
Abstract
Purpose
Our purpose was to compare supramaximal versus submaximal intensity eccentric training performed until volitional fatigue.
Methods
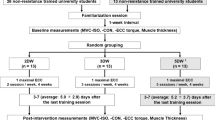
Thirty-two young adults (19 males) were randomized into one of three groups: (1) ECC110 performed eccentric (ECC) only contractions at 110% of concentric (CON) 1-repetition maximum (1RM); (2) ECC80 performed ECC only contractions at 80% of CON 1RM; (3) a control group. Training progressed from 3 to 6 sets of unilateral ECC training of the elbow flexors over 8 weeks, with each set performed until volitional fatigue. Elbow flexors muscle thickness (via ultrasound) and 1RM were assessed pre- and post-training. Rating of perceived exertion (RPE) and muscle soreness was self-reported.
Results
Both ECC110 (+0.25 cm) and ECC80 (+0.21 cm) showed a greater post-training increase in muscle thickness compared to control (−0.01 cm) (p < 0.05), with no differences between ECC110 and ECC80. ECC80 (+1.23 kg) showed a greater post-training increase in strength compared to control (p < 0.05), while ECC110 (+0.76 kg) had no significant difference post-training vs. control (−0.01 kg). ECC80 had significantly lower average RPE scores than ECC110 (p < 0.05).
Conclusions
Both supramaximal intensity eccentric training and submaximal intensity eccentric training are effective for increasing muscle size, but submaximal eccentric training is perceived to require less exertion than supramaximal training. These findings suggest that submaximal eccentric training may be an ideal strategy to increase muscle size and strength in individuals whose needs warrant training at a lower level of exertion.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The pursuit of optimal muscle hypertrophy has long been investigated during adaptations to resistance training, and remains a controversial and popular topic for physiology and exercise scientists. Populations ranging from advanced and elite lifters to clinical populations suffering from disuse atrophy or disease cachexia (Roig et al. 2008) may all benefit from training protocols leading to increased muscle mass. Well-known and generally accepted training prescriptions (Ratamess et al. 2009) (America College of Sports Medicine Positions Stand) suggest that muscle hypertrophy is optimized using moderate-to-heavy loads; 70–85% of one repetition maximum (1RM) for novice and intermediate and 70–100% 1RM for advanced lifters. These different training recommendations recognize that responses to muscle hypertrophy may be affected by the training status of the lifter. Lifters who are untrained exhibit longer lasting and greater overall muscle protein synthesis rates following training sessions compared to those classified as trained (Damas et al. 2015), although less is known about the relationship between training status, training intensity, and chronic muscle hypertrophy. Recent topical reviews focusing on training intensity and muscle hypertrophy suggest much less clarity in this area and summarize evidence on the efficacy of both high and low load training prescriptions for muscle hypertrophy (Fisher et al. 2013; Schoenfeld et al. 2016; Fisher et al. 2017).
A number of studies have shown no differences in training-induced muscle hypertrophy when comparing higher versus lower intensity resistance training protocols (Hisaeda et al. 1996; Chestnut and Docherty 1999; Tanimoto and Ishii 2006; Mitchell et al. 2012; Alegre et al. 2015). Burd and colleagues (2010) report that protein synthesis is stimulated more with low load resistance (30% 1RM) than high (90% 1RM) when both intensities are performed to failure. In explaining their findings, Burd et al. suggest that performing contractions to volitional fatigue (i.e., failure) is more important than the intensity of contraction for activating all motor units, including the high threshold type II fibers. Other studies maintain that lower intensity training remains inferior to high-intensity for muscle hypertrophy (Campos et al. 2002; Holm et al. 2008; Schuenke et al. 2012). To date, no investigation has compared hypertrophic adaptations after high- versus low-intensity eccentric (i.e., lengthening) training. This gap in the literature is noteworthy considering the evidence that eccentrically emphasized training generally leads to greater gains in strength and muscle hypertrophy compared to concentric (shortening) training (Higbie et al. 1996; Seger et al. 1998; Hortobágyi et al. 1996; Farthing and Chilibeck 2003b).
Torque–velocity curves indicate that greater force is produced during eccentric contractions in comparison to concentric contractions (Sale et al. 1987; Hortobáygi and Katch 1990; Westing et al. 1990, 1991; Farthing and Chilibeck 2003b). Intuitively when the eccentric portion of a conventional lifting exercise is emphasized, training can be performed at levels that are greater than 100% of an individual’s concentric 1-RM (known as supramaximal eccentric training). A systematic review by Roig and colleagues (2009) examined the issue of eccentric versus concentric training and concluded that eccentric training, when performed at a higher intensity than concentric training, was more effective for increasing total strength and muscle mass. They suggested that the superiority of eccentric training was likely mediated by the ability of such contractions to produce greater forces during training. Farthing and Chilibeck (2003b) also proposed the idea that the efficacy of eccentric training results from the ability to train with greater intensity than concentric training. Other studies have matched for volume (Hortobágyi et al. 1996) or work (Moore et al. 2005), and reported inherent advantages of eccentric contractions over concentric contractions.
For a given amount of force produced, eccentric contractions have a lower oxygen cost (LaStayo et al. 1999; Meyer et al. 2003) and lower ratings of perceived exertion (Hollander et al. 2003) than concentric contractions. Intense eccentric training is associated with decreased strength and an increase in delayed onset muscle soreness in the days following training sessions (Nosaka and Clarkson 1996; Tokmakidis et al. 2003; Krentz and Farthing 2010). This is likely due to a combination of factors including higher force production during eccentric training and sarcomere disruption specifically associated with lengthening contractions (Shepstone et al. 2005). Submaximal intensity eccentric training has been reported to show less deleterious effects than maximal eccentric training (Nosaka and Newton 2002), and past research on training intensity suggests that training with lower intensities may lead to greater exercise adherence (Perri et al. 2002). Optimization of minimally damaging and lower exertional eccentric training protocols is important in the continued application of eccentric training to a wide variety of individuals, especially clinical populations.
To our knowledge, no research has compared muscle hypertrophy and strength adaptations in response to submaximal versus supramaximal eccentric training when both are performed until volitional fatigue. The purpose of this investigation was to compare supramaximal versus submaximal intensity eccentric training performed until volitional fatigue. The primary hypotheses were that supramaximal eccentric training would be superior to submaximal eccentric training for increasing concentric strength and that both types of eccentric training would significantly increase muscle size compared to control. Due to the limited evidence available, it was difficult to predict which intensity of eccentric training would yield superior muscle hypertrophy, but original concentric-focused work in this area (Burd et al. 2010) suggests that low loads performed to failure may be superior due to greater overall training volume. The secondary hypothesis was that higher intensity (supramaximal) eccentric training will result in higher ratings of perceived exertion and greater muscle soreness than lower intensity eccentric training.
Methods
Participants
Ethical approval for the study was obtained from the University of Saskatchewan Biomedical Ethics Review Board, and all participants gave informed written consent before participating. A total of 44 (22 male) participants were initially enrolled in the study and completed the pre-testing procedures. Young healthy males and females with varied training experience were included to allow for greater generalizability, and because many studies have shown similar time course of adaptation across sexes (Cureton et al. 1988; Staron et al. 1994; Abe et al. 2000; Krentz and Farthing 2010). Once enrolled, participants were asked to continue their regular exercise regime and, if assigned to one of the training groups, to refrain from any additional targeted training of the elbow flexors aside from that prescribed in the study. Participant characteristics are outlined in Table 1.
Study design
The study utilized a between-subjects design consisting of pre- and post-testing after 8 weeks of unilateral elbow flexors concentration curl resistance training. Upon completion of the pre-testing session, participants were randomized to one of three groups [ECC110 performed eccentric (ECC) only contractions at 110% of concentric (CON) 1–repetition maximum (1RM), ECC80 performed ECC only contractions at 80% of CON 1RM, or a control group that did no training] in a counterbalanced fashion using a random number generator (www.random.org), with stratification by sex. All measurements were taken in the same order for each participant on pre- and post-intervention visits. Specifically, participants’ dominant arm muscle thickness was measured first followed by concentric dumbbell 1RM of that same arm.
During the 8 weeks of training, concentric concentration curl 1RM was reassessed at the start of weeks 3 and 6. Monitoring of 1RM during the study allowed for adequate prescription of eccentric training intensities according to each participant’s individual progression in concentric 1RM strength.
Training programs
All training groups performed dominant limb unilateral training of the elbow flexors (i.e., concentration curls) to volitional fatigue using iso-inertial eccentric loading (i.e., dumbbell hand-held weights) where the load was lowered uniformly through the full range of motion for 3 s. Volitional fatigue was defined as the point where the participant could no longer control the resistance for the full three-second phase of the movement or through the full range of motion. The non-dominant limb was used to assist the dominant limb during performance of the concentric portion of the lift. The training period of the study lasted 8 weeks and involved progressive overload. Participants started their first training session by completing three sets of their assigned contractions to volitional fatigue. The training progression then continued by adding one set to each training session until participants reached six sets. Rest between sets was 2 min. Past research from our lab has shown that intense training eccentrically every second day for 20 days using a dynamometer resulted in reduced strength and general overtraining (Krentz and Farthing 2010). For this reason, participants trained two sessions a week with at least 72 h rest in between sessions for the first 2 weeks and then progressed to three training sessions a week for the final 6 weeks of the study. If a participant was able to perform more than 20 repetitions for all prescribed sets, they were instructed to increase the training weight for the next training session. However, this increase was only prescribed if the increased training load still remained within 10% of the prescribed training intensity for that group (110 or 80% 1RM). In addition, if participants were not able to perform at least four repetitions for all prescribed sets, the training weight was lowered for the next training session. As above, this decrease was only permitted if the load remained within 10% of the assigned training intensity. These practical modifications allowed for training to be performed until volitional fatigue during all sessions while ensuring that training was performed within the prescribed repetition ranges (i.e., 8–12) appropriate for optimally increasing both strength and hypertrophy (Ratamess et al. 2009). At the completion of the training phase, participants were given a minimum of 72 h rest before completing the post-testing session to ensure full recovery.
Measures
Muscle thickness
Muscle thickness of the dominant elbow flexors was measured before and after the 8 week training period using B-mode ultrasound (LOGIQ e BTO8, GE Healthcare, Milwaukee, Wisconsin, USA) according to our previous methods (Farthing et al. 2005; Krentz and Farthing 2010). The coefficient of variation for this technique for elbow flexors is 2.14% (Krentz and Farthing 2010).
Muscle thickness measures always preceded strength measures to avoid the confounding effects associated with transient muscle edema. Elbow flexor muscle thickness was taken on the midline of the biceps brachii muscle belly between the medial acromion and the fossa cubit, approximately 1/3 of the distance away from the fossa cubit. Once this point was established, a detailed land marking procedure (using overhead transparencies) was employed to ensure exact placement of the ultrasound probe pre- and post-training (Farthing and Chilibeck 2003a; Krentz and Farthing, 2010). Four measurements were taken on and the averages of the two closest measurements were used to calculate the muscle thickness value.
Iso-inertial maximal strength testing
Iso-inertial strength of the elbow flexors of the dominant arm was assessed using a maximal unilateral concentric concentration curl. Briefly, a concentration curl is a movement where, in a seated position, one arm is rested against the upper thigh for support and the elbow flexors are used to lift a dumbbell (Fig. 1). Participants were instructed to lift the weight off the ground vertically and then pause briefly before attempting the actual lift. Instructions were given to lift the weight in a controlled fashion without leaning their upper body back or other postural compensations.

Concentration curl setup
Prior to beginning maximal lifts, participants were given a light weight to perform 1–2 warm-up sets. Participants then attempted a weight they were confident they could lift. Participants then rested before performing the next weight (approximately 2–3 min). One repetition maximum was determined as the highest weight that could be successfully lifted one time.
Muscle soreness
Muscle soreness of the dominant arm was tracked daily the first 3 weeks of the study using a visual analog scale (VAS), where participants indicated their degree of muscle soreness from 0 to 100 by making a mark on a 100 mm horizontal line on paper. Muscle soreness was monitored only for the first 3 weeks of the study, since our previous research suggests soreness peaks within the first few weeks of training and then decreases to near zero (Krentz et al. 2008). Soreness scores were recorded after completing a standard movement, involving first lengthening, and then shortening (contracting) the biceps in a slow controlled manner. When reporting soreness on a training day, participants were instructed to always record soreness prior to the training session.
Ratings of perceived exertion
All participants were instructed to record a session RPE score upon completion of training each day, using a modified session RPE scale (Foster et al. 2001; McGuigan and Foster, 2004). The scale ranges from 1 to 10, with accompanying verbal descriptions of each numerical rating. Participants were instructed to wait 30 min after the training session and then used this scale to indicate a composite RPE for the training session based on the question “How was your workout?” (McGuigan and Foster 2004). This RPE scale has been reported as a valid measure of both aerobic and anaerobic exercise (Foster et al. 2001). Specific to resistance training, session RPE is a valid (Sweet et al. 2004) and reliable (Day et al. 2004; McGuigan et al. 2004) monitoring tool.
Volume load
All participants were instructed to record the number of repetitions completed and load utilized during each set of training. From these data, average volume load per training session was calculated. Volume load was calculated by multiplying the total number of repetitions completed by the training load (kg) for each training session (McBride et al. 2009). All completed training sessions were tallied and then the total volume load was divided by the total number of possible training sessions for each participant (22 total sessions) to calculate an average volume load per training session.
Data analysis
Data distributions were tested for statistical assumptions of normality before proceeding with further omnibus tests. All data analyses were performed with IBM SPSS, version 22 for Windows. Post-training muscle thickness and concentric 1RM iso-inertial strength were assessed via MANCOVA for two dependent measures, and using pre-training values as covariates. MANCOVA was followed by univariate ANCOVA when appropriate for each of the variables. Muscle soreness and RPE were analyzed separately using two-way [group (ECC110, ECC80) × time (cumulative weekly score for week 1, week 2, and week 3 for muscle soreness; average daily score for weeks 1 + 2, weeks 3 + 4, weeks 5 + 6, and weeks 7 + 8 for RPE)] repeated measures factorial ANOVA. Simple effects analysis and post hoc multiple comparisons (adjusted for familywise error) were performed when appropriate. Volume load was analyzed using an independent t test to examine potential differences between the two training groups (ECC110 and ECC80). Effect size was calculated for MANCOVA and ANCOVA. Effect size values are generally accepted as follows: 0.1 = small, 0.3 = medium, and 0.5 = large (Cohen 1992). Significance was set at p < 0.05. In the case of missing data points resulting from missing training and/or soreness logs (self-reported RPE, muscle soreness, and volume load), only completer data were used for analysis.
Results
Final group enrollment
Of the 44 participants initially enrolled, 32 completed the study. Details of those who withdrew were as follows: ECC110 two males, five females; ECC80 one male, four females. Reasons for withdrawal were as follows: ECC110: three due to time, two due to soreness and pain, two undisclosed; ECC80: four due to time, one undisclosed.
Muscle thickness and strength
MANCOVA revealed a significant group effect (Pillai’s Trace = 0.549, F (4,54) = 5.114, p < 0.01). Univariate ANCOVA revealed a significant group effect for muscle thickness (F (2,27) = 9.09, p < 0.01 partial η 2 = 0.402. Pairwise comparisons on post-training means adjusted for familywise error (p < 0.05/3) revealed that both ECC110 (3.82 cm) and ECC80 (3.78 cm) were significantly greater than control (3.56 cm) (p < 0.01). There was no significant difference between ECC110 and ECC80 (Fig. 2).

Muscle thickness values compared to a covariate adjusted pre-value of 3.57 cm. Asterisk indicates significantly different than both ECC110 (p < 0.01) and ECC80 (p < 0.01). Values are mean ± SEM
Univariate ANCOVA for strength revealed a significant group effect (F (2,27) = 5.70, p < 0.01 partial η 2 = 0.297). Pairwise comparisons on post-training means adjusted for familywise error revealed that ECC80 (16.9 kg) was significantly greater than control (15.7 kg) (p < 0.01) but not different than ECC110 (16.4 kg). There was no significant difference between ECC110 and control (Fig. 3).

Strength values compared to a covariate adjusted pre-value of 15.7 kg. Asterisk indicates significantly different than control (p < 0.01). A non-significant trend (p = 0.065) was present for ECC110 different compared to control. Values are mean ± SEM
Volume load
Upon completion of the study, subjects were instructed to hand back completed training logs to analyze volume load. Unfortunately, not all participants handed back completed log books. For calculation and analysis of volume load, only completer data were used (n = 5 for ECC110, n = 8 for ECC80). Results of the independent t test indicated no significant differences for average volume load per training session between ECC110 and ECC80, t (11) = −0.972, p = 0.352 (Fig. 4). It should be noted that use of completer data for analysis due to missing data points could be a limitation if the completer data were not representative of the entire group. As a check of completer data, additional analysis was performed in which group means were imputed for each missing data point. Results of this analysis were not different than when only completer data were used.

Average volume load per training session. Values are mean ± SEM
Muscle soreness
Similar to volume load, not all muscle soreness logs were returned for analysis; therefore, only completer data were used for analysis (n = 6 for ECC110, n = 8 for ECC80). Results of the omnibus ANOVA revealed a significant main effect of time Greenhouse–Geisser (GG), [F (1.10,13.18) = 14.98, p < 0.01]. Soreness decreased from week 1 to week 3 (p < 0.01; Fig. 5). There was no significant main effect of group and no group × time interaction (p = 0.364). Additional analysis was completed in which group means were imputed for each missing data point and the results of this analysis were not different than when completer data were used.

Cumulative weekly muscle soreness. Asterisk indicates a significant main effect of time pooled across groups (p < 0.01). Values are mean ± SEM
Ratings of perceived exertion (RPE)
In line with volume load, not all training logs containing RPE were returned for analysis; therefore, only completer data were used for analysis (n = 5 for ECC110, n = 8 for ECC80). Results of the 4 (bi-weekly) × 2 (group) repeated measures factorial ANOVA for RPE indicated a significant main effect of group, F (1,11) = 6.70, p < 0.05. There was no significant main effect of time and no significant group × time interaction (p > 0.05). RPE was significantly lower for ECC80 throughout the study (Fig. 6). Additional analysis was completed in which group means were imputed for each missing data point and the results of this analysis were not different than when only completer data were used.

Biweekly ratings of perceived exertion. Asterisk indicates ECC110 significantly different than ECC80, averaged across all weeks (p < 0.05). Values are mean ± SEM
Discussion
The main finding of our study is that both supramaximal (ECC110) and submaximal (ECC80) intensity eccentric training resulted in equal gains in muscle hypertrophy (Fig. 2), but that submaximal intensity training resulted in significantly lower self-reported ratings of perceived exertion (Fig. 6) and was the only training method of the two tested to result in greater increases in strength compared to control. The role of training intensity in resistance training has gained popularity in the literature and led to significant scientific investigation and debate. Though many studies have contributed to this discussion (Hisaeda et al. 1996; Chestnut and Docherty 1999; Tanimoto and Ishii 2006; Burd et al. 2010; Mitchell et al. 2012; Alegre et al. 2015; Schoenfeld et al. 2015; Jenkins et al. 2016), the present study is the first to do so comparing eccentrically emphasized training. These findings suggest that submaximal intensity eccentric training may be an effective alternative to more commonly prescribed supramaximal eccentric training due to its ability to produce similar gains in muscle size while requiring less exertion to perform.
Our findings of similar muscle hypertrophy between supramaximal and submaximal intensity training groups are congruent with several studies which have investigated high- vs. low-intensity concentric training (Hisaeda et al. 1996; Chestnut and Docherty 1999; Tanimoto and Ishii 2006; Mitchell et al. 2012; Ogasawara et al. 2013; Alegre et al. 2015; Schoenfeld et al. 2015; Jenkins et al. 2016). An important commonality between the current study and many previous is training-induced fatigue. This has been accomplished in other studies through performance of equal reps with longer time under tension (Tanimoto and Ishii 2006) or more commonly by performing repetitions until volitional fatigue for each set (Mitchell et al. 2012; Ogasawara et al. 2013; Schoenfeld et al. 2015; Jenkins et al. 2016). In the current study, participants performed repetitions until volitional fatigue as defined by successful completion of eccentric repetitions. Although completed repetitions were free to vary between ECC110 and ECC80, there was no significant difference between the training groups for average volume load per training session (Fig. 4). Our results support the proposition that training to failure may be more important for muscle hypertrophy than the intensity (relative to 1RM) of a given training session (Burd et al. 2010) and, to our knowledge, we are the first to extend this idea to eccentrically emphasized training protocols.
The finding that lower intensity training resulted in similar gains in muscle size (Fig. 2) with a lower rating of perceived exertion (Fig. 6) has important clinical ramifications. One reason for the renewed interest in high- vs. low-intensity resistance training outcomes is related to the limited accessibility of high-intensity training in recreational and clinical settings. Literature from both the American Heart Association (Williams et al. 2007) and the American College of Sports Medicine suggests that high-intensity training may be contraindicated for various clinical populations. It has previously been established that eccentric contractions result in lower ratings of perceived exertion (Hollander et al. 2003) and lower oxygen cost per unit of force (LaStayo et al. 1999; Meyer et al. 2003) than concentric contractions, leading to suggestions that eccentric training may be beneficial for a number of clinical populations in which high exertion levels may be contraindicated (Roig et al. 2008). This application of eccentric training may be promising for patients suffering from a number of chronic health conditions including cardiovascular disease (Steiner et al. 2004), chronic obstructive pulmonary disease (Rooyackers et al. 2003), Parkinson’s disease (Dibble et al. 2006), stroke (Engardt et al. 1995), and Type 2 Diabetes (Marcus et al. 2008). The current findings that low-intensity eccentric training is as effective for muscle hypertrophy with lower RPE than high-intensity training supports this type of training as a good fit for clinical populations who may benefit from increased muscle mass but may not be able to train with maximal intensities. In addition, lower adherence rates have been reported for higher intensity training programs in healthy populations (Perri et al. 2002), suggesting that lower intensity resistance training may enhance adherence and ultimately greater long-term training outcomes.
Although numerous studies have reported equally effective muscle hypertrophy between high- vs. low-intensity concentric training, increases in strength have favoured more traditionally prescribed high-intensity training programs (Rana et al. 2008; Mitchell et al. 2012; Schoenfeld et al. 2015). As such, we hypothesized that high-intensity eccentric training would be more effective for increasing strength than low-intensity eccentric training. Contrary to this, our results show only the ECC80 group significantly increased 1RM when compared to the control group (Fig. 3); although there was also a trend for ECC110 to exceed control (p = 0.065). It is important to note that although only the ECC80 group showed a significant improvement over the control group, the actual difference between the post-testing strength in the two training groups was quite small (0.5 kg). ECC110 increased strength by approximately 4.8% compared to the baseline covariate, whereas ECC80 increased ~7.8%. Two main differences exist between the current study and others comparing high- vs. low-intensity training strength. The current study had participants train eccentrically but then test strength with a concentric 1RM. This was done primarily due to the difficulty of reliably estimating one’s eccentric 1RM with iso-inertial loads and due to the more practical and applied nature of a concentric 1RM. This contrasts with other studies that both trained and tested concentrically (Rana et al. 2008; Mitchell et al. 2012; Schoenfeld et al. 2015). Importantly, other studies that monitored strength utilized training intensities as low as 30% of 1RM (Mitchell et al. 2012), which may not be optimal for increasing muscular strength compared to higher intensities. In the current study, the lowest intensity group (ECC80) trained at 80% of concentric 1RM; an intensity deemed high in conventional training settings and commonly prescribed for increasing strength (Ratamess et al. 2009). This may explain why the low-intensity eccentric training group in the current study (ECC80) was slightly more effective for increasing concentric strength, a finding not consistent with other studies reporting higher intensity training more effective (Mitchell et al. 2012; Schoenfeld et al. 2015).
An important consideration with eccentrically emphasized training is the potential for muscle damage and associated muscle soreness. Intense eccentric training is commonly associated with decreased strength and delayed onset muscle soreness in the first few days after training (Nosaka and Clarkson, 1996; Tokmakidis et al. 2003; Krentz and Farthing, 2010). The current investigation found no significant differences between ECC80 and ECC110 with regard to self-reported muscle soreness. This contrasts with past research where indicators of muscle damage were smaller and recovery was faster with submaximal vs. maximal eccentric loading (Nosaka and Newton 2002). This is likely explained by the fact that the current study had both groups training until failure, while the past study by Nosaka and Newton (2002) had each group perform 3 sets of 10 repetitions, resulting in less total work for the lower intensity group. High-intensity eccentric training has inherent potential to be damaging, but past research supports the idea that eccentric training can be performed safely and with minimal damage (LaStayo et al. 2007). Although the current investigation did not indicate lower intensity training as being more effective for reducing muscle soreness, it is congruent with the idea that well-designed and progressive eccentric training programs of high or low intensities can be well tolerated. Group soreness was elevated during the initial week of training but significantly decreased in the subsequent 2 weeks it was monitored (Fig. 5). The benefits of low intensity eccentric training reported in the current investigation highlight the need for future studies to continue to investigate the relationship between muscle damage, muscle soreness, and varying intensities of eccentric training.
In conclusion, the current study is the first to compare supramaximal- vs. submaximal intensity eccentrically emphasized resistance training and adds to the growing literature focused on the conventional (concentric) training. Although less commonly employed, eccentric training has well-documented advantages for muscle hypertrophy and may be of particular interest and benefit to a subset of clinical populations. The results provide further support and optimism to this idea, reporting for the first time equal increases in muscle hypertrophy after submaximal or supramaximal intensity eccentric training. These results are especially noteworthy considering that lower intensity training was perceived as easier. As a caution, the current study utilized only a single movement (arm curl) and focused on one body joint (elbow flexors). Future studies should seek to replicate and advance these experiments to other muscles groups or include full body investigations. In addition, the current study did not control for training status of the participants which may have influenced potential adaptations between those more or less well trained. Future studies may seek to isolate a particular stratification of the training population to better understand how submaximal and supramaximal eccentric training affect specifically those who are well trained or those who are untrained. Stratification by training experience before randomization may also eliminate the need to use covariate-based analysis as was required in the current study to accommodate for large variation in baseline values between participants. Another notable limitation of the current study was the large number of participant withdrawals. Although time was the most commonly cited reason for withdrawal, eccentric training programs are only truly effective if they are chronically tolerable for those engaging in the training. Future research should continue to monitor the rate of withdrawal when prescribing eccentric training and the pursuit of more accessible, better tolerated eccentric training protocols will continue to be an area of importance. Note that although the results may seem promising for a range of populations, the current study involved only young healthy adults. Future research should seek to extend these results to clinical populations that may benefit from low-intensity eccentric training.
Abbreviations
- ANCOVA:
-
Analysis of covariance
- CON:
-
Concentric
- ECC:
-
Eccentric
- F:
-
Female
- GG:
-
Greenhouse–Geisser
- kg:
-
Kilogram
- M:
-
Male
- MANCOVA:
-
Multiple analysis of covariance
- 1RM:
-
One repetition maximum
- RPE:
-
Ratings of perceived exertion
- VAS:
-
Visual analog scale
References
Abe TD, DeHoyos V, Pollock ML, Garzarella L (2000) Time Course for strength and muscle thickness changes following upper and lower body resistance training in men and women. Eur J Appl Physiol 81:174–180
Alegre LM, Aguado X, Rojas-Martín D, Martín-García M, Ara I, Csapo R (2015) Load-controlled moderate and high-intensity resistance training programs provoke similar strength gains in young women. Muscle Nerve 51:92–101
Burd NA, West DW, Staples AW et al (2010) Low-load high volume resistance exercise stimulates muscle protein synthesis more than high-load low volume resistance exercise in young men. PLoS One 5:e12033
Campos GE, Luecke TJ, Wendeln HK et al (2002) Muscular adaptations in response to three different resistance-training regimens: specificity of repetition maximum training zones. Eur J Appl Physiol 88:50–60
Chestnut JL, Docherty D (1999) The effects of 4 and 10 repetition maximum weight-training protocols on neuromuscular adaptations in untrained men. J Strength Cond Res 13:353–359
Cohen J (1992) A power primer. Psychol Bull 112:155–159
Cureton KJ, Collins MA, Hill DW, McElhannon FM Jr (1988) Muscle hypertrophy in men and women. Med Sci Sports Exerc 20:338–344
Damas F, Phillips S, Vechin FC, Ugrinowitsch C (2015) A review of resistance training-induced changes in skeletal muscle protein synthesis and their contribution to hypertrophy. Sports Med 45:801–807
Day ML, Mcguigan MR, Brice G, Foster C (2004) Monitoring exercise intensity during resistance training using the session RPE scale. J Strength Cond Res 18:353–358
Dibble LE, Hale T, Marcus RL, Droge J, Gerber JP, LaStayo PC (2006) High-intensity resistance training amplifies muscle hypertrophy and functional gains in persons with Parkinson’s disease. Mov Disord 21:1444–1452
Engardt M, Knutsson E, Jonsson M, Sternhag M (1995) Dynamic muscle strength training in stroke patients: effects on knee extension torque, electromyographic activity, and motor function. Arch Phys Med Rehabil 76:419–425
Farthing JP, Chilibeck PD (2003a) The effects of eccentric training at different velocities on cross education. Eur J Appl Physiol 89:570–577
Farthing JP, Chilibeck PD (2003b) The effects of eccentric and concentric training at different velocities on muscle hypertrophy. Eur J Appl Physiol 89:578–586
Farthing JP, Chilibeck PD, Binstead G (2005) Cross-education of arm muscular strength is unidirectional in right-handed individuals. Med Sci Sports Exerc 37:1594–1600
Fisher J, Steele J, Smith D (2013) Evidence-based resistance training recommendations for muscular hypertrophy. Med Sport 17:217–235
Fisher J, Steele J, Smith D (2017) High-and low-load resistance training: interpretation and practical application of current research findings. Sports Med 47:393–400
Foster CJ, Florhaug A, Franklin J, Gottschall L, Hrovatin L, Parker S, Doleshal P, Dodge C (2001) A new approach to monitoring exercise training. J Strength Cond Res 15:109–115
Higbie EJ, Cureton KJ, Warren GL III, Prior BM (1996) Effects of concentric and eccentric training on muscle strength, cross-sectional area, and neural activation. J Appl Physiol 81:2173–2181
Hisaeda H, Miyagawa K, Kuno S, Fukanaga T, Muraoka I (1996) Influence of two different modes of resistance training in female subjects. Ergonomics 39:842–852
Hollander DB, Durand RJ, Trynicki JL, Larock D, Castracane VD, Hebert EP, Kraemer RR (2003) RPE, pain, and physiological adjustment to concentric and eccentric contractions. Med Sci Sports Exerc 35:1017–1025
Holm L, Reitelseder S, Pedersen TG et al (2008) Changes in muscle size and MHC composition in response to resistance exercise with heavy and light loading intensity. J Appl Physiol (1985) 105:1454–1461
Hortobágyi T, Katch FI (1990) Eccentric and concentric torque–velocity relationships during arm flexion and extension. Eur J Appl Physiol 60:395–401
Hortobágyi T, Barrier J, Beard D, Braspennincx J, Koens P, Devita P, Dempsey L, Lambert J (1996) Greater initial adaptations to submaximal muscle lengthening than maximal shortening. J Appl Physiol 81:1677–1682
Jenkins ND, Housh TJ, Buckner SL, Bergstrom HC, Cochrane KC, Hill EC, Smith CM, Schmidt RJ, Johnson GO, Cramer JT (2016) Neuromuscular adaptations after 2 and 4 weeks of 80% versus 30% 1 repetition maximum resistance training to failure. J Strength Cond Res 30:2174–2185
Krentz JR, Farthing JP (2010) Neural and morphological changes in response to a 20-day intense eccentric training protocol. Eur J Appl Physiol 110:333–340
Krentz JR, Quest B, Farthing JP, Quest DW, Chilibeck PD (2008) The effects of ibuprofen on muscle hypertrophy, strength, and soreness during resistance training. Appl Physiol Nutr Metab 33:470–475
LaStayo PC, Reich TE, Urquhart M, Hoppeler H, Lindstedt SL (1999) Chronic eccentric exercise: improvements in muscle strength can occur with little demand for oxygen. Am J Physiol Regul Integr Comp Physiol 276:R611–R615
LaStayo PC, McDonagh P, Lipovic D, Napoles P, Bartolomew A, Esser K, Lindstedt S (2007) Elderly patients and high force resistance exercise- a descriptive report: can an anabolic, muscle growth response occur without muscle damage or inflammation? J Geriatr Phys Ther 30:128–134
Marcus RL, Smith S, Morrell G, Addison O, Dibble LE, Wahoff-Stice D, LaStayo PC (2008) Comparison of combined aerobic and high-force eccentric resistance exercise with aerobic exercise only for people with type 2 diabetes mellitus. Phys Ther 88:1345–1354
McBride JM, McCaulley GO, Cormie P, Nuzzo JL, Cavill MJ, Triplett NT (2009) Comparison of methods to quantify volume during resistance exercise. J Strength Cond Res 23:106–110
McGuigan MR, Foster CF (2004) A new approach to monitoring resistance training. Strength Cond J 26:42–47
McGuigan MR, Egan AD, Foster C (2004) Salivary cortisol responses and perceived exertion during high intensity and low intensity bouts of resistance exercise. J Sports Sci Med 3:8–15
Meyer K, Steiner R, Lastayo P, Lippuner K, Allemann Y, Eberli F, Schmid J, Saner H, Hoppeler H (2003) Eccentric exercise in coronary patients: central hemodynamic and metabolic responses. Med Sci Sports Exerc 35:1076–1082
Mitchell CJ, Churchward-Venne TA, West DW et al (2012) Resistance exercise load does not determine training-mediated hypertrophic gains in young men. J Appl Physiol 113:71–77
Moore DR, Phillips SM, Babraj JA, Smith K, Rennie MJ (2005) Myofibrillar and collagen protein synthesis in human skeletal muscle in young men after maximal shortening and lengthening contractions. Am J Physiol Endocrinol Metab 288:E1153–E1159
Nosaka K, Clarkson PM (1996) Changes in indicators of inflammation after eccentric exercise of the elbow flexors. Med Sci Sports Exerc 28:953–961
Nosaka K, Newton M (2002) Difference in the magnitude of muscle damage between maximal and submaximal eccentric loading. J Strength Cond Res 16:202–208
Ogasawara R, Loenneke JP, Thiebaud RS, Abe T (2013) Low-load bench press training to fatigue results in muscle hypertrophy similar to high-load bench press training. Int J Clin Med 4:114–212
Perri MG, Anton SD, Durning PE, Ketterson TU, Sydeman SJ, Berlant NE, Kanasky WF Jr, Newton RL Jr, Limacher MC, Martin AD (2002) Adherence to exercise prescriptions: effects of prescribing moderate versus higher levels of intensity and frequency. Health Psychol 21:452–458
Rana SR, Chleboun GS, Gilders RM, Hagerman FC, Herman JR, Hikida RS, Kushnick MR, Staron RS, Toma K (2008) Comparison of early phase adaptations for traditional strength and endurance, and low velocity resistance training programs in college-aged women. J Strength Cond Res 22:119–127
Ratamess N, Alvar B, Evetoch T, Housh T, Kibler W, Kraemer W (2009) Progression models in resistance training for healthy adults [ACSM position stand]. Med Sci Sports Exerc 41:687–708
Roig M, Shadgan B, Reid WD (2008) Eccentric exercise in patients with chronic health conditions: a systematic review. Physiother Can 60:146–160
Roig M, O’Brien K, Kirk G et al (2009) The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. B J Sports Med 43:556–568
Rooyackers JM, Berkeljon DA, Folgering HTM (2003) Eccentric exercise training in patients with chronic obstructive pulmonary disease. Int J Rehab Res 26:47–49
Sale DG, MacDougall JD, Always SE, Sutton JR (1987) Voluntary strength and muscle characteristics in untrained men and women and male bodybuilders. J Appl Physiol 62:1786–1793
Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT (2015) Effects of low-vs. high-load resistance training on muscle strength and hypertrophy in well-trained men. J Strength Cond Res 29:2954–2963
Schoenfeld BJ, Wilson JM, Lowery RP, Krieger JW (2016) Muscular adaptations in low-versus high-load resistance training: a meta-analysis. Eur J Sport Sci 16:1–10
Schuenke MD, Herman JR, Gliders RM et al (2012) Early-phase muscular adaptations in response to slow-speed versus traditional resistance-training regimens. Eur J Appl Physiol 112:3585–3595
Seger J, Arvidsson B, Thorstensson A (1998) Specific effects of eccentric and concentric training on muscle strength and morphology in humans. Eur J Appl Physiol 79:49–57
Shepstone TN, Tang JE, Dallaire S, Schuenke MD, Staron RS, Phillips SM (2005) Short-term high-vs. low-velocity isokinetic lengthening training results in greater hypertrophy of the elbow flexors in young men. J Appl Physiol 98:1768–1776
Staron RS, Karapondo DL, Kraemer WJ, Fry AC, Gordon SE, Falkel JE, Hagerman FC, Hakida RS (1994) Skeletal muscle adaptation during early phase of heavy-resistance training in men and women. J Appl Physiol 76:1247–1255
Steiner R, Meyer K, Lippuner K, Schmid JP, Saner H, Hoppeler H (2004) Eccentric endurance training in subjects with coronary artery disease: a novel exercise paradigm in cardiac rehabilitation? Eur J Appl Physiol 91:572–578
Sweet TW, Foster C, McGuigan MR, Brice G (2004) Quantification of resistance training using the session RPE method. J Strength Cond Res 18:796–802
Tanimoto M, Ishii N (2006) Effects of low-intensity resistance exercise with slow movement and tonic force generation on muscular function in young men. J Appl Physiol 100:1150–1157
Tokmakidis SP, Kokkinidis EA, Smilios I, Douda H (2003) The effects of ibuprofen on delayed muscle soreness and muscular performance after eccentric exercise. J Strength Cond Res 17:53–59
Westing HS, Seger JY, Thorstensson A (1990) Effects of electrical stimulation on eccentric and concentric torque-velocity relationships during knee extension in man. Acta Physiol Scand 140:17–22
Westing HS, Cresswell AG, Thorstensson A (1991) Muscle activation during maximal voluntary eccentric and concentric knee extension. Eur J Appl Physiol 62:104–108
Williams MA, Haskell WL, Ades PA, Amsterdam EA, Bittner V, Franklin BA, Gulanick M, Laing ST, Stewart KJ (2007) Resistance exercise in individuals with and without cardiovascular disease. Circulation 116:572–584
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by William J. Kraemer.
Rights and permissions
About this article

Cite this article
Krentz, J.R., Chilibeck, P.D. & Farthing, J.P. The effects of supramaximal versus submaximal intensity eccentric training when performed until volitional fatigue. Eur J Appl Physiol 117, 2099–2108 (2017). https://doi.org/10.1007/s00421-017-3700-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-017-3700-3