over and above seasonal norms after accounting for autocorrelation in the time series. The study strengthens the evidence for a temperature mechanism for altering hip fracture rates. For the area covered by the Sydney statistical division, amongst people aged 75+ years, there was a significant increase in the rate of fall-related hip fracture hospitalisations as the temperature decreased after adjustment for season, day-of-week effects, long-term trend, population change and autocorrelation. There was a significant decrease in fall-related hip fracture hospitalisation counts on Saturdays and Sundays, compared to weekdays, for all age groups.
We found a significant seasonal trend in fall-related hip fracture hospitalisation rates for both males and females aged 75+ years. This is similar to studies showing seasonal trend in hip fracture rates in the USA [2] and Australia [3]. We found little evidence of a seasonal trend in fall-related hip fracture hospitalisation rates for younger people, and this may be related to the lower incidence of fall-related hip fracture in these age groups [13–15]. While a study in a region of Italy found no evidence of a seasonal pattern [4], that study did not stratify by age group, making it difficult to compare the results directly to our study. It is unlikely, however, that a lack of age-group stratification would hide a seasonal effect given that our seasonal effects are seen in the older age groups corresponding to those with the highest hip fracture rates.
Crude associations between weather and hip fractures have been shown by others [6–8]. However, those studies did not account for seasonal trend or autocorrelation. One study [9] that did account for seasonal trend and autocorrelation only used monthly data. As daily temperature fluctuates within a month, it is necessary to take this into account to obtain more accurate estimates of the effects of temperature on hip fracture rates. We found a temperature effect after adjustment for season, day-of-week effects, long-term trend and autocorrelation, using daily counts giving stronger evidence for a relationship between fall-related hip fracture hospitalisations and temperature than has been shown previously.
A possible underlying biological mechanism for our findings comes from a recent paper [16] which showed that weather conditions affect activity levels in older people. Even though many falls occur indoors, changes in activity levels in response to prevailing weather conditions will lead to changes in falls risk (because people will be more or less active) and thus hip fracture rates. This also provides a plausible explanation of why cold days in both winter and summer are associated with higher hip fracture rates.
Our study showed a decrease in fall-related hip fracture hospitalisation rates on Saturdays and Sundays (the weekend) across all strata; we could not find any similar weekend decrease in the literature. This does not appear to be an effect due to people sustaining a hip fracture on the weekend and not being admitted to hospital until the following Monday, as there was no evidence of an elevated number of admissions on Mondays compared to the rest of the week. Recent research has suggested that almost all cases of hip fracture in older people presenting to emergency departments get admitted [17] so the decrease is also unlikely to be due to a differential admission policy on weekends. Further investigation is needed to determine whether falls resulting in hip fracture hospitalisations occur less frequently on weekends compared to weekdays and if so is due to less activity on weekends or more social and family support.
This study used admission date as a proxy for injury date, which is not recorded on the New South Wales Admitted Patients Data Collection. We believe this would cause non-differential misclassification and bias the results towards the null as the weather on the hospitalisation day could be hotter or colder than the temperature on the injury day if the two are different. It is strongly recommended that routine hospital data collections routinely report date of injury to assist with the linking of treated cases with incident-related factors [18].
The New South Wales Admitted Patients Data Collection does not have a unique patient identifier so incident hip fractures were estimated by excluding admissions for which the source of referral was a transfer from another hospital, or for a type-change admission. These exclusion criteria were chosen based on sensitivity and specificity after comparison with a linked hospital-to-hospital dataset where first admissions for a hip fracture could be identified. Unfortunately, the linked data could not be used for the time-series analysis because month and weekday of the admission were included in the dataset but not the actual admission date or week of admission.
Patients were included in the study based on their residential address and not on the address of the hospital they attended; it is possible that a small number of patients may have been admitted to hospitals throughout New South Wales and even in other states. We believe any such admissions would not unduly affect the results as inclusion of patients potentially experiencing quite different temperatures to that used in the model would reduce any real effect towards the null.
The weather stations were not evenly distributed across the Sydney statistical division with areas to the north and south west of the region lacking data. However, they showed high correlation across the rest of the statistical division indicating that the weather fluctuates similarly across the division and any differences in the two regions without data would be expected to be small and have little impact on the results, particularly when these two regions correspond to low population density areas. The Bureau of Meteorology checks all data from weather stations and indicates whether the readings are considered valid (quality controlled) or not. Stations with a large number of poor readings were excluded from these analyses to reduce measurement bias in the temperature variable.
This study demonstrates an association between air temperature and fall-related hip fracture hospitalisation rates for males and females aged 75+ years in the Sydney statistical division of New South Wales, Australia after adjustment for season, day-of-week effects, long-term trend and autocorrelation. The reasons for this association are unclear and should be the focus of future aetiological and epidemiological studies. These studies should investigate whether air temperature has a direct impact on hip fractures through biological mechanisms or if the association reflects some other indirect mechanism such as change in activity level. The weekend fall-related hip fracture hospitalisations count decrease across all strata also needs further investigation for potential causes. Once the reasons for these trends are fully identified, such as the possibility of reduced physical activity levels in older people, it should be possible to develop appropriate intervention strategies to help reduce the rate of fall-related hip fracture hospitalisations at all times of the year in the future.
References
Sanders KM, Nicholson GC, Ugoni AM, Pasco JA, Seeman E, Kotowicz MA (1999) Health burden of hip and other fractures in Australia beyond 2000. Projections based on the Geelong Osteoporosis Study. Med J Aust 170:467–470
Jacobsen SJ, Goldberg J, Miles TP, Brody JA, Stiers W, Rimm AA (1991) Seasonal variation in the incidence of hip fracture among white persons aged 65 years and older in the United States, 1984–1987. Am J Epidemiol 133:996–1004
Lau EMC, Gillespie BG, Valenti L, O'Connell D (1995) The seasonality of hip fracture and its relationship with weather conditions in New South Wales. Aust J Public Health 19:76–80
Pedrazzoni M, Alfano FS, Malvi C, Ostanello F, Passeri M (1993) Seasonal variation in the incidence of hip fractures in Emilia-Romagna and Parma. Bone 14(Suppl 1):S57–63
Chesser TJS, Howlett I, Ward AJ, Pounsford JC (2002) The influence of outside temperature and season on the incidence of hip fractures in patients over the age of 65. Age Ageing 31:343–348
Levy AR, Bensimon DR, Mayo NE, Leighton HG (1998) Inclement weather and the risk of hip fracture. Epidemiology 9:172–177
Bulajic-Kopjar M (2000) Seasonal variations in incidence of fractures among elderly people [see comment]. Inj Prev 6:16–19
Mirchandani S, Aharonoff GB, Hiebert R, Capla EL, Zuckerman JD, Koval KJ (2005) The effects of weather and seasonality on hip fracture incidence in older adults. Orthopedics 28:149–155
Lin HC, Xiraxagar S (2006) Seasonality of hip fractures and estimates of season-attributable effects: a multivariate ARIMA analysis of population-based data. Osteoporos Int 17:795–806
The Australian Bureau of Statistics (2006) www.abs.gov.au
R Development Core Team (2008) R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna
Davis RA, Dunsmuir WTM, Streett SB (2003) Observation driven models for Poisson counts. Biometrika 90:777–790
Boufous S, Finch CF, Lord SR (2004) Incidence of hip fracture in New South Wales: are our efforts having an effect? Med J Aust 180:623–626
Kannus P, Parkkari J, Koskinen S, Niemi S, Palvanen M, Jarvinen M, Vuori I (1999) Fall-induced injuries and deaths among older adults [see comment]. JAMA 281:1895–1899
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Jarvinen M (1999) Hip fractures in Finland between 1970 and 1997 and predictions for the future [see comment]. Lancet 353:802–805
Sumukadas D, Witham M, Struthers A, McMurdo M (2009) Day length and weather conditions profoundly affect physical activity levels in older functionally impaired people. J Epidemiol Community Health 63:305–309
Boufous S, Finch C, Close J, Day L, Lord S (2007) Hospital admissions following presentations to emergency departments for a fracture in older people. Inj Prev 13:211–214
Hayen AD, Boufous S, Harrison JE (2007) A discussion of the potential benefits to injury surveillance through inclusion of date of injury in hospitalisation data in New South Wales and Australia. NSW Public Health Bull 18:130–132
Acknowledgements
Robin Turner was employed as part of the New South Wales Biostatistical Officer Training Program funded by the New South Wales Department of Health while undertaking this work based at the New South Wales Injury Risk Management Research Centre. Caroline Finch was supported by a National Health and Medical Research Council Principal Research Fellowship.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Turner, R.M., Hayen, A., Dunsmuir, W.T.M. et al. Air temperature and the incidence of fall-related hip fracture hospitalisations in older people. Osteoporos Int 22, 1183–1189 (2011). https://doi.org/10.1007/s00198-010-1306-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-010-1306-2