
Abstract
Background
Endoscopic mucosal resection (EMR) or radical surgical resection are the standard treatment options for patients with early Barrett´s adenocarcinoma (EBAC). Endoscopic submucosal dissection (ESD) is a new endoscopic technique, which allows—in contrast to EMR—endoscopic en-bloc resection of neoplastic lesions greater than 2 cm with complete histological evaluation of the resected specimen. In contrast to Western countries, Barrett´s esophagus is less common in Asia indicating the low volume of published data of ESD in EBAC in Japanese series. Therefore, the aim of the present study is to describe the results of ESD in patients with EBAC performed in a German tertiary referral center.
Methods
Between November 2009 and April 2014 ESDs were performed in 22 patients with histologically proven EBAC. Data were given for the en-bloc, the R0, the R0 en-bloc, and the curative resection rate as well as for the complication and the local recurrence rate.
Results
ESD was technically possible in all of the 22 patients. 20 of the resected EBAC were mucosal carcinomas, whereas in two patients the tumor showed submucosal invasion. The en-bloc, R0, R0 en-bloc, and curative resection rates were 95.5, 81.8, 81.8 %, and77.3 %, resp. Complication rate was 27.3 % (perforation n = 1, bleeding n = 2, stenosis n = 3). In case of curative tumor resection, only one local tumor recurrence (5.9 %) occurred after a medium follow-up of 1.6 years.
Conclusions
Despite the small number of patients and a relatively short follow-up, the present data underline the value of ESD, especially in case of curative resections in the definite and less invasive therapy of EBAC. Attention should be drawn toward subsquamous extension of EBAC requiring a sufficient safety margin as an obligate condition for curative R0 resections. Due to the required learning curve and the management of potential complications, ESD should be restricted to greater endoscopic centers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Barrett´s carcinoma is an adenocarcinoma arising from Barrett´s mucosa, which is defined as columnar metaplasia of the distal esophagus. In contrast to squamous cell carcinomas, adenocarcinomas of the distal esophagus have increased during the last two decades especially in the Western world [1]. The conversion rate from non-neoplastic to neoplastic Barrett´s mucosa and even to Barrett´s carcinoma amounts to 0.5–1 % per year [2, 3]. In general, the prognosis of patients with advanced Barrett´s carcinoma is poor, and the 5-year survival rate is less than 20 % [3–6]. Therefore, the detection of neoplastic Barrett´s mucosa or early Barrett´s carcinoma (EBAC) is beneficial for the patients, although treatment strategies for EBAC remain controversial. Currently, endoscopic mucosal resection (EMR) or radical surgical resection are the standard treatment options for EBAC with similar outcome [7]. The disadvantage of EMR is that en-bloc resection is limited to a diameter of 2 cm. Larger lesions must be resected in piecemeal technique without the possibility of a histological confirmation of the R0-status leading to a higher rate of local recurrence [8–11].
Endoscopic submucosal dissection (ESD) of neoplastic lesions of the gastrointestinal tract is a rather new endoscopic technique, which allows—in contrast to EMR—endoscopic en-bloc resection of lesions greater than 2 cm with a complete histological evaluation of the resected specimen, including the resection margins [9, 11–13]. This technique has been proven to be safe and effective for the curative resection of superficial neoplasms in the whole gastrointestinal tract [11–15]. In contrast to Europe and North America, Barrett´s esophagus is less common in Japan indicating the relatively low volume of published patients with ESD in EBAC in large Japanese series [15]. On the other hand, ESD of EBAC is restricted in Western countries to greater endoscopic centers, and only limited data is available in Europe [8, 14, 16]. Therefore, the aim of this study is to describe the results of ESD in patients with EBAC performed in a German tertiary referral center. Data were given for the en-bloc, R0, R0 en-bloc, and curative resection rate as well as for the complication and the local recurrence rate after a follow-up period.
Materials and methods
Between November 2009 and April 2014 ESDs were performed in 22 patients (20 men, 2 women; mean age 64.1 years; range: 45.7–86.7 years) with histologically proven EBAC in the Asklepios Clinic Barmbek (Hamburg, Germany).
Prior ESD, adequate clinical examinations were performed (abdominal ultrasound, endoscopic ultrasonography, computed tomography of the chest and/or abdomen) to exclude lymph-node and distant metastases.
ESD was performed under general anesthesia (n = 20) or under conscious sedation with propofol (n = 2).
All ESDs were carried out by two endoscopists (S.F. n = 19, N.Y. n = 3) who had a large amount of experience in EMR and ESD in the whole gastrointestinal tract.
We only used endoscopes with HDTV and NBI function (Olympus GIF H 180, GIF H 180J, GIF HQ 190) for a better delineation of the neoplastic lesion and a transparent cap at the distal end of the endoscope.
The ESD procedure consists of five steps: setting of coagulation markers, submucosal lifting, mucosal incision, submucosal dissection, and removal of the resected specimen. A typical circumferential ESD is shown in Fig. 1. At the beginning, coagulation marks around the detected neoplastic area with a safety margin of at least 10 mm were placed using Dual-Knife (KD-650U; Olympus; Japan) followed by submucosal injection of diluted indigo carmine or toluidine blue solution in order to lift and separate the mucosal and submucosal layer from the muscular layer. Then, circumferential mucosal incision and submucosal dissection of the whole marked area was performed using different knifes (Dual-Knife (KD-650U; Olympus, Japan), Hook-Knife (KD-620LR, Olympus, Japan), Hybrid-Knife (ERBE Elektromedizin GmbH, Tübingen, Germany). In case of bleeding, the underlying vessel was coagulated with the tip of the Dual-Knife or in case of more severe bleeding by coagulation forceps (CoagGrasper FD-410 LR; Olympus, Japan). Radiofrequency systems were used from Martin (MB1; Martin GmbH, Tuttlingen, Germany) and Erbe (VIO 300D; ERBE Elektromedizin GmbH, Tübingen, Germany).

Endoscopic submucosal dissection (ESD) in a patient with EBAC. A Long-segment Barrett´s esophagus with early adenocarcinoma. B Mucosal incision. C Submucosal dissection. D “Final cut”. E Circumferential resected area. F Resected specimen (12 × 5 cm). G Histology showing EBAC (pT1 m L0 V0 G1 R0); (HE staining, magnification ×40)
The resected specimens were stretched and fixed onto cork with needles after the removal. The maximum diameter of the specimen was measured and recorded. Histopathological evaluation was performed by one experienced pathologist (B.F.) including the type and grading of neoplasia as well as the vertical mucosal and submucosal depth of tumor invasion. The completeness of vertical and lateral resection margins of the EBAC was evaluated by determination of tumor-free margins (R0), tumor-infiltrated margins (R1), or undetermined margins due to coagulation artifacts or in case of piecemeal resection (Rx). Involvement of lymphatic vessels and veins was investigated additionally.
Endoscopic resection was only described as curative in well- (G1) and moderately differentiated tumors (G2) if the lateral and vertical resection margins were tumor free (R0) and histology showed no lymphatic (L0) and no vascular involvement (V0). In cases with submucosal tumor invasion, curative resection was only accepted in cases of submucosal tumor invasion of less than 200 µm. In patients with un-differentiated tumors (G3) or in cases with tumor positive resection margins (R1-resection) and/or lymphatic or vascular involvement (L1 and/or V1) and/or deeper submucosal tumor invasion, radical surgical resection was performed.
After ESD, all patients were administrated proton pump inhibitors for 48 h intravenously. Oral proton pump inhibitor therapy was continued for at least 3 months after the intervention. In order to detect early bleeding complications, follow-up endoscopy was performed the day after the initial procedure. Oral intake of food was allowed if the base of the ESD-ulceration was clean without any bleeding signs.
Complications such as perforation (defined as a visible hole in the esophageal wall and/or clinical signs of perforation with mediastinal emphysema and/or mediastinitis) and delayed bleeding were recorded. Procedural bleedings that could be managed endoscopically and did not cause prolonged hospitalization were not defined as complications.
Regular follow-up examinations including biopsies from the initial neoplastic area were performed 3, 6, and 12 months and then, yearly after the endoscopic tumor resection.
Data collection and statistical analysis were performed by means of descriptive statistics (mean and range) and analyzed with Microsoft Office Excel 2010 and IBM SPSS Statistics 19.
Results
Between November 2009 and April 2014, 22 ESDs in patients with EBAC were performed. The mean age of the patients was 64.1 years (range: 45.7–86.7 years) and includes 20 men and 2 women.
ESD in the described technique was possible in all of the patients. In only one case, snaring of the nearly complete resected specimen was used additionally in order to reduce procedural time. The average procedural time was 114.4 min (range: 40–250 min) and the average size of the resected specimens was 13.7 cm2 (mean length 4.4 cm; range: 1.8–12.0 cm/mean width 2.7 cm; range: 1.5–5.0 cm).
Histology
Twenty (90.9 %) of the resected neoplastic lesions showed an adenocarcinoma limited to the mucosa. Of these lesions, 15 were histopathologically defined as well-differentiated adenocarcinoma (G1) and 5 as moderately differentiated adenocarcinoma (G2) based on a Barrett´s mucosa. In contrast, only two of the resected lesions (9.1 %) showed an adenocarcinoma with submucosal invasion. Both were histopathologically defined as moderately differentiated adenocarcinoma (G2). Lymphatic and/or vascular involvement or un-differentiated tumors were not seen in any of the cases. Table 1 gives an overview of the patient´s characteristics and the histology of the resected EBAC.
Resection rates
The en-bloc resection rate was 95.5 % (n = 21/22). Only in one patient the neoplastic lesion could not be resected in one piece and piecemeal resection was performed. The histologically proven R0 resection rate as well as the R0 en-bloc resection rate was 81.8 % (n = 18/22). In 4 patients (18.2 %) with histologically proven remaining tumor at the tumor margins (R1 resection), the tumor was incompletely resected at one of the lateral margins of the specimen in all 4 cases (100 %) and in 1 of the cases (25 %) the specimen showed additionally vertical tumor invasion down to the base of the resected specimen (see Table 2).
According to the above mentioned criteria, a curative resection for ESD in EBAC could be achieved in 77.3 % (n = 17/22).
The 4 patients with incomplete resected tumors (R1-resection) as well as one additional patient with a R0 resection but a deep (>1,000 µm) submucosal tumor invasion were sent to surgery. In these 5 patients, postoperative histology showed remaining tumors in only 3 patients, whereas in 2 patients no residual tumor could be detected. Lymph-node involvement was seen in 2 of the 5 operated patients.
Complications
The overall complication rate was 27.3 % (n = 6/22). Minor delayed bleeding occurred in 2 patients (9.1 %) and could be treated endoscopically without transfusion of red blood cells. A small perforation was observed in one patient (4.5 %) the day after the endoscopic tumor resection. An asymptomatic mediastinal emphysema was treated conservatively with antibiotics for 5 days. Three of the resected lesions (13.6 %) involved more than half of the esophageal circumference and developed symptomatic esophageal stenosis. These strictures were diagnosed 2–3 weeks after the initial procedure and required a sole balloon dilatation in one case, whereas recurrent balloon dilatations (7 resp. 21 dilatations) were necessary in two cases to eliminate the underlying dysphagia (see Table 2).
Follow-up
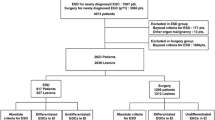
All 17 patients with a curative tumor resection underwent follow-up examinations including routine biopsies for a medium of 1.6 years (range 1 month–4.5 years). In these patients, local tumor recurrence occurred in only one patient (5.9 %). All other patients (94.1 %) remained tumor free during the follow-up period (see Table 2). After a 12 month follow-up, the patient with the described local tumor recurrence showed multifocal high-grade dysplasia in his remaining Barrett´s esophagus and was therefore sent to surgery. Complete histopathological workup after esophagectomy revealed a small mucosal adenocarcinoma. However, this patient was considered as local tumor recurrence as it was not possible to differentiate between a metachronous tumor lesion and a local tumor recurrence. Figure 2 gives an overview of the clinical results and the follow-up data in the 22 patients with EBAC treated by ESD.

Flow chart showing clinical results and follow-up data. R0, histologically confirmed complete resection with tumor-free margins (lateral and vertical); R1, histologically confirmed incomplete resection with tumor-infiltrated margins (lateral and/or vertical); CR complete remission
Discussion
ESD is a newly developed endoscopic technique and has been proven to be safe and effective for the en-bloc resection of superficial neoplasms in the whole gastrointestinal tract and especially in the esophagus and stomach [9, 11, 17]. In contrast to EMR, ESD allows an en-bloc resection for lesions greater than 2 cm and enables a complete histological workup of the resected specimen, including complete evaluation of the lateral and vertical resection margins according to oncological guidelines [12, 13].
In Asia, Barrett´s esophagus and Barrett´s adenocarcinoma (EBAC) are less frequent compared to the Western world, and therefore, limited data are available on ESD in EBAC. Up to now, EMR or radical surgical esophageal resection is the standard treatment in early, especially, mucosal EBAC leading to a comparable rate of curative resections and a similar 5-year survival rate [7]. On the other hand, better results were shown in several studies for ESD compared to EMR concerning the en-bloc, R0, and curative resection rates in esophageal squamous cell carcinomas and gastric adenocarcinomas [11–14].
In our study, ESD was technically feasible in every of the 22 cases with histologically proven EBAC. The en-bloc resection rate was 95.5 %. Complete tumor resections (R0 resections) could be achieved in 81.8 %. The curative resection rate was 77.3 %. In comparison to recent Japanese studies [15, 18], our data show comparable en-bloc, R0, and curative resection rates (see Table 3). In another recent European study [16] with a similar number of patients treated with ESD in early Barrett´s neoplasia, the R0 resection rate is lower compared to our study. In this study, most of the incomplete resections are caused by tumor growth at one of the lateral margins of the resected specimen [16]. This may be caused by a smaller size of the resected specimen compared to our and the other Japanese studies (see Table 3) [15, 16, 18]. A smaller size of the resected specimen can lead to insufficient safety margins especially in cases of subsquamous tumor growth which could be observed frequently in patients with Barrett´s neoplasia [19]. Figure 3 shows an example of such a histologically confirmed subsquamous extension of EBAC underneath the adjacent regular squamous esophageal epithelium which could already be supposed by high-resolution endoscopy in combination with Narrow-band imaging (NBI). Therefore, prior to endoscopic resection of EBAC we recommend a very detailed exploration of the neoplastic area and safety margins of at least 10 mm distance from the visible lesion.

Tumor growth of EBAC underneath the adjacent regular squamous esophageal epithelium. A High-resolution endoscopy. B Narrow-band imaging (NBI). C Histological confirmation of Barrett´s adenocarcinoma underneath squamous esophageal epithelium (HE staining, magnification ×100)
The major complication of ESD is perforation of the gastrointestinal wall which is reported in Japanese and European series in 0–20 % [15, 17, 18, 20–25]. In our study, one perforation occurred (5.9 %) which could be managed conservatively. Minor delayed bleeding was observed in 2 patients (9.1 %) and was managed endoscopically by clipping or by coagulation with a coagulation forceps without any need for transfusion of red blood cells. Recipi et al. and Fujishiro et al. reported minor bleeding in all of the performed ESDs [22, 23]. However, in contrast to delayed bleeding requiring endoscopic re-intervention, in our opinion minor bleeding during ESD cannot be considered as complication of the procedure.
In three of our patients (13.6 %), esophageal stenosis occurred. In all three patients, circumferential resection of the underlying EBAC was performed. This corresponds to other published studies [15, 17, 18, 20–25]. Ono et al. reported a stenosis rate of 2 % after the resection of lesions less than half of the circumference of the esophageal lumen. For resections of 75 % of the esophageal circumference, the stenosis rate rises up to 20 %. If the resection area involves more than 75 % of the esophageal circumference, the risk of stenosis increases up to 90 % [20].
After a mean follow-up of 1.6 years, local tumor recurrence occurred in the present study in only one patient (5.9 %) after a curative ESD of EBAC. In this case, it was not possible to differentiate between metachronous neoplastic lesions after a 12 month follow-up period and local tumor recurrence. Nevertheless, this patient was considered as local tumor recurrence. Our result with a low recurrence rate is in line with other studies [16, 18, 22, 24]. In fact, Hirasawa et al. and Ishii et al. observed no local or distant recurrences after curative resections of esophageal carcinomas after a follow-up period of 19 months [18, 21].
In summary, despite the small number of patients and the relatively short follow-up period, our study shows the value of ESD, especially in case of curative R0 resections, in the definite as well as less invasive endoscopic therapy of EBAC. In our opinion, special attention should be drawn toward undermining tumor growth of EBAC leading to a sufficient safety margin as the most important factor for a complete tumor resection with tumor-free lateral resection margins. However, due to the required learning curve and the management of potential complications, ESD especially in cases of EBAC should be restricted to greater endoscopic centers.
References
Pohl H, Welch HG (2005) The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst 97:142–146
Gaddam S, Singh M, Balasubramanian G, Thota P, Gupta N, Wani S, Higbee AD, Mathur SC, Horwhat JD, Rastogi A, Young PE, Cash BD, Bansal A, Vargo JJ, Falk GW, Lieberman DA, Sampliner RE, Sharma P (2013) Persistence of nondysplastic Barrett’s esophagus identifies patients at lower risk for esophageal adenocarcinoma: results from a large multicenter cohort. Gastroenterology 145:548–553
Sharma P (2009) Clinical practice. Barrett’s esophagus. N Engl J Med 361:2548–2556
Peitz U, Malfertheiner P (2007) Barrett carcinoma: diagnosis, screening, surveillance, endoscopic treatment, prevention. Z Gastroenterol 45(12):1264–1272
Sharma P, Falk GW, Weston AP, Reker D, Johnston M, Sampliner RE (2006) Dysplasia and cancer in a large multicenter cohort of patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 4(5):566–572
Kubo A, Corley DA, Jensen CD, Kaur R (2010) Dietary factors and the risks of oesophageal adenocarcinoma and Barrett’s oesophagus. Nutr Res Rev 23(2):230–246
Pech O, Bollschweiler E, Manner H, Leers J, Ell C, Hölscher H (2011) Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett´s esophagus at two high-volume centers. Ann Surg 254:67–72
Probst A, Golder D, Arnholdt H, Messmann H (2009) Endoscopic submucosal dissection of early cancers, flat adenomas, and submucosal tumors in the gastrointestinal tract. Clin Gastroenterol Hepatol 7(2):149–155
Wang KK, Prasad G, Tian J (2010) Endoscopic mucosal resection and endoscopic submucosal dissection in esophageal and gastric cancers. Curr Opin Gastroenterol 26(5):453–458
Muto M, Manabe T, Ohtsu A, Yoshida S (2005) Local recurrence of squamous-cell carcinoma of the esophagus. Gastrointest Endosc 61:219–225
Ortiz-Fernández-Sordo J, Parra-Blanco A, García-Varona A, Rodríguez-Peláez M, Madrigal-Hoyos E, Waxman I, Rodrigo L (2011) Endoscopic resection techniques and ablative therapies for Barrett’s neoplasia. World J Gastrointest Endosc 3(9):71–182
Ono S, Fujishiro M, Koike K (2012) Endoscopic submucosal dissection for superficial esophageal neoplasms. World J Gastrointest Endosc 4(5):162–166
Miyamoto S, Muto M, Hamamoto Y, Boku N, Ohtsu A, Baba S, Yoshida M, Ohkuwa M, Hosokawa K, Tajiri H, Yoshida S (2002) A new technique for endoscopic mucosal resection with an insulated-tip electrosurgical knife improves the completeness of resection of intramucosal gastric neoplasms. Gastrointest Endosc 55(4):576–581
Yamamoto HKH, Sunada K (2003) Successful en-bloc-resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small caliber-tip-transparent hood. Endoscopy 35:690–694
Höbel S, Baumbach R, Dautel P, Oldhafer KJ, Stang A, Feyerabend B, Yahagi N, Faiss S (2014) Single centre experience of endoscopic submucosal dissection (ESD) in premalignant and malignant gastrointestinal neoplasia. Z Gastroenterol 52:193–199
Toyonaga T, Man-i M, East JE, Nishino E, Ono W, Hirooka T, Ueda C, Iwata Y, Sugiyama T, Dozaiku T, Hirooka T, Fujita T, Inokuchi H, Azuma T (2013) 1,635 Endoscopic submucosal dissection cases in the esophagus, stomach, and colorectum: complication rates and long-term outcomes. Surg Endosc 27(3):1000–1008
Neuhaus H, Terheggen G, Rutz EM, Vieth M, Schumacher B (2012) Endoscopic submucosal dissection plus radiofrequency ablation of neoplastic Barrett’s esophagus. Endoscopy 44:1105–1113
Asano M (2012) Endoscopic submucosal dissection and surgical treatment for gastrointestinal cancer. World J Gastrointest Endosc 4(10):438–447
Hirasawa K, Kokawa A, Oka H, Yahara S, Sasaki T, Nozawa A, Tanaka K (2010) Superficial adenocarcinoma of the esophagogastric junction: long-term results of endoscopic submucosal dissection. Gastrointest Endosc 72(5):960–966
Anders M, Lucks Y, El-Masry MA, Quaas A, Rösch T, Schachschal G, Bähr C, Gauger U, Sauter G, Izbicki JR, Marx AH (2014) Subsquamous extension of intestinal metaplasia is detected in 98% of cases of neoplastic Barrett’s esophagus. Clin Gastroenterol Hepatol 12(3):405–410
Ono S, Fujishiro M, Niimi K, Goto O, Kodashima S, Yamamichi N, Omata M (2009) Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc 70(5):860–866
Ishii N, Horiki N, Itoh T, Uemura M, Maruyama M, Suzuki S, Uchida S, Izuka Y, Fukuda K, Fujita Y (2010) Endoscopic submucosal dissection with a combination of small-caliber-tip transparent hood and flex knife is a safe and effective treatment for superficial esophageal neoplasias. Surg Endosc 24(2):335–342
Repici A, Hassan C, Carlino A, Pagano N, Zullo A, Rando G, Strangio G, Romeo F, Nicita R, Rosati R, Malesci A (2010) Endoscopic submucosal dissection in patients with early esophageal squamous cell carcinoma: results from a prospective Western series. Gastrointest Endosc 71(4):715–721
Fujishiro M, Yahagi N, Kakushima N, Kodashima S, Muraki Y, Ono S, Yamamichi N, Tateishi A, Shimizu Y, Oka M, Ogura K, Kawabe T, Ichinose M, Omata M (2006) Endoscopic submucosal dissection of esophageal squamous cell neoplasms. Clin Gastroenterol Hepatol 4(6):688–694
Fujishiro M, Kodashima S (2009) Indications, techniques, and outcomes of endoscopic submucosal dissection for esophageal squamous cell carcinoma. Esophagus 6(3):143–148
Disclosure
Dr. P. Dautel, Dr. R. Baumbach, Dr. S. Faiss became speaker honoraria from Olympus Deutschland GmbH (Hamburg, Deutschland). Dr. N. Yahagi became speaker honoraria and honoraria for consultantship from Olympus (Tokyo, Japan). Dr. S. Höbel, Dr. K.-J. Oldhafer, Dr. A. Stang, Dr. B. Feyerabend, Dr. C. Schrader have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Höbel, S., Dautel, P., Baumbach, R. et al. Single center experience of endoscopic submucosal dissection (ESD) in early Barrett´s adenocarcinoma. Surg Endosc 29, 1591–1597 (2015). https://doi.org/10.1007/s00464-014-3847-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3847-5