
Abstract
Background
Gaze training is an effective way of training basic laparoscopic skills, resulting in faster acquisition periods and more robust subsequent performance under pressure. The current study is a randomized control trial which examines whether the performance benefits of gaze training stand the test of time (delayed retention) and transfer to more complex skills.
Methods
Thirty-six medical students were trained to proficiency (50 trials) on a one-handed laparoscopic task (picking and dropping balls) in either a discovery learning (DL) or gaze training (GT) group. Both groups performed the one-handed task in baseline, retention and delayed retention (1 month) tests. They also performed baseline, retention and delayed retention tests of a two-handed task (grasping and cutting). Performance (completion time) and gaze control (target locking) were assessed throughout.
Results
For the one-handed task, the GT group displayed superior performance at retention (p < .001), underpinned by more expert-like gaze control (p < .05). The GT group also displayed superior performance in the one-handed task at delayed retention (p < .005), underpinned by more expert-like gaze control strategies (p < .001). Although the DL group’s performance fell to 84 % of performance at retention, the GT group maintained performance at 100 % of retention. There were no differences between the groups for the two-handed task at retention (p = .140); however, at delayed retention, the GT group outperformed the DL group (p < .005) and displayed more expert-like gaze control (p < .001).
Conclusions
Novices trained to adopt an expert-like gaze control strategy were able to attain higher levels of performance more quickly than novices who learned by discovery alone. Furthermore, these skills were more durable over time and were transferable to more complex skills. Gaze training is a beneficial intervention to aid the acquisition of the basic motor skills required for laparoscopy.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
When acquiring laparoscopic techniques, the novice surgeon must overcome environmental constraints on visuomotor control, such as loss of depth perception, poor tactile feedback, and the use of long instruments that amplify movement error and exhibit a fulcrum effect [1, 2]. Recent research has revealed differences in the gaze control strategies of experienced and novice laparoscopic surgeons [3, 4]. Novices, who are still developing the sensory-motor mapping rules for laparoscopy, use visual feedback to check on the effect of their movements, and so exhibit a gaze strategy that switches between tracking their tool movements and fixating the target to be manipulated (a switching strategy) [3, 5]. Experienced surgeons, who have developed the necessary sensory-motor mapping rules, primarily fixate the target without the need to check their tool locations (a target-locking strategy) [3, 4]. This more efficient gaze control strategy has been shown to underpin superior laparoscopic performance: Not only in cross sectional comparisons between experts and novices, but also in training studies. Novices taught to model expert-like gaze strategies acquired laparoscopic skills more quickly than counterparts taught to model expert-like tool movements or to learn by discovery (no instructions) [6, 7].
If training programs are to have clinical utility, they must demonstrate that they transfer to the operating room, where stressors such as multitasking, evaluation threat and time pressure compete for limited attentional demands [8, 9]. The limited research to date that has examined the effectiveness of gaze training has shown that it provides benefits in terms of resilience to such stress, compared to more traditional approaches [6, 7]. It has been proposed that the focus on controlling only one component of the skill—accurate gaze—reduces the attentional demands for novices, allowing them to learn the skill more quickly and have resources available to deal with stressful scenarios [6, 7, 10–12]. However, two other important criteria for effective training are the degree to which learning remains stable beyond the training period (retention), and the degree to which the skills learned actually translate to more complex skills (transfer) [1, 13, 14].
First, as performance is influenced by various temporary factors including feedback, motivation, boredom and fatigue, it is important to ensure that the performance changes assessed after training are relatively permanent [15, 16]. Research into the long-term effect of laparoscopic training has shown varying degrees of skill maintenance and deterioration between 1 week and 6 months after training, dependent on the complexity of the skill being performed [13, 17]. Delayed retention tests are designed to allow a certain time interval to elapse after training and are therefore more reliable in detecting permanent changes in skill acquisition [16]. Second, the utility of any basic technical skills training program is also dependent on the degree to which learning transfers to tasks representative of the OR. Transfer tests assess performance using a more complex or representative task than the practised one [14, 18].
The aim of this study is to further establish the clinical utility of gaze training as a means to develop the basic technical skills required in laparoscopic surgery. Although previous research has established benefits in terms of expedited skill acquisition and robustness under pressure [6, 7], the current study seeks to test if gaze training stands the test of time (via a delayed retention test) and transfers to a more complex task. We derived the following hypotheses in relation to the expected benefits of gaze training compared to an appropriate control.
In the baseline condition, there will be no differences in performance between gaze-trained (GT) and discovery learning (DL; control) groups. Both groups will demonstrate novice-like performance and gaze control strategy (i.e., switching between tool and target).
FormalPara Hypothesis 2In line with previous research, the GT group will display superior performance and a more expert-like (target locking) gaze control strategy in both a retention and delayed retention test when compared to the DL group.
FormalPara Hypothesis 3The GT group will display superior performance and a more expert-like (target locking) gaze control strategy, in a two-handed transfer test when compared to the DL control group in both a retention and delayed retention test.
Methods
Participants
Thirty-six novice participants volunteered to take part in the study (18 men, 18 women; mean, 21.5 years; range, 18–40 years). Participants were medical students with no prior laparoscopic training, and were both left and right-hand dominant (5 left, 31 right). Institutional ethical approval was obtained before initiation of the study, and written informed consent was provided by all participants before commencement of testing. Participants were assigned to one of two treatment groups as discussed below. Previous research has revealed significant differences in performance under pressure between gaze training and discovery learning interventions with group sizes of 10 (t(19) = 4.86, p < .001, Cohen’s d = 2.17) [6]. We are therefore confident that the larger group sizes in the current study have sufficient power to show significant effects across delayed retention and transfer tasks.
Apparatus and task
Testing was performed on a 3-Dmed standard minimally invasive training system with joystick SimScope (3-Dmed, Franklin, OH), based at the University of Exeter, UK (Fig. 1). Participants were trained and tested on a ball pick and drop task from the 3-Dmed training tasks, which has been used in previous laparoscopy training research [2, 19]. To complete the task, participants were required to grasp six foam balls (approximately 5 mm diameter) positioned on stems, using a single instrument (with their dominant hand), and individually place them into a cup in a numbered sequence (Fig. 1). To test transfer of motor skills, a two-handed grasping and cutting task was devised. To complete the task, participants individually grasped six polypropylene filaments (length 60 mm) within a 5 mm grasping area marked in red using a grasping tool held in their nondominant hand, and cut each filament within a 5 mm cutting area marked in blue with a cutting tool held in their dominant hand (Fig. 2). Previous research has shown that similar two-handed grasping and clipping surgical tasks have been able to differentiate performance between novices and experts; have revealed appropriate construct validity and learning curve progression in novices; and emulate the technical precision required to clip and cut a cystic duct during a laparoscopic cholecystectomy [20, 21]. Participants were instructed to complete both tasks as quickly and as accurately as possible.

Testing setup showing the 3-Dmed laparoscopic trainer and the ball pick-and-drop task

Two-handed grasping and cutting task
Participants were fitted with an Applied Science Laboratories Mobile Eye gaze registration system (ASL, Bedford, MA), which uses dark pupil tracking to calculate gaze metrics [3, 4]. The system consists of lightweight headgear that incorporates two cameras; one that records the participant’s eye and the other the scene environment, and a trio of LEDs that project near-infrared (IR) light into the eye. The near-IR light is harmless and not visible to the wearer, though it is visible to the eye camera as a triangle of three dots reflected by the cornea. Visual gaze is computed using corneal reflection and the position of the center of the pupil, by comparing the vector between the pupil and cornea. Video streams from the two cameras are recorded at 30 Hz via a modified digital cassette recorder attached to a laptop installed with Eyevision (ASL) software [3, 4].
Training groups
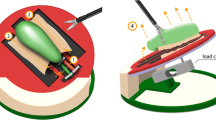
Participants were assigned to one of two training groups: gaze training (GT) and discovery learning (DL) adapted from previous gaze-training research [6, 7]. The GT group (n = 18) were shown a video of an expert’s gaze control during completion of the ball pick and drop task. Participants were then explicitly advised to implement a target-locking gaze control strategy, incorporating long and stable fixations on each target (ball or cup) with smooth shifts of gaze from one target to the next [6]. Additionally, the GT group performed the ball pick and drop task using surgery training template (STT) software, which overlays a template on top of the real-time video images received from the laparoscopic camera [7]. Target locations are preprogrammed on to the display, which are sequentially highlighted by making the rest of the screen darker (Fig. 3). By only highlighting the next target (i.e., the next ball in the sequence or the cup) before the participant initiates each grasp and drop attempt, participants are passively guided to adopt a target-locking gaze control strategy [6, 7].

Training template (STT) used by the gaze-trained group occludes the full field of view with a translucent mask, ensuring that only the next relevant target is highlighted: either the next ball to be picked up (A) or the cup in which the grasped ball is dropped (B)
The DL group (n = 18) did not use the STT template during task completion and were not directed to adopt a target locking strategy. The DL group were told to complete the task as quickly and accurately as possible, and had a normal, unrestricted view of the display monitor (Fig. 1) during the learning phase [6, 7]. Previous research has revealed that discovery learning provides a more effective learning environment than focusing on controlling tool movements, so was considered to be the most appropriate control comparison [6].
Procedure
Participants attended the laboratory individually, and were asked to read an information sheet indicating the study aims before providing written informed consent and completing a demographic questionnaire. The eye tracker was calibrated using a six-point chart on the display screen. All participants performed baseline (untrained) tests of both the ball pick and drop task and the two-handed grasping and cutting task under normal viewing conditions (i.e., without the STT). Participants were then randomly assigned to a treatment group, and received their specific instructions. During the learning phase, participants completed 50 trials of the ball pick and drop task only, resulting in 300 total ball pick-and-drop attempts. The acquisition period was divided into 10 blocks of five trials to provide sufficient rest periods between each block. Previous research has demonstrated 50 trials as the mean number required to attain proficiency levels on a task of similar difficulty [19].
The GT group completed the task with the highlighted viewing conditions provided by the STT software throughout the learning phase, while the DL group completed the task under normal viewing conditions. After the learning phase, participants performed retention tests of both ball pick and drop task and two-handed grasping and cutting task, under normal conditions (no instructions and no STT), in order to assess immediate learning. Participants returned to the laboratory 1 month after their original attendance (mean, 35.42 days; standard deviation, 10.19 days), having received no additional laparoscopic training or practice in the intervening period. The eye tracker was refitted and calibrated, and participants performed both the ball pick and drop, and the two-handed grasping and cutting task. One month was selected as a suitable delay period based on the findings of Stefanidis et al. [17], as it should provide sufficient time for some posttraining skill deterioration to have transpired and performance stabilisation to have occurred. At the end of the study, participants were thanked for their participation and debriefed.
Measures
Performance
Performance was evaluated in terms of task completion time, which has been shown to be a valid index in similar laparoscopic tasks [2–4, 6, 7, 19].
Gaze control
The eye tracker videos were manually analysed in a frame-by-frame manner (1 frame = 33.33 ms) by two experimenters using Quiet Eye Solutions software (QE Solutions Inc., Calgary, Canada). The location of the relevant target was defined for each of the tasks as the trial unfolded: In the single hand learning task, the targets were the current ball in sequence and the cup; and in the two-handed transfer task, the targets were the red grasping area and blue cutting area of the filaments in sequence. Fixations were defined as gaze that remained on one of these locations (within 1° visual angle) for a minimum of 99.99 ms (≥3 frames of video) [3, 4, 6, 7]. The duration of all fixations on the target location and tool location was calculated for each attempt, and a target-locking measure computed by subtracting the percentage of tool fixation time from the percentage of target fixation time [3, 4, 6, 7]. A full target-locking strategy will yield a positive score of over 50 %, while equal fixation durations on tool and target (a switching strategy) is reflected by a score closer to 0. A negative score reflects more time fixating the tools than the target.
Statistical analysis
Shapiro-Wilks tests revealed normal distribution of all data; therefore, parametric statistical analyses were adopted. For both the training and transfer task, main and interaction effects on performance (completion time) and gaze control measures were analysed with 2 (group; GT vs. DL) × 3 (condition; baseline vs. retention vs. delayed retention) mixed-design ANOVAs. Greenhouse-Geisser corrections to the degrees of freedom were applied where the assumption of sphericity was violated. Uncorrected degrees of freedom are reported along with the corrected probability values and the epsilon value. Significant effects were followed up with simple t tests to examine within and between group differences. Partial eta squared (η 2 p ) and Cohen’s d were used to calculate effect sizes for omnibus and simple comparisons, respectively.
Results
Ball pick and drop task
Performance: completion time
ANOVA showed a significant main effect for condition, F (2,68) = 53.67, p < .001, ε = .60, η 2 p = .61, and a main effect for group that was approaching significance, F (1,34) = 2.91, p = .097, η 2 p = .08. There was no significant interaction effect, F (2,68) = 1.00, p = .337, ε = .60, η 2 p = .03.
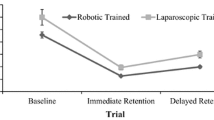
Between-group follow-up t tests revealed no differences between groups at baseline, t (34) = 0.24, p = .815, d = .08. However, the GT group performed significantly faster at retention, t (34) = 4.38, p < .001, d = 1.46, and delayed retention conditions, t (20.19) = 3.49, p < .005, d = 1.16. Although the deterioration in completion time between retention and delayed retention conditions approached significance for the DL group, t (17) = −2.01, p = .06, d = .53, this was not the case for the GT group, t (17) = −.31, p = .76, d = .09 who maintained their level of performance. The completion time data are presented in Fig. 4A.

A Mean (±standard error) completion time during the ball pick and drop task, for gaze training and discovery learning groups in the baseline, retention and delayed retention tests. B Mean (±standard error) target locking fixation scores during the ball pick and drop task, for gaze training and discovery learning groups in the baseline, retention and delayed retention tests
Gaze control
ANOVA showed a significant main effect for condition, F (2,60) = 56.73, p < .001, η 2 p = .65, and group, F (1,30) = 7.82, p < .05, η 2 p = .21. The interaction effect approached significance, F (2, 60) = 2.62, p = .081, η 2 p = .08. Between-group follow-up t tests revealed no differences between groups at baseline, t (32) = −0.66, p = .52, d = .22. However, the GT group revealed significantly higher target locking than the DL group at both retention, t (33) = −2.21, p < .05, d = .75, and delayed retention, t (32) = −4.46, p < .001, d = 1.53. Within-group follow-up tests revealed no deterioration in target-locking between retention and delayed retention conditions for either the DL, t (15) = 1.23, p = .239, d = .45, or GT group, t (16) = −0.09, p = .93, d = .02. The gaze control data are presented in Fig. 4B.
Due to an eye tracker malfunction, gaze data could not be coded for some of the participants. For the one-handed ball pick and drop task, data for two participants from each group could not be coded. For the two-handed grasping and cutting task, data for two participants from the discovery learning group and three participants from the gaze trained group could not be coded.
Two-handed grasping and cutting task
Performance: completion time
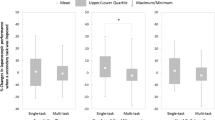
ANOVA showed a significant main effect for condition F (2,68) = 75.34, p < .001, η 2 p = .69, group, F (1,34) = 5.83, p < .05, η 2 p = .15, and a significant interaction effect, F (2,68) = 8.18, p < .005, η 2 p = .19. Between-group follow-up t tests revealed no differences between groups at baseline, t (34) = −0.10, p = .92, d = .03, or at retention t (34) = 1.51, p = .140, d = .50. The GT group performed significantly faster at delayed retention, t (34) = 3.84, p < .005, d = 1.29. Within-group follow-up t tests revealed significant improvements in completion time between baseline and retention for both the DL group, t (17) = 7.66, p < .001, d = 2.07, and GT group, t (17) = 10.32, p < .001, d = 2.92. There was a significant deterioration in completion time between retention and delayed retention conditions for the DL group, t (17) = −3.90, p < .001, d = .92, but not the GT group, t (17) = 0.00, p = .50, d = .00. The completion time data are presented in Fig. 5A.

A Mean (±standard error) completion time (during the two-handed grasping and cutting task, for gaze training and discovery learning groups in the baseline, retention and delayed retention tests. B Mean (±standard error) target locking fixation score during the two-handed grasping and cutting task, for gaze training and discovery learning groups in the baseline, retention and delayed retention tests
Gaze control
ANOVA showed a significant main effect for condition F (2,58) = 13.57, p < .001, η 2 p = .32, group, F (1,29) = 22.30, p < .001, ε = .83, η 2 p = .44, and a significant interaction effect, F (2,58) = 11.07, p < .001, ε = .83, η 2 p = .28. Between-group follow-up t tests revealed no differences between groups at baseline, t (31) = −0.33, p = .75, d = .11. However, the GT group had significantly higher target-locking scores at retention, t (33) = −3.85, p < .001, d = 1.30, and delayed retention conditions, t (31) = −6.51, p < .001, d = 1.88. Within-group follow-up t tests revealed a significant improvement in target-locking between baseline and retention for the GT group, t (16) = −8.31, p < .001, d = 1.49, but not the DL group, t (15) = −0.94, p = .18, d = .22. There was no deterioration in target-locking between retention and delayed retention conditions for the DL group, t (16) = 0.89, p = .19, d = .33, or the GT group, t (14) = −1.24, p = .12, d = .28. The gaze control data are presented in Fig. 5B.
Discussion
Gaze training has recently begun to establish its efficacy in accelerating laparoscopic technical skill acquisition during the early learning curve phase [6, 7]. The purpose of this study was to explore the utility of a gaze-focused intervention on the learning of new psychomotor skills via simulation. Furthering previous research investigating the effects of gaze training on novices’ performance [6, 7] this study assessed their ability to learn via tests of transferability, and delayed retention. Importantly, the findings from the baseline condition imply that consequent differences between groups in the postacquisition testing phase can be attributed to the training protocols administered. In support of hypothesis 1, both groups displayed similar, slow completion times and switching gaze control strategies in the baseline condition. Specifically, completion times were approximately 80 and 250 s for the pick and drop task (Fig. 4A) and the grasp and cut task (Fig. 5A), respectively. Target locking percentages were approximately 0 and 18 % for the pick and drop task (Fig. 4B) and the grasp and cut task (Fig. 5B), respectively.
One-handed pick and drop (training) task
Hypothesis 2 predicted that the GT group would exhibit superior performance over the DL group in the pick and drop task, in both the retention and delayed retention conditions, with expert-like gaze control underpinning the performance advantage. The results support the hypothesis; in the retention condition the GT group performed 9 s faster (28 %) on average (Fig. 4A) and displayed a 33 % higher target-locking score (Fig. 4B) than the DL group. The findings therefore support previous literature promoting the importance of expert gaze control strategy in the acquisition of basic laparoscopic skills [6, 7]. Interestingly, the DL group increased their target-locking score by 56 % (compared with 72 % in the GT group) from baseline, which shows that learning through experience alone results in the development of more expert-like gaze control [22]. However, by explicitly training novices to model the gaze control of experienced surgeons, this process can be expedited [7].
In the delayed retention condition, the GT group performed 16 s faster (49 %) on average than the DL group after a 1-month break (Fig. 4A), with a superior target-locking score underpinning their performance advantage (72 vs. 35 %; Fig. 4B). This target locking score displayed by the GT group is closer to that of experienced laparoscopic surgeons, and suggests that these trainees are further along the learning curve [3, 4]. Furthermore, the GT group maintained stable performance and gaze control between the retention and delayed retention conditions, whereas the DL group’s performance significantly deteriorated after 1 month of no practice (Fig. 4A). Previous research has demonstrated varying levels of laparoscopic skill maintenance (75–90 %); depending on task complexity, training duration, and delay period [17, 23]. In the current study, the GT group’s performance at delayed retention was maintained at 100 % of retention levels, whereas the DL group’s performance dropped to 84 % of retention levels.
Two-handed grasp and cut (transfer) task
Hypothesis 3 predicted that the GT group would exhibit superior performance and gaze control on a two-handed transfer test than the DL group, despite both groups exclusively learning on a simpler one-handed task. Generalisation of skills is a vital component of training during the early learning curve phase if video box trainers are to be beneficial for laparoscopic training curricula [14, 20, 21, 24, 25]. Both the GT and DL groups improved their completion time in the transfer task from baseline to retention by 46 and 38 %, respectively (Fig. 5A), although the difference between the groups at retention approached significance (p = 0.07). The gaze control results show that the GT group was able to significantly increase target-locking by 44 %, compared with the DL group who made no significant increase in target-locking (Fig. 5B). Unlike with the one-handed trained task, target locking did not increase in a concomitant fashion with performance for the DL group in the transfer task. This effect is likely because the task itself was not trained, but generic visuomotor control skills important for working in the laparoscopic environment were improved.
At 1 months delayed retention, the GT group displayed significantly better performance and gaze control in the transfer task than their DL group counterparts. They performed approximately 69 s faster on average (Fig. 5A) underpinned by a 52 % higher target-locking score (Fig. 5B). The GT group’s performance at delayed retention was maintained at 100 % of retention levels, whereas the DL group’s performance decreased by 33 % of retention levels. This finding suggests that delayed transfer (more so than delayed replication of a trained skill) is especially disrupted for trainees left to learn by discovery; even if the time period is only 1 month. However, the performance of the GT group in either the trained or transfer task, was unaffected by this delay.
Why is gaze training superior?
Previous research investigating the efficacy of gaze training for novices acquiring basic psychomotor skills in laparoscopic surgery [6, 7] and sport [10–12], has revealed a performance advantage for gaze training that is revealed in both how quickly the skill is acquired and in how resilient the skill is to the demands of various stressors (e.g., multitasking, time pressure, evaluation threat). The current study extends this advantage to the transfer of the skill to novel, more complex tasks and the durability/robustness of the skill over time. However, the big question is how does such training achieve these impressive results that are important for skill acquisition in domains where basic skills need to be learned quickly; performed under pressure; translated to more complex tasks—and often at a date that is distant from when the skill was trained? The explanation for this advantage is multifaceted and can be explained in terms of theories of visuomotor control and skill acquisition.
First, by modelling the strategic gaze control and hence visuomotor control strategies of experts, novices are able to cheat the learning process; where such a strategy is typically developed over time through trial and error and continual practice [22]. Proficiency in a motor task is reached when effective gaze control provides the required target-related information at the right time to be used by the central nervous system to control movement [26]. By adopting this strategy earlier in learning, gaze trained novices are able to make use of more optimal and efficient visuomotor strategies. The results of the current study suggest that the gaze control strategy of target locking is transferable from one skill to other similar skills. Second, it appears that a strategy of modelling gaze is more effective than modelling other important components of the task (e.g., limb movements) because it reduces the attentional demands of the control process. Controlling a single facet of the skill (gaze position) is much less attentionally demanding than trying to control the multiple degrees of freedom inherent in the relevant effectors (e.g., multiple joints, coactivating muscles). The fact that gaze trained surgical novices are able to multitask more effectively than novices trained to focus on their hand movement, or learn via discovery, supports such an attentional capacity explanation [6].
Conclusions
To conclude, the current study revealed that novice surgeons trained to implement an expert-like gaze control strategy were able to transfer laparoscopic psychomotor skills over to a more complex and realistic task, thus climbing the learning curve to laparoscopic proficiency in less time than novices who learn by discovery alone. The findings suggest that gaze-trained novices have additional spare attentional resources allowing them to perform better at a complex task and maintain this performance even after a period of no practice. Bench model video box trainers can facilitate the learning of optimal gaze control and subsequent technical proficiency, when supported with relevant (target locking) instructions and passive guidance via integrated software. The clinical utility of these devices and techniques should permit their inclusion within formal surgical training curricula, and could potentially be useful in reducing the time and cost of surgical training.
References
Gallagher AG, McClure N, McGuigan J, Crothers I, Browning J (1999) Virtual reality training in laparoscopic surgery: a preliminary assessment of minimally invasive surgical trainer virtual reality (MIST VR). Endoscopy 31:310–313
Scott DJ, Bergen PC, Rege RV, Laycock R, Tesfay ST, Valentine RJ, Euhus DM, Jeyarajah DR, Thompson WM, Jones DB (2000) Laparoscopic training on bench models: better and more cost effective than operating room experience? J Am Coll Surg 191:272–283
Wilson M, McGrath J, Vine S, Brewer J, Defriend D, Masters R (2010) Psychomotor control in a virtual laparoscopic surgery training environment: gaze control parameters differentiate novices from experts. Surg Endosc 24:2458–2464
Wilson MR, McGrath JS, Vine SJ, Brewer J, Defriend D, Masters RS (2011) Perceptual impairment and psychomotor control in virtual laparoscopic surgery. Surg Endosc 25:2268–2274
Law B, Atkins MS, Kirkpatrick AE, Lomax AJ, Mackenzie CL (2004) Eye gaze patterns differentiate novice and experts in a virtual laparoscopic surgery training environment. In: Duchowski AT, Vertegaal R (eds) Proceedings of the eye tracking research and application symposium, San Antonio, TX, March 22–24, 2004, pp 41–47
Wilson MR, Vine SJ, Bright E, Masters RS, Defriend D, McGrath JS (2011) Gaze training enhances laparoscopic technical skill acquisition and multi-tasking performance: a randomised, controlled study. Surg Endosc 25(12):3731–3739
Vine SJ, Masters RS, McGrath JS, Bright E, Wilson MR (2012) Cheating experience: guiding novices to adopt the gaze strategies of experts expedites the learning of technical laparoscopic skills. Surgery 152:32–40
Goddell KH, Cao CG, Schwaitzberg SD (2006) Effects of cognitive distraction on performance of laparoscopic surgical tasks. J Laparoendosc Adv Surg Tech 16:94–98
Poolton JM, Wilson MR, Malhotra N, Ngo K, Masters RS (2011) A comparison of evaluation, time pressure and multi-tasking as stressors of psychomotor surgical performance. Surgery 149(6):776–782
Vine SJ, Wilson MR (2010) Quiet eye training: effects on learning and performance under pressure. J Appl Sport Psychol 22:361–376
Vine SJ, Wilson MR (2011) The influence of quiet eye training and pressure on attentional control in a visuo-motor task. Acta Psychol 136:340–346
Vine SJ, Moore LJ, Wilson MR (2011) Quiet eye training facilitates competitive putting performance in elite golfers. Front Psychol 2:8
Grober ED, Hamstra SJ, Wanzel KR, Reznick RK, Matsumoto ED, Sidhu RS, Jarvi KA (2004) Laboratory based training in urological microsurgery with bench model simulators: a randomized controlled trial evaluating the durability of technical skill. J Urol 172:378–381
Gallagher AG, Ritter EM, Champion H, Higgins G, Fried MP, Moses G, Smith CD, Satava RM (2005) Virtual reality simulation for the operating room: proficiency-based training as a paradigm shift in surgical skills training. Ann Surg 241:364–372
Wulf G, Shea C, Lewthwaite R (2010) Motor skill learning and performance: a review of influential factors. Med Educ 44:75–84
Arthur W Jr, Bennet W Jr, Stanush PL, McNelly TL (1998) Factors that influence skill decay and retention: a quantitative review and analysis. Hum Perform 11:57–101
Stefanidis D, Korndoffer JR Jr, Markley S, Sierra R, Scott DJ (2006) Proficiency maintenance: impact of ongoing simulator training on laparoscopic skill retention. J Am Coll Surg 202:599–603
Grantcharov TP, Kristiansen VB, Bendix J, Bardram L, Rosenberg J, Funch-Jensen P (2004) Randomized clinical trial of virtual reality simulation for laparoscopic skills training. Br J Surg 91:146–150
Ritter EM, Scott DS (2007) Design of a proficiency-based skills training curriculum for the fundamentals of laparoscopic surgery. Surg Innov 14:107–112
Aggarwal R, Grantcharov TP, Eriksen JR, Blirup D, Kristiansen VB, Funch-Jensen P, Darzi A (2006) An evidence-based virtual reality training program for novice laparoscopic surgeons. Ann Surg 244:310–314
Aggarwal R, Crochet A, Dias A, Misra A, Ziprin P, Darzi A (2009) Development of a virtual reality training curriculum for laparoscopic cholecystectomy. Br J Surg 96:1086–1093
Salier U, Flanagan JR, Johansson RS (2005) Eye–hand coordination during learning of a novel visuomotor task. J Neurosci 205:8833–8842
Torkington J, Smith SG, Rees B, Darzi A (2001) The role of the basic surgical skills course in the acquisition and retention of laparoscopic skill. Surg Endosc 15:1071–1075
Gurusamy K, Agarwal R, Palanivelu L, Davidson BR (2009) Systematic review of randomized controlled trials on the effectiveness of virtual reality training for laparoscopic surgery. Br J Surg 96:1087–1093
Boehler ML, Schwind CJ, Rogers DA, Ketchum J, O’Sullivan E, Mayforth R, Quin J, Wohltman C, Johnson C, Williams RG, Dunnington G (2007) A theory-based curriculum for enhancing surgical skillfulness. J Am Coll Surg 205:492–497
Land MF (2009) Vision, eye movements, and natural behavior. Vis Neurosci 26:51–62
Acknowledgments
The authors would like to acknowledge Roy Chandra-Ramanan for his support in data collection, and Chenghua Lin for developing the STT software. This work was supported by a bilateral research grant from the Economic and Social Research Council, UK and the Research Grants Council, Hong Kong (RES-000-22-3016).
Disclosures
Dr. Vine, Mr. Chaytor, Mr. McGrath, Prof. Masters, and Dr. Wilson have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vine, S.J., Chaytor, R.J., McGrath, J.S. et al. Gaze training improves the retention and transfer of laparoscopic technical skills in novices. Surg Endosc 27, 3205–3213 (2013). https://doi.org/10.1007/s00464-013-2893-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-2893-8