
Abstract
Objective
Levamisole (LEV) has been used successfully on an alternate-day regime of 2.5 mg/kg in steroid-dependant nephrotic syndrome (SDNS) to maintain remission. This pilot study was carried out between 2010 and 2015 at a single center in Sri Lanka to evaluate the efficacy of LEV prescribed at 2.5 mg/kg daily, which is double the alternate-day dose.
Methods
Sequential children with SDNS, relapsing more than twice in the preceding 12 months and previously treated with LEV and low-dose alternate-day prednisolone (0.1–0.6 mg/kg) were recruited to the study. This group received LEV (2.5 mg/kg) daily with the same dose of alternate-day prednisolone for 1 year. Urine protein excretion was recorded by parents on a daily basis, and the presence of 3+ proteinuria on 3 consecutive days was considered a relapse. Full blood counts and liver function tests were performed every 3 months to monitor for adverse effects.
Results
Sixty-four children were enrolled into the study; six were excluded due to prescription of other immunosuppressive drugs. Median age was 7.9 years; 33 were boys. The number of relapse episodes was 163 [mean per patient 2.8 ± standard deviation (SD) 0.8] in patients on alternate-day LEV and 77 (mean 1.3 ± SD 0.9) for those on daily LEV during the 12-month period of observation. The P value 0.000 (according to the Wilcoxon signed-rank test) was <0.001. No major adverse events were noted.
Conclusions
The prescription of daily LEV is effective and safe for maintaining SDNS remission.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nephrotic syndrome (NS), the most common manifestation of glomerular disease in children, classically refers to the tetrad of massive proteinuria, hypoalbuminemia, hyperlipidemia, and generalized edema [1]. Steroid-sensitive nephrotic syndrome (SSNS) is the predominant type of childhood NS, and 80–90% of children achieve remission with corticosteroid therapy. However, after 8 weeks of corticosteroid therapy orally, ∼80% of children will relapse, requiring further courses of steroids. Half of these children have steroid-dependent nephrotic syndrome (SDNS), in which relapses occur while being treated with reducing doses of steroids [2, 3]. Complications such as sepsis, thrombosis, malnutrition, dyslipidemia, and hypovolemia are risks associated with relapses, while high doses of prednisolone are associated with adverse effects such as hypertension, diabetes, and behavioral disorders [4–6].
Infections in NS arise as a result of reduced immunoglobulin G (IgG), impaired cytokine and complement pathways, depressed T-cell function, and immunosuppressed state caused by drugs. Steroids act by lowering polymorphonuclear activity and capillary permeability to decrease inflammation, whereas cyclophosphamide (CYC), cyclosporine, mycophenolate mofetil (MMF), and levamisole (LEV) are given for steroid sparing. CYC and MMF display long-term efficacy in SDNS patients [7–10]. However, their potential side-effects—such as opportunistic infections, sterility in men, and development of future malignancies are main concerns [11, 12]. Unlike in the developed world, increased risk of infections and subsequent death of children with NS due to sepsis is a major problem in developing countries like Sri Lanka. This may be attributed to overcrowding, inadequate sanitary facilities, lack of routine cleaning and basic infection control measures, and improper waste management commonly seen in hospitals in such countries, all of which can give rise to opportunistic infections in immune-compromised patients [13].
Levamisole, known as an immunomodulatory agent, is used as a steroid-sparing agent mainly in patients with SDNS and is normally administered at a dose of 2–2.5 mg/kg on alternate days for 12–24 months [14]. Several studies have suggested that LEV reduces relapse frequency and reduces steroid dose in SDNS patients, both as a first alternative to steroids and after failure of CYC or cyclosporine [15–17].
This single-center study was conducted to evaluate the efficacy of LEV in maintaining remission in children with SDNS when administered daily, compared with alternate-day administration.
Methods
This single-center pilot study was conducted at the Paediatric Nephrology Unit, Teaching Hospital Peradeniya, Sri Lanka. All procedures were in accordance with the ethical standards of the Scientific and Ethics Committee, Faculty of Medicine of the University of Peradeniya, and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all participants. The study period was January 2010 to January 2015.
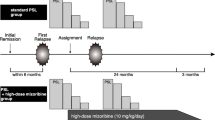
Children with SDNS treated with LEV and low-dose alternate-day prednisolone (0.1–0.6 mg/kg) and relapsing more than twice in the preceding 12 months to the date of enrolment were recruited. Steroid dependence was defined as two consecutive relapses during steroid therapy tapering or within 14 days of cessation of treatment. All patients underwent the standard tapering regimen for prednisolone, in which it was reduced by 2.5 mg every 3 months if the patient was stable on a certain steroid dose and remained free of proteinuria for the preceding 3 months. Previous treatment with any steroid-sparing agents, biopsy histology revealing conditions other than minimal-change nephropathy (MCN), and having secondary NS were criteria for exclusion from the study. Renal biopsy was performed only for specific indications, such as renal impairment, macroscopic hematuria, or other complications.
This group of children received LEV (2.5 mg/kg) daily with alternate-day prednisolone for 1 year, with 40 mg LEV tablets used in quarters; hence, the amount administered was between 2.32 mg and 2.86 mg/kg per dose. The highest prednisolone dose was 0.6 mg/kg and the lowest 0.3 mg/kg. Any relapses were treated with the standard relapse regimen of prednisolone 60 mg/m2 as a single daily dose until remission, followed by 40 mg/m2 on alternate days for 28 days. A patient-held health record was maintained for each patient. Parents were taught to test for and record urine protein daily. The presence of 3+ proteinuria for 3 consecutive days was considered a relapse. Tests for full blood count, serum glutamic–pyruvic transaminase (SGPT), serum creatinine, and blood pressure were reviewed every 3 months, as was urine protein excretion to monitor for any adverse effects.
We analysed the difference in number of relapses, means of neutrophil counts, and liver function tests prior to and after daily LEV treatment initiation. Neutropenia was defined as an absolute neutrophil count (ANC) <1.5 × 109/L [18]. Collected variables were entered into SPSS software version 19 and analyzed using descriptive statistics, paired t test, and nonparametric tests.
Results
Sixty-four participants were enrolled into the study, with the oldest being 14.2 years and the youngest 4.5 years (median 7.95 years). Six children were excluded due to prescription of other immunosuppressive drugs. Of the final study participants, 33 were boys (56.9%), and 25 were girls (43.1%). The number of relapses during the 12-month period in those on alternate-day LEV was 163 (mean 2.81 ± SD 0.78). Baseline characteristics at the beginning of the study are shown in Table 1.
The number of relapses with daily LEV was 77 (mean 1.33 ± SD 0.92) during the 12-month period of the study (Fig. 1). Of the 58 children enrolled, 12 (20.69%) were relapse free and 21 had only one relapse with daily LEV. Hence, 56.9% of children had better outcomes compared with their previous alternate-day regimen. There was a significant reduction in the number of relapses with daily LEV (P value = 0.000) than with the alternate-day regimen (Wilcoxon signed-rank test) (Tables 2 and 3 and Fig. 1).

Mean number of relapses in patients on alternate-day and levamisole (LEV) [mean 2.81, interquartile range (IQR) = 2–3) and daily LEV therapy (mean 1.3, IQR = 1–2)
The total steroid dose given during the year of the study was remarkably lower than that during the year prior to the study (P = 0.000). No serious infection was encountered in either group; minor episodes of infection were not counted. There was no significant difference between mean neutrophil counts, serum creatinine, and SGPT values between groups (P > 0.5). Mean hemoglobin (Hb) level during daily LEV therapy was significantly higher than during the previous year (Table 4). Patient age had no observable impact on the number of relapses prior to or during the study (P > 0.5).
Discussion
This study evaluated 2.5 mg/kg of LEV daily in comparison with 2.5 mg/kg on alternate days to assess its effect on relapses in children with SDNS. Findings demonstrate significant reduction of the number of relapses with this new dose which was accompanied by a lower dose of alternate-day prednisolone of 0.1-0.6mg/kg. The 56.9% of patients who had improved relapse rates and reduced dosages of steroids confirm the efficacy of this new strategy. The simultaneous reduction of the annual steroid dose is also highlighted as an added advantage.
A vast majority of preadolescent children with idiopathic NS have MCN on renal biopsy [19]. More than 90% of children with MCN have steroid-sensitive nephrotic syndrome (SSNS), achieving remission with corticosteroids orally [20]. Most of these patients relapse, with various associated risk factors and complications. Recent research reports interesting findings regarding steroid-sparing drugs for reducing NS relapse rates. In a notable review by Pravitsitthikul et al., the authors conclude that short-term courses of CYC or chlorambucil and prolonged courses of cyclosporine and LEV plus corticosteroids reduce relapse risk in children with SSNS compared with corticosteroids alone. MMF and rituximab are also promising [3]. However, higher relapse rates and more side effects were seen with rituximab and CYC for patients on steroid therapy, and no beneficial effect of MMF in maintaining steroid-free remission was seen [21, 22]. The antihelminthic drug LEV is a synthetic, low-molecular-weight compound that modifies components of host immune reaction [23]. Newer studies show evidence for this immunomodulatory effect of LEV in NS.
MCN is associated with an immune response biased toward type 2, with elevated serum IgE. Findings by Szeto et al. show that LEV selectively induces interleukin 18 (IL-18) gene expression, thereby resetting this imbalance toward type 1. Rats treated with LEV also showed a dose-dependent drop in serum IgE [24]. This restoration and maintenance of immunity might lead to the reduced relapse rate seen in our study. Levamisole also induces expression of glucocorticoid receptor (GCR) activities and signalling in order to directly act on human podocytes and protect them against injury [25].
Infections are a main cause of relapses in NS children in developing countries, as explained previously [26, 27]. Hence, a steroid-sparing drug that would help improve the patient’s comproised immunity would be a better choice than cytotoxic drugs in such settings [1]. In the studies of Sumegi, Madani, and Al-Saran, LEV significantly reduced relapse rates and cumulative annual steroid burden in children with frequently relapsing NS (FRNS) and SDNS, with the majority remaining in total remission [28–30]. In a study by Boyer et al., LEV had the similar beneficial effects over the long term even after ceasing LEV therapy, with added advantages of normalized blood pressure in hypertensive children and improved of height velocity [31]. Bagga et al., in 1997, showed that a significant proportion of SDNS patients could be kept in remission with LEV alone [16]. While all these studies have followed the alternate-day LEV dose, Fu et al. in 2004, reported that daily LEV usage is effective and can be considered in children with FRNS or SDNS when response to alternate-day treatment is unsatisfactory [32]. A retrospective study by Ekambaram et al. also revealed that daily LEV was effective in a majority (77.3%) of FRNS and SDNS children, reducing the cumulative steroid intake and relapse rates [33]. Our results are in concordance with these studies.
The notable reduction in the number of relapses in this study could be due to immune modulation by the higher dose of LEV, with a significantly reduced steroid dose, thus preventing infections and complications that would give rise to relapses. On that account, side effects from higher steroid doses would also reduce as an added advantage.
A number of immune cells, including B cells, monocytes, T cells, and dendritic cells (DC), express nicotinic acetylcholine receptors (nAChR). The influence of nicotine to alter the action of these cells and thereby its anti-inflammatory effect in several diseases such as chronic obstructive pulmonary disease (COPD) and ulcerative colitis, is largely discussed in the literature [34]. Being a nicotinic receptor agonist, LEV might also play a role in the nicotinic pathway of the immune response. Further exploring this aspect will create new therapeutic modalities for NS.
Several studies have shown side-effects such as vasculitis, neutropenia, and liver toxicity associated with LEV usage, although these issues subsided after the treatment ended [35, 36]. SGPT was monitored as a screening test, and based on the results, no liver toxicity was observed. Neutropenia or anemia was not observed in this study. Although Hb level was significantly less during the year with daily LEV, no patient had Hb below the normal range [37]. However, any possible relation between LEV doses and Hb is an interesting point and hence could be investigated in a future study. To conclude, a higher dose of daily LEV along with low alternate-day steroid therapy has better efficacy and is safe in maintaining relapses in children with SDNS.
References
Park SJ, Shin JI (2011) Complications of nephrotic syndrome. Kor J Pediatr 54:322–328
Sinha M, MacLeod R, Rigby E, Clark A (2006) Treatment of severe steroid-dependent nephrotic syndrome (SDNS) in children with tacrolimus. Nephrol Dial Transplant 21:1848–1854
Pravitsitthikul N, Willis NS, Hodson EM, Craig JC (2013) Non-corticosteroid immunosuppressive medications for steroid-sensitive nephrotic syndrome in children. Cochrane Database Syst Rev. doi:10.1002/14651858.CD002290.pub4
Uwaezuoke SN (2015) Steroid-sensitive nephrotic syndrome in children: Triggers of relapse and evolving hypotheses on pathogenesis. Ital J Pediatr 41:19
Niaudet P (2009) Long-Term Outcome of Children with Steroid-Sensitive Idiopathic Nephrotic Syndrome. Clin J Am Soc Nephrol 4:1547–1548
Hall AS, Thorley G, Houtman PN (2003) The effects of corticosteroids on behavior in children with nephrotic syndrome. Pediatr Nephrol 18:1220–1223
Bagga A, Hari P, Moudgil A, Jordan S (2003) Mycophenolate mofetil and prednisolone therapy in children with steroid-dependent nephrotic syndrome. Am J Kidney Dis 42:1114–1120
Bircan Z, Kara B (2003) Intravenous cyclophosphamide is the drug of choice for steroid dependent nephrotic syndrome. Pediatr Int 45:65–67
Mendizábal S, Zamora I, Berbel O, Sanahuja M, Fuentes J, Simon J (2005) Mycophenolate mofetil in steroid/cyclosporine-dependent/resistant nephrotic syndrome. Pediatr Nephrol 20:914–919
Arbeitsgemeinschaft für Pädiatrische Nephrologie (1982) Effect of Cytotoxic Drugs in Frequently Relapsing Nephrotic Syndrome with and without Steroid Dependence. New Engl J Med 306:451–454
Jayaweera A, Abeyagunawardena A (2012) Effectiveness and safety of cyclosporin A therapy in steroid dependent nephrotic syndrome in childhood. Sri Lanka J Child Health 41:176–179
Latta K, von Schnakenburg C, Ehrich JH (2001) A meta-analysis of cytotoxic treatment for frequently relapsing nephrotic syndrome in children. Pediatr Nephrol 16:271–282
Rimi N, Sultana R, Luby S, Islam M, Uddin M, Hossain M, Zaman R, Nahar N, Gurley E (2014) Infrastructure and Contamination of the Physical Environment in Three Bangladeshi Hospitals: Putting Infection Control into Context. PLoS ONE 9(2):e89085
Bagga A (2008) Revised guidelines for management of steroid-sensitive nephrotic syndrome. Indian J Nephrol 18:31–39
Rashid HU, Ahmed S, Fatima N, Khanam A (1996) LEV in the treatment of steroid dependent or frequent relapsing nephritic syndrome in children. Bangladesh Renal J 15:6–8
Bagga A, Sharma A, Srivasta RN (1997) Levamisole therapy in corticosteroid-dependent nephrotic syndrome. Pediatr Nephrol 11:415–417
Tenbrock K, Müller-Berghaus J, Fuchshuber A, Michalk D, Querfeld U (1998) Levamisole treatment in steroid-sensitive and steroid-resistant nephrotic syndrome. Pediatr Nephrol 12:459–462
Newburger P, Dale D (2013) Evaluation and Management of Patients With Isolated Neutropenia. Semin Hematol 50:198–206
International Study of Kidney Disease in Children Nephrotic syndrome in children (1978) Prediction of histopathology from clinical and laboratory characteristics at time of diagnosis. Kidney Int 13:159–165
Trompeter RS, Lloyd BW, Hicks J, White RH, Cameron JS (1985) Long-term outcome for children with minimal-change nephrotic syndrome. Lancet 1:368–370
Webb H, Jaureguiberry G, Dufek S, Tullus K, Bockenhauer D (2015) Cyclophosphamide and rituximab in frequently relapsing/steroid-dependent nephrotic syndrome. Pediatr Nephrol 31:589–594
Deegens J, Wetzels J (2015) Therapy: Maintenance of steroid-free remission in nephrotic syndrome. Nat Rev Nephrol 11:569–570
Renoux G (1980) The General Immunopharmacology of LEV. Drugs 20:89–99
Szeto C, Gillespie K, Mathieson P (2000) LEV induces interleukin-18 and shifts type 1/type 2 cytokine balance. Immunology 100:217–224
Jiang L, Dasgupta I, Hurcombe J, Colyer H, Mathieson P, Welsh G (2015) LEV in steroid-sensitive nephrotic syndrome: usefulness in adult patients and laboratory insights into mechanisms of action via direct action on the kidney podocyte. Clin Sci 128:883–893
Ali SH, Twfeek ZA, Ahmed Azat NF, Hasan AA (2016) Triggering Factors for Relapses in Steroid Sensitive Nephrotic Syndrome. IJCMAS 5:842–851
Moorani K, Raj M (2012) Spectrum of Infections in Children with Newly Diagnosed Primary Nephrotic Syndrome. Pak J Med Res 51:10–14
Sumegi V, Haszon I, Ivanyi B, Bereczki C, Papp F, Turi S (2004) Long-term effects of levamisole treatment in childhood nephrotic syndrome. Pediatr Nephrol 19:1354–1360
Madani A, Isfahani ST, Rahimzadeh N, Fereshtehnejad SM, Hoseini R, Moghtaderi M, Mohseni P, Ataiee N (2010) Effect of Levamisole in steroid-dependent nephrotic syndrome. Iran J Kidney Dis 4:292–296
Al-Saran K, Mirza K, Al-Ghanam G, Abdelkarim M (2006) Experience with levamisole in frequently relapsing, steroid-dependent nephrotic syndrome. Pediatr Nephrol 21:201–205
Boyer O, Moulder J, Grandin L, Somers M (2008) Short- and long-term efficacy of levamisole as adjunctive therapy in childhood nephrotic syndrome. Pediatr Nephrol 23:575–580
Fu LS, Shien CY, Chi CS (2004) Levamisole in steroid-sensitive nephrotic syndrome children with frequent relapses and/or steroid dependency: Comparison of daily and every-otherday usage. Nephron Clin Pract 97:c137–c141
Ekambaram S, Mahalingam V, Nageswaran P, Udani A, Geminiganesan S, Priyadarshini S (2014) Efficacy of levamisole in children with frequently relapsing and steroid-dependent nephrotic syndrome. Indian Pediatr 51(5):371–373
Jonge W, Ulloa L (2009) The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br J Pharmacol 151:915–929
Fu L, Chi C (2000) LEV in steroid-sensitive nephrotic syndrome children with steroid-dependency and/or frequent relapses. Acta Paediatr Taiwan 41:80–84
Bulugahapitiya D (1997) Liver toxicity in a nephrotic patient treated with LEV. Arch Dis Child 76:289
Virgo P (n.d.) Children’s Reference Ranges for FBC. Normal Blood Count Values in Childhood.https://www.nbt.nhs.uk/sites/default/files/Childrens%20FBC%20Reference%20Ranges.pdf. Accessed December 20, 2016
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in the study were in accordance with the ethical standards of the Scientific and Ethics committee, Faculty of Medicine of the University of Peradeniya and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Abeyagunawardena, A.S., Karunadasa, U., Jayaweera, H. et al. Efficacy of higher-dose levamisole in maintaining remission in steroid-dependant nephrotic syndrome. Pediatr Nephrol 32, 1363–1367 (2017). https://doi.org/10.1007/s00467-017-3616-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-017-3616-5