
Abstract
Background
Preoperative colonic stenting for malignant large bowel obstruction (MLBO), also called bridge to surgery (BTS), is considered a great substitute treatment for emergency resection (ER) in the left-sided colon. However, its efficacy in the right-sided colon remains controversial. This systematic review and meta-analysis aimed to compare the postoperative short-term outcomes between BTS and ER for right-sided MLBO.
Methods
A comprehensive electronic literature search throughout December 2020 was performed to identify studies comparing short-term outcomes between BTS and ER for right-side MLBO. The main outcome measures were postoperative complications and mortality rates. A meta-analysis was performed using a fixed-effect or a random-effect method to calculate odds ratios (ORs) with 95% confidence intervals (95% CIs).
Results
Seven studies were included in this meta-analysis, comprising 5136 patients, of whom 1662 (32.4%) underwent BTS and 3474 (67.6%) underwent ER. This meta-analysis demonstrated that BTS resulted in reductions in postoperative complications (OR = 0.78; 95% CI: 0.66–0.92) and mortality (OR = 0.51; 95% CI: 0.28–0.92) than ER.
Conclusion
The results of this meta-analysis indicate that BTS for right-sided MLBO confers preferable short-term outcomes as well as for left-sided. This suggests that BTS results in a reduction of postoperative complications and mortality for right-sided MLBO than ER.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Patients with malignant large bowel obstruction (MLBO) account for 8–34% of those with colorectal carcinoma, which is considered a life-threatening condition that requires immediate intervention [1,2,3]. Emergency one-stage resection for MLBO is associated with significantly higher mortality and morbidity rates than after elective surgery because patients with MLBO are in a poor clinical condition due to several days of reduced intake and impaired intestinal function [4]. Staged surgeries comprised bowel resection and stoma creation, and subsequent closure of the stoma have been performed in some cases [5,6,7]. Regarding left-sided MLBO, many studies have reported good short-term outcomes and safety of long-term prognosis of preoperative decompression with self-expanding metallic stent (SEMS) compared to emergency surgery, which is called a bridge to surgery (BTS) [8,9,10,11,12]. Based on these results, BTS for left-sided MLBO came to be recommended in the updated version of the guidelines from the European Society of Gastrointestinal Endoscopy (ESGE) in April 2020 [8].
In contrast, right-sided MLBO has been traditionally managed with resection and primary anastomosis, which is considered to be safe based on old prospective data showing equivalent morbidity and mortality between emergency and elective surgery in right-sided MLBO [13,14,15]. However, recent studies have demonstrated significantly higher operative risks for emergency resection compared to elective surgery [16,17,18]. Although approximately 32–54% of MLBO cases are located in the right-sided colon, it has been reported that only 5% of reported BTS cases involve the right-sided colon [19]. Studies evaluating the safety and efficacy of BTS for right-sided MLBO are sparse, which has hampered definitive conclusions [20,21,22,23,24,25,26]. Recently, some retrospective cohort studies have shown the promising results for BTS compared to emergency resection (ER). Thus, we conducted a meta-analysis to evaluate the safety and effectiveness of BTS in patients with right-sided MLBO on short-term outcomes with a large sample size (n = 5,136).
Material and methods
The current meta-analysis met the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 2020 [27].
Literature retrieval and study selection
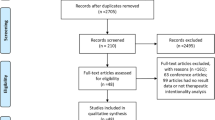
A literature systematic search was performed in MEDLINE (PubMed), Google Scholar, and the Cochrane databases to identify relevant studies published throughout December 2020 (Fig. 1). The search was limited to English language and human studies. The search terms were (‘‘colon cancer” OR “colonic obstruction”) AND (“proximal” OR “right-sided”) AND (“resection” OR “surgery” OR colectomy” OR “colostomy” OR “stoma” OR “stent”). The related article’s function was used to broaden the search. Reference lists of all relevant publications were manually searched for additional studies that were initially overlooked using this search strategy. Methodological index for non-randomized studies (MINORS) tool was used to assess the risk of bias for individual studies [28]. The grading of recommendations assessment, development and evaluation (GRADE) methodology was applied for assessing quality of evidence, and reported in the results with the help of the GRADE Pro Software (McMaster University and Evidence Prime Inc, Ontario, Canada) [29].

Flow chart of study selection according to PRISMA guidelines
Inclusion and exclusion criteria
The inclusion and exclusion criteria were defined priori. The inclusion criteria were as follows: (1) patients with acute malignant proximal or right-sided colonic obstruction, and (2) a comparative study evaluating morbidity and mortality between patients who underwent BTS or ER. ER was defined as emergency one-stage tumor resection. Exclusion criteria were defined as (1) duplicated studies and (2) studies in which predefined outcomes were not reported or it was impossible to extract the number of outcome events.
Data extraction
Each retrieved publication was evaluated independently by two investigators (S.K. and A.M.) for inclusion or exclusion. The following data were extracted from the included studies: the primary author’s name, year of publication, country in which the study was performed, number of institutions, design and duration of the study, number of included participants, and their characteristics, including age, sex, tumor-related variables, performer of SEMS placement, interval from SEMS placement to surgery, and all available short-term outcomes.
Data synthesis and statistical analysis
Dichotomous variables were analyzed by assessing the odds ratio (OR) of short-term adverse outcomes in terms of primary anastomosis, stoma construction, mortality, overall morbidity, surgical site infection, anastomotic leakage, and postoperative ileus, occurring with BTS compared to ER along with 95% confidence intervals (95% CIs). An OR < 1 favored the BTS group, and the point estimate of the OR was considered statistically significant at P < 0.05, if the 95% CI did not include the value 1. The pooled OR was calculated using the Mantel–Haenszel fixed-effects model or DerSimonian–Laird random-effects model to combine ORs for outcomes of interest. Meta-analysis was performed using Review Manager (Version 5.1) for Windows’ (Nordic Cochrane Center, Cochrane Collaboration; Copenhagen, Denmark; http://www.cc-ims.net/RevMan). Cochran’s Chi square-based Q statistic test was used to assess between-study heterogeneity. I2 was used to test for heterogeneity among the included studies. Study heterogeneity was measured using the χ2 and I2 statistics, with χ2 P < 0.05, and I2 ≥ 50% indicating heterogeneity [30]. A fixed-effect model was used to estimate the overall effect if the OR was homogenous; if the OR was non-homogenous, a random-effect model was used [31]. Publication bias was assessed by statistical analysis using Egger’s linear regression test and the rank correlation test (Begg’s test) using ‘‘WINPEPI’’ software (available at http://www.brixtonhealth.com/pepi4windows.html)32,33.
Results
Literature review and included studies
In total, 255 citations were matched during the initial screening. After reviewing the titles and abstracts, 149 studies were excluded. Ninety-nine studies were excluded after full-article evaluation. Therefore, the seven remaining studies [20,21,22,23,24,25,26] (published from 2014 to 2020) were included in the meta-analysis (Fig. 1). The background characteristics of the included studies are listed in Table 1. Five studies [21, 23,24,25,26] originated from Asia and two [20, 22] from the Netherlands. Six [20, 21, 23,24,25,26] of these were retrospective, and one [22] is prospective observational studies. Only one study [25], which is the largest population-based data, applied propensity score matched analysis to adjust potential background confounders. The definitions of right-sided colon in each study were as follows, from the cecum (1) to the hepatic flexure [21], (2) to proximal transverse colon [23], (3) to the entire transverse colon [20, 22, 24,25,26]. Of the 5136 patients included in the meta-analysis, 1662 (32.4%) underwent BTS and 3474 (67.6%) underwent ER. The mean ± standard deviation of MINORS score of included studies was 14.57 ± 1.72, which indicates a fair quality of evidence for non-randomized studies [28]. A comprehensive list of MINORS for included studies is available in Table 2.
According to the GRADE criteria, overall quality of evidence was very low for postoperative complications, primary anastomosis, anastomotic leakage, surgical site infection, and ileus. It was low for mortality, stoma construction and laparoscopic surgery. (Table 3).
Postoperative complications
Postoperative complications were reported in seven studies. The postoperative complication rates in the BTS and ER groups were 19.3% (320/1662) and 31.3% (1088/3474), respectively. The heterogeneity test indicated χ2 = 9.35, and I2 = 36%, demonstrating homogeneity. Therefore, the fixed-model was adopted, and the OR was 0.78 (95% CI: 0.66–0.92) (Fig. 2). This meta-analysis demonstrated that BTS contributed to a significant reduction in postoperative complications compared to ER. We found no significant publication bias by Egger’s test (P = 0.169), or Begg’s test (P = 0.179). Five [19, 20, 23,24,25] of seven studies classified the severity of postoperative complications. However, meta-analysis of severe postoperative complications, which is Clavien–Dindo grading ≥III or requiring reintervention, demonstrated no significant difference between the BTS and the ER groups (OR = 0.98, 95% CI 0.68–1.41).

Meta-analysis of postoperative complications between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER Emergency resection, BTS Bridge to surgery
Mortality
Mortality was reported in seven studies. The postoperative mortality rates in the BTS and ER groups were 0.9% (15/1,662) and 5.2% (181/3474), respectively. The heterogeneity test indicated χ2 = 1.88 and I2 = 0%, demonstrating homogeneity. Therefore, the fixed-model was adopted, and the OR was 0.51 (95% CI: 0.28–0.92) (Fig. 3a). This meta-analysis demonstrated that BTS contributed to a significant reduction in mortality compared to ER. We found no significant publication bias by Egger’s test (P = 0.749), or Begg’s test (P = 0.497).

Meta-analysis of postoperative mortality between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER Emergency surgery, BTS Bridge to surgery
Other outcomes
The other evaluated outcomes are listed in Table 4 and shown in Supplementary Figs. 1–6. The rates of primary anastomosis favored the BTS group over ER group (97.8% [134/137] and 85.9% [1653/1925], respectively), and stoma construction was preferable in the BTS group (2.0% [33/1637] and 11.0% [378/3425], respectively). Both meta-analyses demonstrated significant differences between the groups (OR = 0.31, 95% CI 0.10–0.96; primary anastomosis rate: OR = 0.45, 95% CI 0.25–0.83 for the stoma construction rate) without between-study heterogeneity (χ2 = 0.11, I2 = 0%, P = 0.95, and χ2 = 5.09, I2 = 21%, and P = 0.28, respectively).
Although only 15.7% (547/3474) of ER patients underwent laparoscopic surgery, BTS enabled it in 48.5% (806/1662) of the patients. The OR was significantly higher in the BTS group than in the ER group (OR = 0.21, 95% CI 0.10–0.42). However, the analysis showed significant heterogeneity (χ2 = 18.36, I2 = 67%, P < 0.01).
Regarding detailed postoperative complications, anastomotic leakage, surgical site infection, and ileus were analyzed. Meta-analyses of anastomotic leakage and surgical site infection demonstrated significantly favorable results in the BTS group over ER group (OR = 0.66, 95% CI 0.45–0.96 for the anastomotic leakage: OR = 0.62, 95% CI 0.46–0.82 for the surgical site infection) without between-study heterogeneity. The meta-analysis showed a trend toward frequent ileus in the BTS group, although the difference was not significant (OR = 1.28, 95% CI 0.96–1.71).
Discussion
This meta-analysis was performed to verify an overview of the current literature on the outcomes of acute right-sided MLBO. This review article ultimately included seven studies consisting of 5,136 patients. The results suggested that BTS with subsequent elective resection of right-sided MLBO is associated with significantly lower mortality and postoperative complications when compared to ER.
Although patients with MLBO should be decompressed immediately, emergency resection of the carcinoma is associated with high morbidity and mortality. It may also deteriorate long-term outcomes in that there is no interval for staging workup or screening of synchronous proximal lesions [34]. Thus, staged surgery has been widely performed, which separates decompression of the proximal bowel from resection of the tumor by constructing a stoma [5,6,7].
SEMS was first used by Dohmoto et al. in 1990 for palliation and used for BTS since 1994 [35, 36]. Since then, various reports have indicated that preoperative decompression of bowel obstruction using SEMS reduces postoperative complications and mortality [11, 12, 37]. Recently, the reports of BTS for left-sided MLBO, demonstrating no significant differences in oncologic outcomes compared with ER, were published successively [4, 9, 10, 38]. Based on these reports showing at least equivalent short-term and long-term outcomes compared with ER, recently updated ESGE guidelines for BTS for left-sided MLBO have been recommended within a sufficient shared decision-making process [8].
On the other hand, patients with right-side MLBO are generally managed with emergency resection and primary anastomosis because it is considered relatively safe [39]. However, Kobayashi et al. reported that emergency right hemicolectomy has a significantly higher 30-day mortality rate than elective hemicolectomy (6.0% vs. 0.7%, P < 0.001) in the National Clinical Database of Japan [14]. In addition, previous studies reported high postoperative mortality (8.8–14.5%) and morbidity (32–54.3%) rates in patients who underwent ER for right-sided MLBO [40, 41]. Therefore, the management of patients with right-sided MLBO has become a critical issue. Campbell et al. first reported the use of SEMS in the proximal transverse colon in 1997 [42]. SEMS placement for the proximal colon might be technically challenging because of the long distance from the anus to the obstruction site, increased colon tortuosity, and inappropriate colonic preparation. Further, previous studies showed lower success rates of SEMS placement for the right-sided MLBO than for the left-sided [43]. A recent post hoc analysis of a multicenter trial in Japan demonstrated that the tumor site in the right colon was independently associated with the technical difficulty of SEMS placement (OR 2.5; 95% CI: 1.61–4.01, P < 0.0001) [44]. These factors could have considerable potential for selection bias, and preferable results of BTS compared to ER might be derived from the result of selection bias for “easy-to-stent cases” in all included non-randomized studies for this meta-analysis. However, it is noteworthy that the largest included study by Sakamoto et al. [25] applied propensity score matching and instrumental variable analysis to confirm the robustness of the results. Moreover, they finally demonstrated a lower postoperative complication rate and less stoma creation in BTS than in ER, which was consistent with the results of this meta-analysis. Furthermore, sensitivity analyses excluding the largest study by Sakamoto et al. [25] did not affect the significance in the postoperative complication and maintained the favorable mortality of BTS, although the statistical significance had disappeared (Supplementary Table 1). According to a systematic review by Amelung et al. [19], this is the first systematic review in which BTS for right-sided MLBO has a significantly lower postoperative complication rate (0.8% vs. 23.9%) and surgical mortality (0% vs. 10.8%) than ER. Although this report did not include a comparative study, many patients were included.
The influence to outcomes of the interval from SEMS placement to surgery is one of the concerns in the BTS strategy. Theoretically, longer interval could contribute to a reduction of postoperative complications due to the stabilization of patients’ condition. Our subgroup analyses, divided by median interval of 20 days, demonstrated significant reductions of postoperative complications (OR = 0.45; 95% CI: 0.22–0.92, P = 0.03 for less than 20 days, and OR = 0.81; 95% CI: 0.68–0.96, P = 0.02 for 20 days or more) regardless of length of the interval.
This study had several limitations. As with all systematic reviews, the strength of the conclusions depends on the quality of the primary studies, and there are no randomized controlled trials (RCTs) in our analysis. To draw a conclusion, a reliable RCT is preferred, but conducting RCTs with an adequate sample size on this topic is difficult due to lower incidence of right-sided MLBO compared to left-sided. Furthermore, there was heterogeneity between papers because the sample size, type of SEMS, technical quality of procedures, pathological staging, study design, and follow-up were different. There was also heterogeneity in the definitions of morbidity and mortality. These heterogeneities affect the results considerably.
In conclusion, it should be considered that the postoperative mortality and morbidity rates of surgery for right-sided colon cancer, especially emergency surgery, are higher than previously reported, and BTS may result in a reduction of postoperative complications and mortality for right-sided obstructive colon cancer.
References
Carraro PGS, Segala M, Cesana BM, Tiberio G (2001) Obstructing colonic cancer: failure and survival patterns over a 10 year follow up after one stage curative surgery. Dis Colon Rectum 44:243–250
De Salvo GL, Gava C, Pucciarelli M. Curative surgery for obstruction from primary left colorectal carcinoma: primary or staged resection? (2004) Cochran Database of Syst Rev. DOI: https://doi.org/10.1002/14651858.CD002101.pub2, April 19, 2004
Manceau G, Voron T, Mege D, Bridoux V, Lakkis Z, Venara A, Beyer-Berjot L, Abdalla S, Sielezneff I, Lefèvre JH, Karoui M; AFC (French Surgical Association) Working Group (2019). Prognostic factors and patterns of recurrence after emergency management for obstructing colon cancer: multivariate analysis from a series of 2120 patients. Langenbecks Arch Surg; 404: 717–729
Saida Y, Sumiyama Y, Nagao J, Uramatsu M (2003) Long-term prognosis of preoperative “bridge to surgery” expandable metallic stent insertion for obstructive colorectal cancer: comparison with emergency operation. Dis Colon Rectum 46(10 Suppl):S44–S49
Amelung FJ, Draaisma A, Consten ECJ, Siersema PD, ter Borg F (2017) Self-expandable metal stent placement versus emergency resection for malignant proximal colon obstructions. Surg Endosc 31:4532–4541
Tanis PJ, Paulino PNR, van Hooft JE, Consten ECJ, Bemelman WA (2015) Resection of obstructive left-sided colon cancer at a national level: a prospective analysis of short-term outcomes in 1,816 patients. Dig Surg 32:317–324
Öistämö E, Hjern F, Blomqvist L, Falkén Y, Pekkari K, Abraham-Nordling M (2016) Emergency management with resection versus proximal stoma or stent treatment and planned resection in malignant left-sided colon obstruction. World J Surg Oncol 14:1–7
van Hooft JE, Veld JV, Arnold D, Beets-Tan RGH, Everett S, GötzM, van Halsema EE, Hill J, Manes G, Meisner S, Rodrigues-Pinto E, Sabbagh C, Vandervoort J, Tanis PJ, Vanbiervliet G, Arezzo A (2020). Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline–Update 2020. Endoscopy. 52: 389–407
Yang SY, Park YY, Han YD, Cho MS, Hur H, Min BS, Lee KY, Kim NK (2019) Oncologic outcomes of self-expandable metallic stent as a bridge to surgery and safety and feasibility of minimally invasive surgery for acute malignant colonic obstruction. Ann Surg Oncol 26:2787–2796
Matsuda A, Miyashita M, Matsumoto S, Matsutani T, Sakurazawa N, Takahashi G, Kishi T, Uchida E (2015) Comparison of long-term outcomes of colonic stent as “bridge to surgery” and emergency surgery for malignant large-bowel obstruction: a meta-analysis. Ann Surg Oncol 22:497–504
Huang X, Lv B, Zhang S, Meng L (2014) Preoperative colonic stents versus emergency surgery for acute left-sided malignant colonic obstruction: a meta-analysis. J Gastrointest Surg 18:584–591
Allievi N, Ceresoli M, Fugazzola P, Montori G, Coccolini F, Ansaloni L (2017) Endoscopic stenting as bridge to surgery versus emergency resection for left-sided malignant colorectal obstruction: an updated meta-analysis. Int J Surg Oncol. https://doi.org/10.1155/2017/2863272,Jul5,2017
Lee YM, Law WL, Chu KW, Poon RTP (2011) Emergency surgery for obstructing colorectal cancers: a comparison between right-sided and left-sided lesions. J Am Coll Surg 192:719–725
Smithers BM, Theile DE, Cohen JR, Evans EB, Davis NC (1986) Emergency right hemicolectomy in colon carcinoma: a prospective study. Aust N Z J Surg 56:749–752
Goligher JC, Smiddy FG (1957) The treatment of acute obstruction or perforation with carcinoma of the colon and rectum. Br J Surg 45:270–274
Smothers L, Hynan L, Fleming J, Turnage R, Simmang C, Anthony T (2003) Emergency surgery for colon carcinoma. Dis Colon Rectum 46:24–30
Kobayashi H, Miyata H, Gotoh M, BabaH KW, Kitagawa Y, Nakagoe T, Shimada M, Tomita N, Sugihara K, Mori M (2014) Risk model for right hemicolectomy based on 19,070 Japanese patients in the National Clinical Database. J Gastroenterol 49:1047–1055
Matsuda A, Yamada M, Matsumoto S, Sakurazawa N, Kawano Y, Sekiguchi K, Yamada T, Matsutani T, Miyashita M, Yoshida H (2019) Blood galectin-3 levels predict postoperative complications after colorectal cancer surgeries. J Nippon Med Sch 86(3):142–148
Amelung FJ, de Beaufort HWL, Siersema PD, Verheijen PM, Consten ECJ (2015) Emergency resection versus bridge to surgery with stenting in patients with acute right-sided colonic obstruction: a systematic review focusing on mortality and morbidity rates. Int Colorectal Dis 30:1147–1155
van den Berg MW, Sloothaak DAM, Dijkgraaf MGW, van der Zaag ES, Bemelman WA, Tanis PJ, Bosker RJI, Fockens P, ter Borg F, van Hooft JE (2014) Bridge-to-surgery stent placement versus emergency surgery for acute malignant colonic obstruction. Br J Surg 101:867–873
Ji WB, Kwak JM, Kang DW, Kwak HD, Um JW, Lee SI, Min BW, Sung NS, Kim J, Kim SH (2017) Clinical benefits and oncologic equivalence of self-expandable metallic stent insertion for right-sided malignant colonic obstruction. Surg Endosc 31:153–158
Amelung FJ, Consten ECJ, Siersema PD, Tanis PJ (2016) A population-based analysis of three treatment modalities for malignant obstruction of the proximal colon: acute resection versus stent or stoma as a bridge to surgery. Ann Surg Oncol 23:3660–3668
Kye BH, Lee YS, Cho HM, Kim JG, Oh ST, Lee IK, Kang WK, Ahn CH, Lee SC, Park JK, Kim HJ (2016) Comparison of long-term outcomes between emergency surgery and bridge to surgery for malignant obstruction in right-sided colon cancer: a multicenter retrospective study. Ann Surg Oncol 23:1867–1874
Morita S, Yamamoto K, Ogawa A, Naito A, Mizuno H, Yoshioka S, Matsumura T, Ohta , Suzuki R, Matsuda C, Hata T, Nishimura J, Mizushima T, Doki Y, Mori M, Clinical Study Group of Osaka University (CSGO), Colorectal Group (2019). Benefits of using a self-expandable metallic stent as a bridge to surgery for right-and left-sided obstructive colorectal cancers. Surg Today. 49: 32–7
Sakamoto T, Fujiogi M, Lefor AK, Matsui H, Fushimi K, Yasunaga H (2020) Stent as a bridge to surgery or immediate colectomy for malignant right colonic obstruction: propensity-scored, national database study. Br J Surg 107:1354–1362
Li B, Cai SL, Lv ZT, Zhou PH, Yao LQ, Shi Q, Qi ZP, Sun D, Yalikong A, Xu EP, Xu JM, Zhong YS (2020) Self-expandable metallic stenting as a bridge to elective surgery versus emergency surgery for acute malignant right-sided colorectal obstruction. BMC Surg 20:1–10
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021). The PRISMA statement: an updated guideline for reporting systematic reviews. BMJ. 29;372:n71.
Slim K, Nini E, Forest D, Kwiatkowsi F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716
Balshem H, Helfand M, Schünemann HJ et al (2011) GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 64:401–406
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Egger M, Smith GD, Schneider M, Minderet C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Abramson JH (2011) WINPEPI updated: computer programs for epidemiologists, and their teaching potential. Epidemiol Perspect Innov 8:1–9
Runkel NS, Schlag P, Schwarz V, Herfarth C (1991) Outcome after emergency surgery for cancer of the large intestine. Br J Surg 78:183–188
Dohmoto M, Rupp KD, Hohlbach G (1990) Endoscopicallyimplanted prosthesis in rectal carcinoma. Dtsch Med Wochenschr 115:915
Cwikiel W, Andren-Sandberg A (1993) Malignant stricture with colovesical fistula: stent insertion in the colon. Radiology 186:563–564
Gregorio MA, Mainar A, Rodriguez J, Alfonso ER, Tejero E, Herrera M, Medrano J, D’Agostino H (2004) Colon stenting: a review. Semin Intervent Radiol 21:205–216
Gianotti L, Tamini N, Nespoli L, Rota M, Bolzonaro E, Frego R, Redaelli A, Antolini L, Ardito A, Nespoli A, Dinelli M (2013) A prospective evaluation of short-term and long-term results from colonic stenting for palliation or as a bridge to elective operation versus immediate surgery for large-bowel obstruction. Surg Endosc 27:832–842
Weiss JM, Pfau PR, O’Connor ES, King J, LoConte N, Kennedy G, Smith MA (2011) Mortality by stage for right-versus left-sided colon cancer: analysis of surveillance, epidemiology, and end results–Medicare data. J Clin Oncol 29:4401
Lee YM, Lau WM, Chu KW, Poon RT (2001) Emergency surgery for obstructing colorectal cancers: a comparison between right-sided and left-sided lesions. J Am Coll Surg 192:719–725
Hsu TC (2005) Comparison of one-stage resection and anastomosis of acute complete obstruction of left and right colon. Am J Surg 189:384–387
Campbell KL, Hussey JK, Eremin O (1997) Expandable metal stent application in obstructing carcinoma of the proximal colon: report of a case. Dis Colon Rectum 40:1391–1393
Cho YK, Kim SW, Lee BI, Lee KM, Lim CH, Kim JS, Chang JH, Park JM, Lee IS, Choi MG, Choi KY, Chung IS (2011) Clinical outcome of self-expandable metal stent placement in the management of malignant proximal colon obstruction. Gut Liver 5:165–170
Kuwai T, Yamaguchi T, Imagawa H, Yoshida S, Isayama H, Matsuzawa T, Yamada T, Saito S, Shimada M, Hirata N, Sasaki T, Koizumi K, Maetani I, Saida Y (2019) Factors related to difficult self-expandable metallic stent placement for malignant colonic obstruction: A post-hoc analysis of a multicenter study across Japan. Gastrointest Endosc 31:51–58
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
None.
Author information
Authors and Affiliations
Contributions
Study concept and design: SK, AM, TY, RO, SS, GT, TI, and KT. Literature search and data collection: SK and AM. Statistical analysis and interpretation of data: SK, AM, KU, SK, and TM. Drafting of manuscript: SK and AM. Revising the manuscript: HS and TY. Study supervision: TY and HY. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Disclosures
Drs. Shintaro Kanaka, Akihisa Matsuda, Takeshi Yamada, Ryo Ohta, Hiromichi Sonoda, Seiichi Shinji, Goro Takahashi, Takuma Iwai, Kohki Takeda, Koji Ueda, Sho Kuriyama, Toshimitsu Miyasaka, and Hiroshi Yoshida have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
464_2022_9071_MOESM1_ESM.tif
Supplementary file1—Supplementary Figure 1. Meta-analysis of primary anastomosis between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 144 kb)
464_2022_9071_MOESM2_ESM.tif
Supplementary file2—Supplementary Figure 2. Meta-analysis of stoma construction between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 146 kb)
464_2022_9071_MOESM3_ESM.tif
Supplementary file3—Supplementary Figure 3. Meta-analysis of laparoscopic surgery between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 156 kb)
464_2022_9071_MOESM4_ESM.tif
Supplementary file4—Supplementary Figure 4. Meta-analysis of anastomotic leakage between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 146 kb)
464_2022_9071_MOESM5_ESM.tif
Supplementary file5—Supplementary Figure 5. Meta-analysis of surgical site infection between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 146 kb)
464_2022_9071_MOESM6_ESM.tif
Supplementary file6—Supplementary Figure 6. Meta-analysis of ileus between bridge to surgery and emergency resection. Odds ratio is shown with 95% confidence intervals. ER: emergency surgery; BTS: Bridge to surgery. (TIF 144 kb)
Rights and permissions
About this article

Cite this article
Kanaka, S., Matsuda, A., Yamada, T. et al. Colonic stent as a bridge to surgery versus emergency resection for right-sided malignant large bowel obstruction: a meta-analysis. Surg Endosc 36, 2760–2770 (2022). https://doi.org/10.1007/s00464-022-09071-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09071-7