
Abstract
Purpose
This study aimed to compare variations between the earlobe and fingertip sampling sites in exercises dominated by upper body muscle exertion. It also sought to investigate capillary blood lactate differences between Lactate Scout 4 (LS4) and a bench-top analyzer (Biosen S-Line analyzer, BSL) during Double Poling.
Methods
Blood samples were collected from the earlobe and fingertip immediately before exercise, at the end of each of five stages, and at 1-, 3-, 5-, and 7-min post-exercise. Forty healthy university students participated as volunteers. During the study, they performed double poling on a ski ergometer with progressively increasing load. Lactate levels were measured using both the BSL and LS4 analyzers.
Results
Fingertip Bla values were significantly higher than earlobe values, with a mean bias of −0.66 mmol/L, reaching −0.86 mmol/L in the 4–8 mmol/L range. At the earlobe, the highest CCC between BSL and LS4-a was 0.84 (> 8 mmol/L), and for BSL and LS4-b, it was 0.85 (> 8 mmol/L). At the fingertip, the highest CCC between BSL and LS4-c was 0.68 (> 8 mmol/L), and for BSL and LS4-d, it was 0.52 (> 8 mmol/L). Comparing LS4-a and LS4-b at the earlobe, the highest CCC was 0.83 (0–4 mmol/L). At the fingertip, comparing LS4-c and LS4-d, the highest CCC was 0.68 (> 8 mmol/L).
Conclusions
Blood lactate concentrations are higher at the fingertip than the earlobe during SkiErg double poling. The LS4 is less reliable, especially at the fingertip, so using the earlobe with the BSL analyzer is recommended for accurate measurements.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The level of lactate in the blood (Bla) provides an indication of the balance between the production and clearance of this byproduct of anaerobic metabolism (Brooks 1986; Poole et al. 2021). Accordingly, Bla is widely utilized to evaluate an athlete’s anaerobic threshold, exercise intensity, degree of fatigue, and post-exercise recovery (Faude et al. 2009; Ghosh 2004). Since these factors play key roles in planning personal training in a manner that enhances performance optimally, determination of Bla must be as accurate as possible (Crotty et al. 2021; Tanner et al. 2010).
Quantification of Bla is influenced by whether the blood analyzed is from an artery, vein, or capillary (Foxdal et al. 1990; Yoshida et al. 1982). For instance, Bla in arterial blood from the arms is significantly higher than that in venous blood from these same limbs during exercise dominated by leg movements, such as cycling and running (El-Sayed et al. 1993; Robergs et al. 1990). In the case of sampling from arteries and veins, a catheter must be inserted into the brachial vein or artery of the arms or femoral artery of the legs (Williams et al. 1992), which is not recommendable in connection with training practice due to the invasiveness, discomfort, and difficulty associated with this procedure (Dassonville et al. 1998; Feliu et al. 1999). On the other hand, sampling of capillary blood from the earlobe, fingertip, or toe requires no more than 20 μL of blood, involves only slight discomfort (puncture with a lancet), and is easy to perform and is, consequently, widely utilized (Forsyth and Farrally 2000). However, the accuracy of capillary blood measurements can be compromised if improper handling allows sweat, which contains lactate, to contaminate the sample (Sakharov et al. 2010).
The Bla difference between the earlobe, fingertip, and toe may vary depending on the exercise mode (Dassonville et al. 1998). During cycling, running and rock climbing, where force is generated primarily by the leg muscles, the Bla in capillary blood collected from the fingertip was significantly higher than in samples from the earlobe (Draper et al. 2006; Feliu et al. 1999; Yamagata et al. 2018). However, some reports have disagreed with this conclusion and, moreover, it remains unclear whether the Bla in earlobe and fingertip capillary blood differ or not when the arm muscles are primarily involved in exercise (Forsyth and Farrally 2000; Moran et al. 2012).
Assessment of Bla employing different testing principles and operating modes, as well as in different situations, can vary significantly (Mc Naughton et al. 2002). In this context, measurement with bench-top analyzers in the laboratory is generally considered the gold standard (van Someren et al. 2005), but usage of such devices outdoors can be complicated by factors such as limited portability, the requirement for a continuous power supply, and longer testing procedures which may preclude obtaining results in real-time (Baldari et al. 2009; Stewart and Stavrianeas 2008).
Consequently, portable, battery-operated lactate analyzers, such as those in the Lactate Scout series (LS + : EKF diagnostic GmbH, Barleben, Germany), are widely used in the field of sports for rapid acquisition of Bla during training and testing. The earlier versions of the LS have already been shown to be highly reliable, particularly in animal experiments (Belic et al. 2016; Ferasin et al. 2007; Kaynar et al. 2015); whereas LS4, the latest version released in 2019, has not yet undergone a comprehensive evaluation to show its reliability and accuracy, perhaps even more so than the earlier versions in connection with sports testing (Bonaventura et al. 2015; Tanner et al. 2010).
Double Poling, one of the primary techniques used in cross-country skiing, engages the muscles of the upper body and core (Stöggl and Holmberg 2011). The dependency on coordinated exertion of the upper limbs and core muscles renders Double Poling an ideal scenario for investigating differences in capillary Bla between the earlobe and fingertip in exercises predominantly involving upper body strength. Double Poling is an important metric for assessing athletes’ performance and training outcomes (Holmberg et al. 2005), while the Bla serving as a commonly used and significant physiological indicator to evaluate athletes’ responses to such loads. In this type of exercise modality, current research on the differences in lactate concentrations between the earlobe and fingertip as sampling sites is insufficient, underscoring the need for further investigation.
This study aims to address these gaps by investigating how different lactate concentrations from earlobe and fingertip sites are based on BSL analysis of capillary blood, comparing the LS4 measures of blood lactate concentration with those obtained using BSL analysis from the same site, and assessing the variability of LS4 repeated measures of blood lactate concentration at earlobe and fingertip sites. Our hypotheses are that the portable LS4 analyzer measures lactate levels reliably and accurately, and that significant differences exist between measurements taken from the earlobe and fingertip.
Methods
Subjects
The 23 male and 17 female volunteers who participated (23.0 ± 1.8 years of age, 1.71 ± 9.83 cm tall, weighing 65.0 ± 11.9 kg (means ± SD) all exercised regularly, had been engaged in sport-specific training for, on average, 5.7 ± 3.9 years, and completed a medical questionnaire prior to the study. Ethical approval for the study was obtained in accordance with the regulations of the ethics committees of the university involved. In addition, all subjects provided written informed consent to participate after hearing the procedures they would be undertaking explained verbally.
Experimental design and procedures
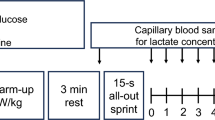
Within a single 3 day period, all subjects completed an incremental load test on a C2-SkiErg (Concept 2 Inc., USA). Prior to this test, they performed 5 min of dynamic stretching, followed by 5 min of resting while seated. Preliminary trials and adjustments were employed to determine that appropriate starting loads for the males and females were 50 and 40 W, respectively. This starting load was maintained for 3 min, after which the load was increased by 20 and 5 W for the men and women, respectively, during each consecutive 3 min period, with one-minute of seated rest prior to each increase. After completing a total of 5 such periods, the subjects rested for 5 min and then performed a 30 s all-out test.
During the test, the resistance of the ski ergometer was set at 4 and verbal encouragement provided throughout in order to ensure that the subjects performed exactly as instructed and attained the power required at each level. During each intensity level of the double poling exercise, a researcher informed the participant of the required power output based on the real-time ergometer display, ensuring the participant maintained the prescribed intensity for three minutes, after which the researcher recorded the average power output corresponding to the increasing poling speed.
Blood sampling
The gold standard bench-top lactate analyzer Biosen-S-Line (BSL: SensLab GmbH, Germany), manufactured by the same company as the LS4, was used to compare and validate differences between earlobe and fingertip measurements with the LS4 (Stefánsdóttir et al. 2012). Each participant needed to have blood drawn from both the earlobe and fingertip at specific times: before the test, at the end of each intensity stage, and at 1-, 3-, 5-, and 7-min post-exercise, totaling ten collections. Two skilled technicians stationed on either side of the resting area conducted these collections, each obtaining three blood samples using a BSL and two LS4s. Technician 1 collected with BSL [Earlobe], LS4-a[Earlobe], and LS4-b[Earlobe], while Technician 2 used BSL [Fingertip], LS4-b [Fingertip], and LS4-d [Fingertip]. The sequence and timing of the blood draws by both technicians were synchronized. Prior to collection, the site was cleaned with a pre-sterilized alcohol swab to eliminate any interference from hair or sweat. After drying the site, a new lancet was used to make a gentle puncture until a small amount of blood appeared. Then, 20 μL of blood were collected using a new blood collection tube. Immediately afterward, two LS4s, each fitted with a new sensor, were brought close to the blood droplet. The sensors quickly detected and absorbed approximately 0.2 μL of blood. After collecting blood with the LS4s, the site was cleaned again with an alcohol swab. Collecting blood with the tube took about 5 s, and the subsequent LS4 collections took about 2 s each. All blood samples were collected from the same puncture. After collection, the blood drawn by the technicians was handed over to their respective assistants for processing, which involved placing the capillary blood into a cup and mixing it with an anticoagulant. Then, both samples were measured using the same BSL. Data from the four LS4s were available shortly after the sensors had collected the blood.
Statistical analysis
Blood sample data from each comparison were arranged by size and divided into three intervals: 0 to 4.0 mmol/L, 4.0 to 8.0 mmol/L, and > 8.0 mmol/L. This categorization was based on the observation that variability between measurements increases as Bla rise (Tanner et al. 2010). Paired t-tests were used to compare differences between instruments and sampling sites, and Cohen’s d was used to evaluate the effect size (ES). Consistency between instruments was assessed using the concordance correlation coefficient (CCC) for repeated measures. The Bland–Altman method and limits of agreement (LoA) were employed to analyze the mean differences between instruments and between measurements at different sites. The correlation coefficients for repeated measures were used to evaluate the relationship between different instruments and sites. The ES, Cohen’s d, was determined, with values of 0.2 or −0.2 considered small, 0.5 or −0.5 medium, and 0.8 or −0.8 large (Nakagawa and Cuthill 2007). The CCC was interpreted as values < 0.70, 0.70–0.90, 0.90–0.95, 0.95–0.99, and > 0.99 indicating very poor, poor, moderate, good, and very good agreement, respectively. (Martins and Nastri 2014). Calculations for the paired sample t-test and effect size were performed using Excel. The CCC, Bland–Altman, and correlation coefficient (r) analyses were conducted using the ‘simplyagree’ and ‘rmcorr’ packages in R. In all cases a value of < 0.05 was considered statistically significant.
Results
Statistic description of all pooled data
Table 1 presents the mean and standard deviation of lactate concentrations obtained from the earlobe and fingertip sites in 40 participants, using one BSL device and four LS4s, during ten blood sampling sessions in this experiment. The average power of the five stages and the 30 s all-out are also indicated in Table 1. 240 lactate measurements were obtained in each of the first nine sampling sessions of this experiment, while the tenth session resulted in only 234 measurements due to the absence of data from one participant at 7 min post-exercise. Figure 1 illustrates the ten-stage lactate trend of a representative subject across six blood sampling sites.

One representative subject’s ten-stage lactate trend chart across the six blood sampling sites: BSL [E], BSL [F], LS4-a [E], LS4-b [E], LS4-c [F], and LS4-d [F]
Comparison of the Bla in earlobe and fingertip capillary blood
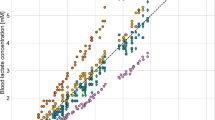
BSL measurements of fingertip Bla were significantly higher than earlobe Bla across all intervals. Mean bias based on Bland–Altman analysis was −0.66 mmol/L (95% CI: −2.18 to 0.86 mmol/L; CCC = 0.95; r = 0.97) using pooled data across all intervals. Table 2 and Fig. 2 include full details for these comparisons.

The scatter plots and Bland–Altman plots for comparisons between earlobe and fingertip Bla obtained using BSL. Subfigures a show scatter plots for comparisons between earlobe and fingertip Bla obtained using BSL. Subfigures b correspond to the respective Bland–Altman plots
The comparison between LS4s and BSL at the earlobe and fingertip site
No significant difference was found between BSL and LS4-a in the overall pooled data, but a significant difference was observed in the 0–4 mmol/L interval. Significant differences existed in the pooled data between BSL and LS4-b. For BSL and LS4-a, the mean bias based on Bland–Altman analysis was 0.05 mmol/L (95% CI: −2.69 to 2.80 mmol/L; CCC = 0.95; r = 0.94). For BSL and LS4-b, it was −0.16 mmol/L (95% CI: −2.87 to 2.56 mmol/L; CCC = 0.96; r = 0.95). Complete results are shown in Table 3 and Fig. 3.

The scatter plots and Bland–Altman plots for comparisons of Bla between BSL and LS4. Subfigures a, c, e and g respectively show scatter plots for comparisons between BSL [E] and LS4-a [E], BSL [E] and LS4-b [E], BSL [F] and LS4-c [F], BSL [F] and LS4-d [F]. Subfigures b, d, f and h correspond to the respective Bland–Altman plots
The comparison within LS4s at the earlobe and fingertip site
Comparisons within LS4s revealed significant differences across three intervals. For LS4-a and LS4-b at the earlobe, the mean bias based on Bland–Altman analysis was −0.21 mmol/L (95% CI: −3.25 to 2.83 mmol/L; CCC = 0.95; r = 0.94). For LS4-c and LS4-d at the fingertip, it was −1.04 mmol/L (95% CI: −7.39 to 5.31 mmol/L; CCC = 0.81; r = 0.77). Full details are provided in Table 4 and Fig. 4.

The scatter plots and Bland–Altman plots for comparisons of Bla within LS4s. Subfigures a and c respectively show scatter plots for comparisons between LS4-a [E] and LS4-b [E], LS4-c [F] and LS4-d [F]. Subfigures b and d correspond to the respective Bland–Altman plots
Discussion
Here, we explored Bla in capillary blood from the earlobe and fingertip during double poling on a SkiErg, which involves primarily upper-body muscles, as determined using two different types of measuring devices. Our major findings were that (1) fingertip Bla were significantly higher than those from the earlobe. (2) Comparing BSL with LS4, there were significant differences across various concentration intervals at both the earlobe and fingertip sites, indicating variability in the validity of LS4. (3) Within the LS4, there were significant discrepancies between different LS4 models at both the earlobe and fingertip sites, indicating variability in the reliability of LS4.
Comparison of the Bla in earlobe and fingertip capillary blood
An important finding in this study was that during SkiErg double poling, Bla determined with the BSL device was significantly higher in fingertip capillaries than in those in the earlobe, which is consistent with previous findings (Dassonville et al. 1998; Draper et al. 2006; Feliu et al. 1999; Yamagata et al. 2018). For instance, Yamagata found that during continuous cycling at intensities of 60% and 70% of maximal oxygen uptake, the Bla in fingertip was higher than in earlobe capillaries during the first 10 min of exercise (Yamagata et al. 2018). Similar observations have been made with other modes of exercise, such as running and rock climbing. In contrast, Moran observed no significant difference between fingertip and earlobe Bla during power cycling (Moran et al. 2012), probably because that investigation involved continuous low-intensity exercise rather than exercise with incremental increases in load.
When simulating the movements of cross-country skiing, our participants had to pull the handlebars with both hands and exert downward force. In connection with this process, the palm grasping the handlebar needs to maintain continuous force, which restricts blood flow and thus perhaps enhances lactate production and limits its removal, both during and after the exercise (Fryer et al. 2011). Indeed, it has been shown that the flow of blood in the fingers is reduced during cycling at a constant load (Midttun and Sejrsen 1998). Although cycling and skiing differ in many ways, both require the use of hand muscles.
Furthermore, it has been proposed that sympathetic nervous activity influences blood flow, which may, at least in part, explain differences in Bla in different regions of the body (Johnson 1992). Vessels in peripheral regions, including the fingertips and earlobes, are innervated primarily by sympathetic adrenergic vasoconstrictor nerves (Kellogg et al. 1991). At the onset of exercise, the activity of these nerves is enhanced, leading to the secretion of norepinephrine, which constricts blood vessels and limits blood flow in the skin.
Interestingly, despite consistently higher Bla levels in the fingertips than in the earlobes, the differences remained less than 1 mmol/L across all intensity intervals. This suggests that although localized lactate production may increase due to restricted blood flow and muscle activity in the fingertips, systemic circulation ensures relatively uniform lactate distribution across different body parts (Fryer et al. 2011). The relatively small differences imply moderate disparities in lactate production and removal between these sites, further emphasizing the role of local factors (such as muscle activity and restricted blood flow) and systemic physiological mechanisms in Bla levels. Therefore, fingertip readings may reflect more immediate changes due to local muscle exertion, whereas earlobe readings might better represent overall systemic lactate concentration.
It is also worth noting that sweating can impact Bla in blood samples (Pattersonet al. 2000), since the sweat produced during exercise contains a certain amount of lactate (Karpova et al. 2020). Thus, differences in the amount and nature of sweat produced at different sampling sites may also contribute to differences in the Bla observed (Feliu et al. 1999). However, in our case, prior to each blood collection, the fingertip or earlobe was disinfected with an alcohol swab, ensuring the site was dry and clean before proceeding with the puncture. This practice was adopted to ensure that the measurement results were not influenced by sweat, hair, or other factors present on the skin.
The validity and reliability of the LS4
Compared to the high-precision BSL, the LS4 demonstrated higher validity when capillary blood was collected from the earlobe (LS4-a: CCC of 0.95 and r of 0.94; LS4-b: CCC of 0.96 and r of 0.95) but poorer validity when collected from the fingertip (LS4-c: CCC of 0.78 and r of 0.82; LS4-d: CCC of 0.63 and r of 0.71). This finding is consistent with other reports that the Lactate Scout does not perform well in terms of accuracy (Bonaventura et al. 2015; Tanner et al. 2010). For example, Tanner observed that with Bla in the low-to-medium range, the values provided by the Lactate Scout showed a significant trend towards more pronounced deviation from those obtained with the ABL laboratory-based lactate analyzer, considered the gold standard. This observation is consistent with our findings of LS4’s diminished validity at the interval of 0 to 4 mmol/L.
The LS4 utilized in this study demonstrated poor reliability across three intervals at both sites. As illustrated in Fig. 1, the Bla from four LS4s for a single subject exhibited discernible variation at each blood sampling stage. Notably, these LS4s showed poorer performance compared to those in previous studies. (Bonaventura et al. 2015). For instance, Tanner found that although the Lactate Scout was not more accurate than the other two portable lactate analyzers utilized, it was reliable enough to be used in sports settings (with a SEE of 1.4 and the r of 0.837) (Tanner et al. 2010). Although the LS4-a and b here gave values for the Bla in earlobe capillary blood that were closely correlated (CCC of 0.95 and r of 0.94), the reliability of this lactate analyzer was reduced at certain exercise intensities. Especially when capillary blood was collected from the fingertip, the differences in the Bla in all three ranges measured simultaneously by the LS4-c and d were significant.
The limited validity and reliability of the LS4 can be primarily attributed to the differences in measurement principles between the LS4 and the BSL. The BSL employs advanced chip sensor technology and electrochemical methods for lactate detection, ensuring high precision and stability. In contrast, the LS4 uses an enzymatic-amperometric detection method (Rathee et al. 2016). Although this method enhances the LS4’s portability and ease of use, it compromises measurement precision and stability, making the device more susceptible to environmental and operational influences.
The LS4 demonstrates poorer validity and reliability when used at the fingertip due to several factors. There are inherent differences in blood flow and lactate concentration between the earlobe and the fingertip. Capillary blood sampling from the fingertip often necessitates “squeezing” to obtain sufficient blood, which can introduce interstitial fluid and affect lactate concentration measurements (Krleza et al. 2015). Additionally, the process of squeezing can cause hemolysis, especially when a disinfecting agent is applied, thereby increasing lactate concentration and skewing results (Krleza et al. 2015). Most critically, the LS4’s inherent instability amplifies these issues, making the discrepancies between measurements at the fingertip and earlobe even more pronounced. This inherent instability is the primary problem, exacerbating all other factors and leading to greater inconsistency in measurements from the fingertip compared to the earlobe.
Practical implications
This study provides critical insights into the practical implications of using different sampling sites and lactate analyzers during cross-country skiing. The first significant finding is the notable difference in lactate concentrations between the earlobe and fingertip, with the discrepancy being less than 1 mmol/L. Although seemingly minor, this difference is crucial as it can significantly impact the assessment of exercise intensity based on lactate concentration. Therefore, it is recommended to consistently use the same sampling site for accurate and reliable results (Moran et al. 2012). The earlobe is suggested as a more stable and preferable site due to its lower variability compared to the fingertip.
The second important finding concerns the validity and reliability of the LS4 lactate analyzer. The LS4 showed poor validity and reliability, particularly when used at the fingertip. Although the LS4’s performance improved slightly when used at the earlobe, it still displayed significant discrepancies compared to the high-precision BSL analyzer. Given the LS4’s inherent instability, it is advisable to exercise caution when using it as the sole device for lactate measurement in sports settings. The potential for measurement errors and the device’s sensitivity to environmental and operational factors make it less reliable than more stable alternatives like the BSL. Therefore, practitioners and coaches should be cautious in interpreting lactate data obtained using the LS4, especially from fingertip samples.
Limitations
The limitations of the current investigation include the following: First, we selected SkiErg double poling as the cyclic movement involving hand-grasping, but this hand-grasping differs in some ways from that involved in rowing and cycling. Therefore, it remains to be seen whether our findings can be extended to other exercise modalities as well. Secondly, we utilized only one brand of portable lactate analyzer (i.e., the LS4) and other brands, such as the LP2 and LP, remain to be examined(Tanner et al. 2010). Third, although each stage in the experiment lasted no more than three minutes that is inadequate for blood lactate to reach a steady state(Jakobsson and Malm 2019), the difference in corresponding Bla between devices and sites at each timepoint was not affected, since blood was collected almost simultaneously. Last, while the participants in this study were not specialized cross-country skiers and had limited double poling skill, the purpose was solely to examine differences in Bla using different devices and sites across exercise intensities, thus their role was simply to have Bla produced.
Conclusions
The data presented here indicate significant differences in blood lactate concentrations between the earlobe and fingertip during SkiErg double poling, with fingertip values consistently higher, although the discrepancy is less than 1 mmol/L. This difference can impact the assessment of exercise intensity based on lactate concentration. Additionally, the LS4 analyzer exhibited poor validity and reliability, particularly at the fingertip, compared to the high-precision BSL analyzer. Given the LS4’s inherent instability, it is advisable to use the earlobe for more consistent and reliable lactate measurements. Coaches and practitioners should reconsider the use of LS4 for lactate measurement in sports settings and standardize earlobe sampling to ensure accurate and stable results.
Data availability
The authors of this study will unconditionally provide the raw data that supports their conclusions.
References
Baldari C, Bonavolontà V, Emerenziani GP, Gallotta MC, Silva AJ, Guidetti L (2009) Accuracy, reliability, linearity of accutrend and lactate pro versus EBIO plus analyzer. Eur J Appl Physiol 107(1):105–111. https://doi.org/10.1007/s00421-009-1107-5
Belic M, Radin L, Brkljaca Bottegaro N, Beer Ljubic B, Benic M, Stanin D, Vrbanac Z (2016) Reliability of lactate scout portable analyzer in agility dogs during multiple measurements. Acta Vet-Beogr 66(4):549–555. https://doi.org/10.1515/acve-2016-0047
Bonaventura JM, Sharpe K, Knight E, Fuller KL, Tanner RK, Gore CJ (2015) Reliability and accuracy of six hand-held blood lactate analysers. Int J Sports Med 12:203
Brooks GA (1986) The lactate shuttle during exercise and recovery. Med Sci Sports Exerc 18(3):360–368. https://doi.org/10.1249/00005768-198606000-00019
Crotty NM, Boland M, Mahony N, Donne B, Fleming N (2021) Reliability and validity of the lactate Pro 2 analyzer. Meas Phys Educ Exerc Sci 25(3):202–211. https://doi.org/10.1080/1091367X.2020.1865966
Dassonville J, Beillot J, Lessard Y, Jan J, André AM, Le Pourcelet C, Rochcongar P, Carré F (1998) Blood lactate concentrations during exercise: effect of sampling site and exercise mode. J Sports Med Phys Fitness 38(1):39–46
Draper N, Brent S, Hale B, Coleman I (2006) The influence of sampling site and assay method on lactate concentration in response to rock climbing. Eur J Appl Physiol 98(4):363–372. https://doi.org/10.1007/s00421-006-0289-3
El-Sayed MS, George KP, Dyson K (1993) The influence of blood sampling site on lactate concentration during submaximal exercise at 4 mmol/L lactate level. Eur J Appl Physiol 67(6):518–522. https://doi.org/10.1007/BF00241648
Faude O, Kindermann W, Meyer T (2009) Lactate threshold concepts: how valid are they? Sports Med 39(6):469–490. https://doi.org/10.2165/00007256-200939060-00003
Feliu J, Ventura JL, Segura R, Rodas G, Riera J, Estruch A, Zamora A, Capdevila L (1999) Differences between lactate concentration of samples from ear lobe and the finger tip. J Physiol Biochem 55(4):333–339
Ferasin L, Dodkin SJ, Amodio A, Murray JK, Papasouliotis K (2007) Evaluation of a portable lactate analyzer (lactate scout) in dogs. Vet Clin Pathol 36(1):36–39. https://doi.org/10.1111/j.1939-165X.2007.tb00179.x
Forsyth JJ, Farrally MR (2000) A comparison of lactate concentration in plasma collected from the toe, ear, and fingertip after a simulated rowing exercise. Br J Sports Med 34(1):35–38. https://doi.org/10.1136/bjsm.34.1.35
Foxdal P, Sjödin B, Rudstam H, Östman C, Östman B, Hedenstierna GC (1990) Lactate concentration differences in plasma, whole blood, capillary finger blood and erythrocytes during submaximal graded exercise in humans. Eur J Appl Physiol 61(3–4):218–222. https://doi.org/10.1007/BF00357603
Fryer S, Draper N, Dickson T, Blackwell G, Winter D, Ellis G (2011) Comparison of lactate sampling sites for rock climbing. Int J Sports Med 32(6):428–432. https://doi.org/10.1055/s-0031-1271712
Ghosh AK (2004) Anaerobic threshold: its concept and role in endurance sport. Malays J Med Sci 11(1):24–36
Holmberg H-C, Lindinger S, StöGgl T, Eitzlmair E, Müller E (2005) Biomechanical analysis of double poling in elite cross-country skiers. Med Sci Sports Exerc 37(5):807–818. https://doi.org/10.1249/01.MSS.0000162615.47763.C8
Jakobsson J, Malm C (2019) Maximal lactate steady state and lactate thresholds in the cross-country skiing sub-technique double poling. Int J Exerc Sci 12(2):57–68
Johnson JM (1992) Exercise and the cutaneous circulation. Exerc Sport Sci Rev 20:59–97
Karpova E, Laptev A, Andreev E, Karyakina E, Karyakin A (2020) Relationship between sweat and blood lactate levels during exhaustive physical exercise. ChemElectroChem 7:191–194. https://doi.org/10.1002/celc.201901703
Kaynar O, Karapinar T, Hayirli A, Baydar E (2015) Reliability of the lactate scout point-of-care instrument for the determination of blood L-lactate concentration in sheep. Vet Clin Pathol 44(4):559–563. https://doi.org/10.1111/vcp.12288
Kellogg DL, Johnson JM, Kosiba WA (1991) Competition between cutaneous active vasoconstriction and active vasodilation during exercise in humans. Am J Physiol Heart Circ Physiol 261(4):H1184–H1189. https://doi.org/10.1152/ajpheart.1991.261.4.H1184
Krleza JL, Dorotic A, Grzunov A, Maradin M (2015) Capillary blood sampling: national recommendations on behalf of the croatian society of medical biochemistry and laboratory medicine. Biochemia Medica 25(3):335
Martins WP, Nastri CO (2014) Interpreting reproducibility results for ultrasound measurements: correspondence. Ultrasound Obstet Gynecol 43(4):479–480. https://doi.org/10.1002/uog.13320
Mc Naughton LR, Thompson D, Philips G, Backx K, Crickmore L (2002) A comparison of the lactate pro, accusport, analox GM7 and kodak ektachem lactate analysers in normal, hot and humid conditions. Int J Sports Med 23(2):130–135. https://doi.org/10.1055/s-2002-20133
Midttun M, Sejrsen P (1998) Cutaneous blood flow rate in areas with and without arteriovenous anastomoses during exercise. Scand J Med Sci Sports 8(2):84–90. https://doi.org/10.1111/j.1600-0838.1998.tb00173.x
Moran P, Prichard JG, Ansley L, Howatson G (2012) The influence of blood lactate sample site on exercise prescription. J Strength Cond Res 26(2):563–567. https://doi.org/10.1519/JSC.0b013e318225f395
Nakagawa S, Cuthill IC (2007) Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev 82(4):591–605
Patterson MJ, Galloway SDR, Nimmo MA (2000) Variations in regional sweat composition in normal human males. Exp Physiol 85(6):869–875. https://doi.org/10.1111/j.1469-445X.2000.02058.x
Poole DC, Rossiter HB, Brooks GA, Gladden LB (2021) The anaerobic threshold: 50+ years of controversy. J Physiol 599(3):737–767. https://doi.org/10.1113/JP279963
Rathee K, Dhull V, Dhull R, Singh S (2016) Biosensors based on electrochemical lactate detection: a comprehensive review. Biochem Biophys Rep 5:35–54. https://doi.org/10.1016/j.bbrep.2015.11.010
Robergs R, Chwalbinska-Moneta J, Mitchell J, Pascoe D, Houmard J, Costill D (1990) Blood lactate threshold differences between arterialized and venous blood. Int J Sports Med 11(06):446–451. https://doi.org/10.1055/s-2007-1024835
Sakharov D, Shkurnikov M, Vagin MY, Yashina EI, Karyakin AA, Tonevitsky A (2010) Relationship between lactate concentrations in active muscle sweat and whole blood. Bull Exp Biol Med 150:83–85. https://doi.org/10.1007/s10517-010-1075-0
Stefánsdóttir GJ, Ragnarsson S, Jansson A (2012) A comparison of a portable blood lactate analyser and laboratory plasma analysis of blood samples from exercised horses. Comp Exerc Physiol 8(3–4):227–231. https://doi.org/10.3920/CEP13002
Stewart MT, Stavrianeas S (2008) Studying reliability using identical handheld lactate analyzers. Adv Physiol Educ 32(2):165–166. https://doi.org/10.1152/advan.90106.2008
Stöggl T, Holmberg H-C (2011) Force interaction and 3D pole movement in double poling: force interaction and 3D in double poling. Scand J Med Sci Sports 21(6):e393–e404. https://doi.org/10.1111/j.1600-0838.2011.01324.x
Tanner RK, Fuller KL, Ross MLR (2010) Evaluation of three portable blood lactate analysers: lactate pro, lactate scout and lactate plus. Eur J Appl Physiol 109(3):551–559. https://doi.org/10.1007/s00421-010-1379-9
van Someren KA, Howatson G, Nunan D, Thatcher R, Shave R (2005) Comparison of the lactate pro and analox GM7 blood lactate analysers. Int J Sports Med 26(8):657–661. https://doi.org/10.1055/s-2004-830337
Williams JR, Armstrong N, Kirby BJ (1992) The influence of the site of sampling and assay medium upon the measurement and interpretation of blood lactate responses to exercise. J Sports Sci 10(2):95–107. https://doi.org/10.1080/02640419208729912
Yamagata T, Kume D, Wakimoto T, Nagao N (2018) The influence of sampling site on blood lactate response to steady state exercise. J Sports Sci 6:276–284
Yoshida T, Takeuchi N, Suda Y (1982) Arterial versus venous blood lactate increase in the forearm during incremental bicycle exercise. Eur J Appl Physiol 50(1):87–93. https://doi.org/10.1007/BF00952247
Acknowledgements
The authors express their gratitude to the athletes and testers who generously participated in the study, and provided support despite such a challenging case. The authors declare that they have no conflicts of interest to report.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
Yongming Li conceived and designed the study. Xinxin Wang and Fogen Zhong performed the experiments. Lizhi Chen and Fogen Zhong analyzed the data. Fogen Zhong drafted the manuscript. Zhengqiu Gu reviewed the manuscript. Yongming Li and Hans-Christer Holmberg critically revised the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Conflict of interest
The authors state that this study was conducted without any commercial or financial relationship that could be interpreted as a potential conflict of interest.
Ethical approval
The research protocols involving human subjects were subjected to rigorous review and received approval from the ethical committee at Shanghai University of Sport. All individuals who participated in the study provided explicit written consent after receiving adequate information about the nature and scope of the study.
Additional information
Communicated by I. Mark Olfert.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhong, F., Chen, Z., Gu, Z. et al. Comparison of lactate measurements from earlobe and fingertip capillary blood using Biosen S-Line and lactate scout analyzers. Eur J Appl Physiol (2024). https://doi.org/10.1007/s00421-024-05585-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00421-024-05585-1