
Abstract
Introduction
Little is known about the predictors of increased ambulatory costs following open ventral and incisional hernia repair (VIHR); however, postoperative complications would be expected to be associated with an increased burden on outpatient resources. The purpose of this study is to evaluate the impact of perioperative factors on outpatient resource utilization following VIHR.
Methods
With IRB approval, the surgery scheduling system was queried to identify all cases of VIHR done at our institution over 3 years. Cases with other procedures done at time of VIHR were excluded. National Surgical Quality Improvement Program clinical data, physician billing data which included market and payor across cases, and medical record review data were combined and evaluated in order to quantify care and predictors of usage during the 6 months postoperatively.
Results
Data were analyzed for 308 patients. Median patient age was 52 years (SD = 13.3), and over half were female. The number of outpatient visits to the surgical office varied from 0 to 18 [median = 2; interquartile range (IQR) = 1–3]. CDC Wound Class >1 was associated with increase of mean 1.4 visits (IQR: 0.5–2.3); p = 0.003. Component separation, longer duration of operation, and increased mesh size were also predictive of increased number of office visits (p < 0.01). Postoperative infected seroma/seroma requiring drainage added a mean 2.3 visits (IQR: 1.3–3.3), (p < 0.001); and deep wound infection added a mean 3.9 visits (IQR: 1.9–5.9) (p < 0.001).
Conclusions
Postoperative complications confer a significant burden for patients and to the outpatient surgical office. In an era in which improved quality and cost-efficiency has become imperative, measures to decrease risk of postoperative complications particularly for more complex VIHR would be expected to decrease resource utilization and increase value of care.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Ventral hernia repairs are commonly performed procedures with an estimated 350,000 done in the U.S. annually [1]. Patient outcomes following open ventral and incisional hernia repair (VIHR) frequently are calculated in terms of surgical site infection (SSI) and hernia recurrence. The outcomes of nearly one-third of patients that undergo complex ventral hernia repair is thought to be adversely affected by SSI [2, 3], and SSI is the most common reason for hospital readmission following all surgical procedures, including VIHR [4]. The unplanned 30-day readmission rate following hernia repair surgery is thought to be between 5 and 10% of all patients. [4, 5].
All complications following ventral hernia repair do not necessarily require readmission to the hospital. For example, a patient may experience an abdominal wall abscess or postoperative seroma requiring an in-office incision and drainage which may be managed on an outpatient basis. These patients, however, may require home health care nursing services, wound care supplies, additional outpatient office visits, and may require additional time off work than would have been required if complication had not occurred, all of which increase ultimate health care and societal costs attributed to VIHR.
Surgical site infection diagnosed after hospital discharge and not associated with hospital readmission is not as well-defined or as well-documented as SSI diagnosed during the index surgical hospitalization. Perencevich et al. determined that SSI identified during the eight-week post-discharge time period following index procedure was associated with an increased resource utilization, including increased number of outpatient office visits, emergency room visits, radiology, and home health care services. [6] While post-discharge hospital costs, including costs of emergency room visits and readmissions postoperatively, specifically associated with ventral hernia repair have been explored [7], little information is available in recent literature concerning the ambulatory resource utilization associated with VIHR and predictors of increased outpatient resource utilization.
As part of long-term efforts to improve quality of patient care in the U.S., the Centers for Medicare and Medicaid Services (CMS) have embarked on implementation of a fundamentally changed system for evaluating and paying for healthcare. The Medicare Access and CHIP Reauthorization Act of 2015 provided guidelines for health care payment based on the quality and effectiveness of care provided with new reimbursement strategies granting that physicians will be increasingly paid based on outcomes of the care provided as opposed to volume of care [8]. In an effort to improve quality of care of patients undergoing VIHR, patient outcomes, not only from the index hospitalization, but also during the extended time period after discharge, must be defined. In this study, we are interested in quantifying the ambulatory resource utilization and determining the predictors of increased resource utilization associated with VIHR during the 180-day postoperative period.
Methods
With Institutional Review Board approval, the surgery scheduling system at the University of Kentucky, a large academic medical center with a primarily rural-based patient population, was queried to identify all cases of open VIHR (CPT code 49560, 49561, 49565, or 49566) done over 3 years: October 1, 2011, through September 30, 2014. Cases during which other planned procedures, such as hysterectomy or cholecystectomy were performed, were excluded from analysis. National Surgical Quality Improvement Program (NSQIP) data which included 30-day post-discharge clinical data, physician billing data which included market and payor across cases, and medical record review data were combined and evaluated in order to quantify care and predictors of usage during the 6 months postoperatively. The medical record review identified postoperative complications documented post-discharge in the outpatient surgical office notes to augment the NSQIP data. The medical record review also quantified number of visits to the outpatient surgical office during the six-month time period post-discharge.
The primary outcome of postoperative office visits was compared between binary variables using t tests without assuming equal variances. Categorical variables were compared using analysis of variance. Continuous variables were correlated with visits using Spearman’s rho test for correlation. Significance was set at p < 0.05. SPSS statistical software (IBM Corp., Armonk, New York) version 23 was used for all calculations.
Results
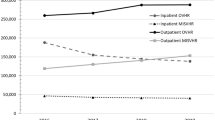
Open VIHRs performed between October 1, 2011, through September 30, 2014, were analyzed; two cases with 30-day deaths were excluded from the analyses leaving a total of 308 cases for analysis. Across all cases, the number of outpatient surgical office visits varied from 0 to 18 [median = 2; interquartile range (IQR) = 1–3] (Fig. 1). Slightly over half of the study population was female, and the mean age was 52.1 years ± 13.3 years (Table 1). Approximately half of the patients had residence in either the primary (county in which the University of Kentucky hospitals are located) or secondary (regional) market. Significant preoperative predictors of increased number of postoperative office visits included residence in secondary market and history of COPD (Table 1).

Clinic visits in 6-month postoperative period
More than three-fourths of the VIHR cases (83.7%) were done electively, and 80% were clean cases (Centers for Disease Control and Prevention Wound Class I). The median length of hospital stay was 5 days, and half of the cases were open repair for recurrent hernia. Numerous operative variables were associated with significantly increased or decreased number of office visits in the six-month post-discharge time period (Table 2) Operations lasting 181 min or longer were associated with a median 2.5 surgical office visits as compared to operations lasting 120 min or less being associated with median of one office visit (Fig. 2). Patients that had surgery on an outpatient basis had significantly few postoperative office visits, and cases that were done on an emergent basis also had fewer office visits postoperatively. Postoperative complications were associated with significant increase in number of office visits during the six-month post-discharge time period (Table 3).

Operative duration (minutes) and number of office visits
Discussion
Increasing emphasis is placed on quality of postoperative patient care to ensure not only surgery effectiveness, but also efficient resource application. Prevention of postoperative complications following hernia repair, would be expected to improve patient long-term outcomes and to reduce costs. SSIs have been shown to increase risk of hernia recurrence, thereby creating a greater burden on patients and the healthcare system. [9] While previous VIHR studies have shown that preoperative factors such as gender, ASA class, and hypertension increase hospital costs [7], the current study indicates that the same factors do not increase resource utilization post-discharge. Instead, the increased resource utilization in the postoperative time period appears to be related for the most part to increased intraoperative complexity and postoperative complications, particularly SSI.
Sanger et al. showed that major challenges that impact patients’ ability to manage post-discharge surgical wound complications following open colorectal and ventral hernia repair surgeries include required knowledge for wound monitoring, self-efficacy of wound monitoring, and accessible communication with providers [10]. The current study quantifies ambulatory resource utilization, especially as it relates to postoperative complications associated with surgical wounds to determine the postoperative financial impact of VIHRs. Previous studies have monitored post-discharge SSIs following hernia repairs [11], and established preoperative risk stratification systems to determine SSI risk but have not quantified the clinical impact [12, 13].
Patients with residence in secondary markets had significantly more office visits than patients from other markets, possibly indicating deficient access to care for the tertiary and primary market patients (Table 1). Additionally, uninsured patients had significantly fewer office visits compared with insured patients, also indicating possible lack of access or lack of transportation for these patient groups. Awareness of patient market and/or payor status may be necessary in arranging follow up and in patient education strategies in order to avoid failure to identify postoperative complications at an early stage or to avoid complete loss to follow up. If an offsite clinic were available closer to county of residence or if follow up could be arranged to occur with a patient’s primary care physician, given inability to travel to the academic medical center, patients may be better served. It is possible that uninsured patients may not return for an increased level of care postoperatively due to concern of inability to pay. Perhaps these patients have decreased utilization in general, but likely concern of inability to pay was predictive.
Early follow up with the patient’s primary care provider (PCP) following open thoracic aortic aneurysm repair has been shown to decrease 30-day hospital readmission rates; however, early PCP follow up after ventral hernia repair was not found to reduce readmission rate [14]. The authors noted that identifying high-risk patients for early PCP follow up would be the key to avoiding need for readmission. The surgical office has an obligation to assure that patient concerns are addressed and patient phone calls are managed to assist patients to seek care in a timely manner and at a location appropriate according to the patients’ postoperative issues. In the current study, CDC Wound Class greater than I, component separation technique, more than one piece of mesh implanted, and requirement of transfusion in the 72 h postoperative time period, all indicators of increased complexity, were associated with increased number of office visits. Routine early follow up in the surgical office, particularly for complex hernia repair patients would be expected to identify SSI at an early stage which may prevent emergency room visits or hospital readmission, both of which have a greater financial impact on the healthcare system than office visits. With identification of the higher risk VIHR patients, it would be expected that earlier surveillance in the surgical office, early follow up with PCP and telephone monitoring may decrease hospital readmissions and severity of wound complications.
Prevention of postoperative complications would be expected to result in not only decreased outpatient resource utilization following VIHR, but also decreased number of hospital readmissions and potentially lead to reduction in the overall negative financial impact [15] that has been associated with VIHR. Enhanced recovery after surgery (ERAS) protocols are evidence-based quality improvement pathways of patient care reported to be associated with improved patient outcomes. Enhanced recovery protocols for ventral hernia repair have been linked to decreased length of hospital stay, quicker return of bowel function, and reduced readmission rates [16]. Standardization of care during the perioperative time period, such as that occurring with ERAS protocols, has potential to benefit patients undergoing VIHR. If complication rates could be reduced, ultimately the adverse impact on the healthcare system and patients also could be reduced. Nonetheless, identification of risk factors for increased outpatient resource utilization is a necessary step in the process of enhancing the value of postoperative hernia care.
Limitations impacting this study largely involve resources needed to adhere to a therapeutic postoperative management plan. Just over half (52%) of the patients studied lived in tertiary locations. Therefore, it is conceivable that these patients may have postponed care of their ventral hernias until they were required to present with emergent cases and then not return for routine postoperative care. If the patients had a follow-up appointment within the 180-day time-frame, this information was included in the data set. However, not all patients returned for follow-up appointments, likely for the reasons described above such as transportation difficulty or no emergent needs. A total of 12 patients (3.8%) did not return to our facility for follow-up visit. For any patient that did not follow up with surgeon, that information was noted in our dataset. We do not know for this study if the patients sought care at an outside facility or if they did not require postoperative care. Without returning for postoperative care, if complications occurred, they were not recorded and these patients, thereby, utilized less resources. Also, 4.5% of the patients studied were uninsured, which could have also skewed the data towards less resource utilization despite other preoperative factors.
Conclusions
Postoperative complications following VIHR add a significant burden to both patients and the outpatient surgical office. In an era in which improved quality and cost-efficiency has become imperative, measures to decrease risk of postoperative complications particularly for more complex VIHRs would be expected to decrease clinical resource utilization and increase value of care. Further study is needed to understand the relationship between increased outpatient resource utilization and hospital readmission, costs and personal burdens for patients that develop complications following ventral hernia repair.
References
Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Holzman MD (2012) Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 16:179–183. doi:10.1007/s10029-011-0879-9
Liang MK, Goodenough CJ, Martindale RG, Roth JS, Kao LS (2015) External validation of the ventral hernia risk score for prediction of surgical site infections. Surg Infect 16:36–40. doi:10.1089/sur.2014.115
Roth JS, Brathwaite C, Hacker K, Fisher K, King J (2015) Complex ventral hernia repair with a human acellular dermal matrix. Hernia 19:247–252. doi:10.1007/s10029-014-1245-5
Merkow RP, Ju MH, Chung JW, Hall BL, Cohen ME, Williams MV, Tsai TC, Ko CY, Bilimoria KY (2015) Underlying reasons associated with hospital readmission following surgery in the United States. JAMA 313:483–495. doi:10.1001/jama.2014.18614
Nguyen MT, Li LT, Hicks SC, Davila JA, Suliburk JW, Leong M, Kao LS, Berger DH, Liang MK (2013) Readmission following open ventral hernia repair: incidence, indications, and predictors. Am J Surg 206:942–949. doi:10.1016/j.amjsurg.2013.08.022
Perencevich EN, Sands KE, Cosgrove SE, Guadagnoli E, Meara E, Platt R (2003) Health and economic impact of surgical site infections diagnosed after hospital discharge. Emerg Infect Dis 9:196–203
Plymale MA, Ragulojan R, Davenport DL, Roth JS (2017) Ventral and incisional hernia: the cost of comorbidities and complications. Surg Endosc 31:341–351. doi:10.1007/s00464-016-4977-8
CMS.gov. Retrieved at https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/value-based-programs/macra-mips-and-apms/macra-mips-and-apms.html
Rosen MJ, Bauer JJ, Harmaty M, Carbonell AM, Cobb WS, Matthews B, Goldblatt MI, Selzer DJ, Poulose BK, Hansson BM, Rosman C, Chao JJ, Jacobsen GR (2017) Multicenter, prospective, longitudinal study of the recurrence, surgical site infection, and quality of life after contaminated ventral hernia repair using biosynthetic absorbable mesh: the COBRA study. Ann Surg 265:205–211. doi:10.1097/SLA.0000000000001601
Sanger PC, Hartzler A, Han SM, Armstrong CA, Stewart MR, Lordon RJ, Lober WB, Evans HL (2014) Patient perspectives on post-discharge surgical site infections: towards a patient-centered mobile health solution. PLoS ONE 9:e114016. doi:10.1371/journal.pone.0114016
Taylor EW, Duffy K, Lee K, Noone A, Leanord A, King PM, O’Dwyer P (2003) Telephone call contact for post-discharge surveillance of surgical site infections. A pilot, methodological study. J Hosp Infect 55:8–13
Meguid RA, Bronsert MR, Juarez-Colunga E, Hammermeister KE, Henderson WG (2016) Surgical risk preoperative assessment system (SURPAS): I. Parsimonious, clinically meaningful groups of postoperative complications by factor analysis. Ann Surg 263:1042–1048. doi:10.1097/SLA.0000000000001669
Leekha S, Lahr BD, Thompson RL, Sampathkumar P, Duncan AA, Orenstein R (2016) Preoperative risk prediction of surgical site infection requiring hospitalization or reoperation in patients undergoing vascular surgery. J Vasc Surg 64:177–184. doi:10.1016/j.jvs.2016.01.029 Epub 2016 Feb 27
Brooke BS, Stone DH, Cronenwet JL, Nolan B, DeMartino RR, MacKenzie TA, Goodman DC, Goodney PP (2014) Early primary care provider follow-up and readmission after high-risk surgery. JAMA Surg 149:821–828. doi:10.1001/jamasurg.2014.157
Totten CF, Davenport DL, Ward ND, Roth JS (2016) Cost of ventral hernia repair using biologic or synthetic mesh. J Surg Res 203:459–465. doi:10.1016/j.jss.2016.02.040
Majumder A, Fayezizadeh M, Neupane R, Elliott HL, Novitsky YW (2016) Benefits of multimodal enhanced recovery pathway in patients undergoing open ventral hernia repair. J Am Coll Surg 222:1106–1115
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Roth is a speaker for Bard, has grants with Bard, Life Cell, Gore, and MTF, and is a consultant for Life Cell. Mr. Wade, Dr. Plymale, Dr. Johnson, Dr. Davenport, Dr. Madabhushi, Mr. Tancula, and Ms. Mastoroudis have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Wade, A., Plymale, M.A., Davenport, D.L. et al. Predictors of outpatient resource utilization following ventral and incisional hernia repair. Surg Endosc 32, 1695–1700 (2018). https://doi.org/10.1007/s00464-017-5849-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5849-6