
Abstract
Purpose
Changes in elbow flexion torque and biceps brachii electromyogram (EMG) activity over 30 repetitive maximal voluntary concentric-only (CON-only), eccentric-only (ECC-only), and alternative concentric and eccentric (CON-ECC, 30 concentric + 30 eccentric) contractions were examined to compare their muscle fatigue profiles.
Methods
Fifteen healthy young men performed CON-only, ECC-only and CON-ECC in their maximal effort between 10° and 100° elbow flexion on an isokinetic dynamometer at an angular velocity of 30°/s with a 3-s rest between contractions in a randomised order with ≥ 3 days between conditions. Changes in torque and EMG over the repeated contractions and maximal voluntary isometric contraction (MVC-ISO) torque with EMG before the first contraction and immediately after the last contraction were compared among conditions by two-way repeated measures analysis of variance.
Results
The torque decreased (p < 0.01) from the first to 30th contraction in CON-only (− 49.5 ± 11.0%), ECC-only (− 32.2 ± 7.4%), and concentric (− 62.3 ± 8.7%) as well as eccentric phase (− 58.9 ± 9.3%) in CON-ECC (− 46.0 ± 12.3% overall). The magnitude of the decrease in the torque was greater (p < 0.01) for the CON-only than ECC-only, and the concentric than an eccentric phase in the CON-ECC. However, MVC-ISO torque decreased (p < 0.01) similarly after CON-only (− 42.9 ± 13.8%) and ECC-only (− 40.1 ± 9.2%), which was smaller (p < 0.01) than CON-ECC (− 56.8 ± 9.2%). EMG over contractions decreased (p < 0.01) for all conditions similarly from the first to the last contraction (− 28.5 ± 26.8%), and EMG in MVC-ISO also decreased similarly for all conditions (− 24.7 ± 35.8%).
Conclusion
These results suggest greater fatigue resistance in repetitive maximal eccentric than concentric contractions, but the fatigue assessed by MVC-ISO does not show it.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
General or conventional resistance exercises consist of concentric (shortening) and eccentric (lengthening) muscle contractions. However, resistance exercises in which the load for the concentric phase is eliminated or the load for the eccentric phase is increased to emphasise the eccentric contractions are also often performed. The use of eccentric-only and/or accentuated eccentric contractions in resistance exercises has been increasing (Roig et al. 2009; Čretnik et al. 2022). This is due to possible greater training effects generated by eccentric than concentric contractions (Sato et al. 2022a, b; Chen et al. 2017; Tseng et al. 2020). Roig et al. (2009) stated that resistance exercise training with eccentric contractions was more effective for increasing overall muscle strength than concentric contractions, which was associated with greater mechanical loads imposed on muscles during eccentric than concentric contractions. The advantages of eccentric over concentric contractions also stem from the greater muscle force generation capability and less energy requirement or less neuromuscular fatigue in eccentric contractions (Peñailillo et al. 2013; Shibata et al. 2023; Tesch et al. 1990).
Regarding the greater muscle force generation capability, Hollander et al. (2007) reported that one-repetition maximum (1-RM) of the overhead press, lat pull down, leg press, bench press, knee extension, and leg curl was 20–50% greater in eccentric than concentric exercises. Other studies have also reported 22–49% greater force generation capacity for eccentric than concentric contraction of the elbow flexors (Doss and Karpovich 1965) and extensors (Hortobágyi and Katch 1990), knee flexors and extensors (Wu et al. 1997), plantar flexors (Baudry et al. 2007) and dorsi flexors (Pasquet et al. 2000). The greater force generation capability in eccentric than concentric contraction is believed to be originated predominantly from the structural protein titin, which provides passive force (Herzog 2014).
In terms of less energy requirement or less neuromuscular fatigue in eccentric than concentric contractions, Peñailillo et al. (2013) showed that eccentric cycling consumed 50% less oxygen than concentric cycling for the same workload. Pasquet et al. (2000) showed that the rate of torque reduction over 30 consecutive maximal contractions of the ankle dorsiflexors at the angular velocity of 50°/s was significantly smaller in eccentric-only (− 23.8%) than in concentric-only contractions (− 31.6%). Kay et al. (2000) reported a 42.3% decrease in MVC torque of the knee extensors over concentric-only contractions but no decrease in the torque over eccentric-only contractions when they were performed for 100 s for a 78° range of motion performed on an isokinetic dynamometer at an angular velocity of 60°/s. Additionary, Nuzzo and Nosaka (2022) reported that the maximal voluntary contraction (MVC) of concentric and eccentric torque of the elbow flexors decreased significantly less for eccentric (− 55.3%) than concentric phase (− 77.9%) over 25 maximal alternative concentric-eccentric contractions. Moreover, Shibata et al. (2023) have recently demonstrated that the repetitions to failure (RF) was 1.6–2.7 times greater in eccentric-only than concentric-only contractions in arm curl exercise at 70%, 80%, 90% and 95% of respective one-repetition maximum load. In conventional resistance exercises and many of our locomotions, concentric and eccentric contractions are performed alternatively. Thus, it is also important to examine changes in force generation capacity over repetitive concentric-eccentric contractions. Although Ruas et al. (2022) compared concentric-eccentric contractions and eccentric-only contractions for the knee extensors, no previous study has compared concentric-eccentric, eccentric-only and concentric-only contractions for fatigability over repetitive maximal contractions of the elbow flexors.
Some studies showed that changes in maximal voluntary isometric contraction (MVC-ISO) strength and/or force generated by electrical stimulation from immediately before to immediately after exercise were similar between eccentric and concentric contractions. For example, Royer et al. (2022) reported that MVC-ISO torque immediately post-exercise decreased similarly after repeated concentric-only (− 21.7 ± 11.5%) and eccentric-only contractions (− 26.2 ± 15.6%) of the knee extensors when the torque-time integral of the exercise was matched. It should be noted that the total number of muscle contractions was approximately 40% greater for the concentric (135.5 ± 22.5) than for eccentric exercise (96.4 ± 15.5) in the study. Pasquet et al. (2000) showed no significant difference in MVC-ISO torque reduction between concentric-only (− 37.4%) and eccentric-only contractions (− 33.8%) of the dorsiflexors immediately after 5 sets of 30 maximum voluntary contractions, although the force in the repeated contractions decreased greater for concentric (− 31.6%) than eccentric contractions (− 23.8%). Ruas et al. (2022) compared eccentric-only (6 sets of 8 eccentric contractions at 80% of eccentric one-repetition maximum) and coupled concentric and eccentric contractions (6 sets of 8 alternating concentric and eccentric contractions at 80% of concentric one-repetition maximum and eccentric one-repetition maximum, respectively) of the knee extensors for changes in MVC-ISO force, resting twitch force, maximal M-wave, voluntary activation, motor evoked potentials, corticospinal silent period, and short interval intracortical inhibition. They found no significant differences between the eccentric-only and concentric-eccentric protocols for the changes in the variables after exercise. It is possible that the muscle fatigue profile is not much different between concentric-only, eccentric-only, and concentric-eccentric contractions when it is assessed by MVC-ISO torque at immediately post-exercise; but no previous study has systematically investigated this.
In the study by Kay et al. (2000) mentioned above, they reported no significant changes in surface electromyography (EMG) activity during in both concentric-only and eccentric-only contractions, in spite of the different fatigue profiles in the strength. In contrast, Pasquet et al. (2000) reported greater decreases in the tibialis anterior EMG activity for the concentric-only (− 26.4%) than eccentric-only task (− 17.5%) in the study mentioned above. They also showed that neither the interpolated-twitch response nor the ratio of the voluntary EMG to the amplitude of the compound muscle action potential (M-wave) changed in both tasks, but decreases in the contractile properties in response to single and paired electrical stimuli, as well as the interpolated-twitch method and postactivation potentiation were greater after the concentric-only than eccentric-only contractions. They concluded that the greater alterations in the contractile properties observed during the concentric-only contractions were possibly associated with a higher energy requirement in concentric than eccentric contractions. To the best of our knowledge, no previous study has compared maximal concentric-only, eccentric-only, and concentric-eccentric contractions for changes in the force generation capacity over repeated contractions as well as MVC-ISO torque before and after the repeated contractions.
Therefore, the present study examined changes in eccentric and concentric torque of the elbow flexors and biceps brachii EMG over 30 maximal repetitive concentric-only, eccentric-only, and concentric-eccentric (60 in total) contractions, and changes in the elbow flexor MVC-ISO torque and EMG before and immediately after the task to clarify the muscle fatigue profile. We hypothesised that the toque produced in the eccentric-only contractions and eccentric phase in the concentric-eccentric contractions would be greater than that produced in the concentric-only contractions and concentric phase in the concentric-eccentric contractions, respectively. However, the rate of the torque reduction in eccentric-only contractions would be smaller than that in concentric-only contractions, but the magnitude of decrease in MVC-ISO torque from pre- to post-exercise would be similar between them. In concentric-eccentric contractions, the torque would be decreased greater for the concentric than an eccentric phase, and the decrease in the MVC-ISO would be greater when compared with the concentric-only and eccentric-only conditions. Regarding EMG, we hypothesised that EMG activity would decrease less over eccentric-only than concentric-only contractions, and the decrease would be greater for concentric-eccentric condition than the other two conditions. In addition, the EMG in MVC-ISO torque measure would decrease greater after concentric-eccentric than the other two conditions, but the concentric-only and eccentric-only would show a similar decrease.
Methods
Participants and study design
The sample size was estimated from the study by Pasquet et al. (2000) who showed a significantly smaller rate of torque reduction over 30 repetitive maximal eccentric (− 23.8%) than concentric contractions (− 31.6%) of the ankle dorsiflexors. The effect size was considered to be large (dZ = 0.8), thus with an alpha value of 0.05 and a power (1−β) of 0.8, the sample size was estimated to be 12 participants for the difference between eccentric-only and concentric-only for matched pairs (G*Power 3.1, Germany). In the present study, the same participants performed concentric-only (CON-only), eccentric-only (ECC-only), and concentric-eccentric (CON-ECC) contractions of the elbow flexors on different days in a randomised order. Thus, we recruited 15 participants, considering the estimation error for the comparison of the three conditions, and possible dropouts in the study.
The participants were male university students with the average ± SD age, height and body mass being 22.1 ± 3.5 years, 171.6 ± 4.5 cm, and 71.5 ± 9.8 kg, respectively. They had a resistance training experience of at least six months prior to the present study. All participants were briefed on the study's purpose and procedures, and written consent was obtained from each participant. This study was approved by the Ethics Committee of Niigata University of Health and Welfare (#18202).
All participants performed a familiarisation session in which three maximal isometric, concentric-only, eccentric-only, and concentric-eccentric contractions of elbow flexors were performed. One week after the familiarisation session, the participants completed three fatigue tasks (CON-only, ECC-only, CON-ECC) over three weeks in a randomised order. Considering the effect of possible muscle damage induced by maximal eccentric contractions, at least one week was inserted after ECC-only or CON-ECC, but at least three days were inserted after CON-only. In the CON-only or ECC-only conditions, 30 maximal concentric or eccentric contractions were performed, and in the CON-ECC condition, 30 maximal alternative concentric-eccentric contractions were performed, thus the total number of contractions was 60. Over the 30 or 60 maximal contractions of the elbow flexors, elbow flexion torque and biceps brachii muscle activity were recorded. Before and immediately after each task, maximal voluntary isometric contraction (MVC-ISO) torque of the elbow flexors and muscle activity of the biceps brachii during the MVC-ISO were measured.
Muscle fatigue task
All participants performed the three fatiguing tasks with their dominant arms on an isokinetic dynamometer (Biodex System 3.0, Biodex Medical Systems Inc., Shirley, NY, USA) for the CON-only and ECC-only or CON-ECC conditions. During the tasks, the arm was positioned in front of the body on padded support adjusted to 45°of shoulder flexion, and the forearm was kept supinated with the wrist placed against the lever arm of the dynamometer. The range of motion was 90° for all exercises, and the starting angle was 10° for CON-only and CON-ECC conditions, and 100° elbow flexion for ECC-only condition, where the fully extended elbow joint was defined as 0°. For all tasks, the angular velocity was 30°/s based on our previous studies (Sato et al. 2022b; Yoshida et al. 2022), thus each muscle contraction was 3 s.
In the CON-only condition, each participant was instructed to perform maximal concentric contractions from 10º to 100º of elbow flexion, and the arm was returned to the starting angle (10º elbow flexion) passively over a period of 3 s. For the ECC-only condition, each participant was instructed to perform maximal eccentric contractions from 100º to 10º of elbow flexion; the arm was returned to the starting angle (100º elbow flexion) passively over a period of 3 s. In the CON-ECC condition, a maximal concentric contraction from 10° to 100° elbow flexion was followed by a maximal eccentric contraction from 100° to 10° elbow flexion. This was repeated 30 times with a 3-s rest period between contractions, thus the total number of muscle contractions was 60. Participants were verbally encouraged to generate maximal force for the entire range of motion. The force of each contraction was displayed computer screen to provide feedback and a target to motivate the participant to generate as high a force as possible. The peak torque in each contraction during the fatigue tasks occurred between 40° and 70° of elbow flexion for all conditions.
Elbow flexor torque during the repeated contractions was recorded via an analog-to-digital converter (PowerLab 8/30, AD Instruments, Colorado Springs, CO, USA) to a personal computer with analysis software (LabChart 7, AD Instruments). Biceps brachii muscle activity was recorded using surface electromyography during the repeated muscle contraction tasks with torque data. The electrodes were placed in the distal two-thirds from the acromion to the lateral epicondyle of the humerus. Using a surface electrode with a distance of 2.0 cm between the centre of the electrodes, EMG activities were recorded via a preamplifier (FA-DL-720-140: Four Assist, Japan) and AD converter (PowerLab, ADinstrument, Australia) to a personal computer (DESKTOP-CRVN2SU, MouseComputer Co., Ltd., Japan). The band-pass filter was set from 20 to 500 Hz, and full-wave rectified EMG waveforms were analysed by the software (LabChart 8.1.14: AD instrument, Australia). A mean EMG root mean square (RMS) value was computed for each during a time window equivalent to the amount of time needed to complete the range of motion (i.e., 3 s) of the muscle fatigue task. For EMG during muscle fatigue, the average value for the same range of motion (i.e., 40° to 70° of elbow flexion) was used for all conditions. In the MVC-ISO torque measures, EMG in a 50-ms slot before and after a peak torque was analysed. Changes in EMG over 30 contractions were normalised to the EMG of the first contraction.
Maximum voluntary isometric contraction (MVC-ISO)
After a standardized warm-up protocol consisting of one 3-s submaximal voluntary contraction at 60% of MVC-ISO, participants performed two MVC-ISO at an elbow joint angle of 90° (0° = full elbow extension) on the dynamometer, interspaced by 1-min rest before the fatigue task. The highest peak torque in 3 s MVC-ISO measurement from each MVC-ISO torque measure, the larger value of the two measures, was used for further analysis. Immediately after the fatigue task, only MVC-ISO measurement was taken within 3 s after the 30th contraction for the CON-only and ECC-only, and 60th contraction for the CON-ECC condition. EMG during MVC-ISO measurement was recorded in the same way as that described above for the EMG during repetitive contractions. The average value of 50 ms before and after the peak torque during MVC-ISO measurement was analysed for RMS and used for further analyses.
Statistical analyses
Statistical analyses were performed using the SPSS version 28.0 (IBM Japan, Inc., Tokyo, Japan). The normality of the data was checked by a Shapiro–Wilk test. The baseline measures were compared among the three tasks using a one-way analysis of variance (ANOVA). A repeated two-way ANOVA with two factors (conditions x repetitions) was used to compare the changes in peak torque and EMG over 30 contractions among CON-only, ECC-only, CON-ECC-CON, and CON-ECC-ECC. We calculated the average values of MVC torque during the muscle fatigue task in every 10 contractions, which were compared between conditions by Bonferroni comparisons. In addition, a two-way repeated measures ANOVA was used to compare the changes in MVC-ISO torque and EMG among CON-only, ECC-only, and CON-ECC conditions. Moreover, percentage changes in MVC-ISO torque from baseline to post-exercise were compared between groups in Bonferroni comparisons. Effect size (ES) was calculated as a difference in the mean values between pre- and post-training divided by the pooled SD. ES of 0.00–0.19 was considered trivial, 0.20–0.49 was small, 0.50–0.79 was moderate, and ≥ 0.80 was large (Cohen 2013). The differences were considered statistically significant at an alpha level of 0.05. Descriptive data are shown as mean ± SD.
Results
Changes in torque over maximal contractions
All participants completed the three muscle fatigue tasks. Figure 1 shows the average (± SD) changes in torque of 15 participants over 30 maximal contractions (in CON-ECC, 30 CON, and 30 ECC contractions). The torque produced in the first contraction was 7.2–38.5% (average ± SD of 15 participants: 27.0 ± 8.9%) greater for ECC-only (70.6 ± 10.2 Nm) than for CON-only contraction (50.5 ± 6.9 Nm). The total torque produced over the 30 contractions was also 27.7–47.8% (39.0 ± 6.3%) greater for ECC-only than CON-only condition. In the CON-ECC, the torque produced in the eccentric phase was 31.6 ± 11.8% greater for the first contraction as well as the rest of the contractions (e.g., 10th contraction: 66.6 ± 28.3%, 20th contraction: 56.2 ± 29.8%, 30th contraction: 45.6 ± 27.8%) when compared with the concentric phase. The sum of the maximum torque generated during the repeated contractions was greater (p < 0.01) for ECC-only (4986.7 ± 768.0 Nm s) than CON-only (3048.5 ± 534.3 Nm s) and for CON-ECC (5646.0 ± 989.2 Nm s) than ECC-only (p < 0.01), because of the inclusion of eccentric and concentric contractions. The sum of the maximum torque in the eccentric phase of CON-ECC (3425.6 ± 636.5 Nm s) was greater (p < 01) than that in the concentric phase in CON-ECC (2220.3 ± 386.6 Nm s).

Changes in elbow flexor torque (mean ± SD of 15 participants) over 30 maximal voluntary concentric only (CON-only), eccentric only (ECC-only), and alternating concentric and eccentric (CON-ECC) eccentric contractions. For the CON-ECC, the torque in the concentric phase (CON phase) and that in the eccentric phase (ECC pase) over 30 contractions each are shown
The one-way ANOVA showed that the decreases in the torque over repetitive contractions were significant for the ECC-only [F (29, 406) = 60.0, p < 0.01, ηp2 = 0.81], CON-only [F (29, 406) = 119.1, p < 0.01, ηp2 = 0.89], and ECC torque [F (29, 406) = 100.9, p < 0.01, ηp2 = 0.87] as well as CON torque in the ECC-CON [F (29, 406) = 111.8, p < 0.01, ηp2 = 0.88]. The two-way repeated ANOVA showed a significant interaction effect for changes in the torque [F (87, 1624) = 7.974, p < 0.01, ηp2 = 0.299]. The magnitude of the decrease in the torque over 30 maximal contractions was greater (p < 0.01) for the CON-only (− 49.5 ± 11.0%) than the ECC-only (− 32.2 ± 7.4%), and ECC torque (− 58.9 ± 9.3%) than CON torque in the ECC-CON (− 62.3 ± 8.7%) as shown in Fig. 2. When looking at the changes in MVC torque every 10 contractions, the rate of torque reduction from 1st to 10th was smaller (p < 0.01) for ECC-only than CON-only and ECC than CON in CON-ECC. This was also the case for the change from 11 to 20th contractions. Additionally, the first 15 contractions in the ECC-CON condition (30 contractions in total) showed a greater (p < 0.01) decrease in the ECC (− 47.2 ± 11.0%) and CON torque (− 57.7 ± 8.9%), when compared with the ECC-only condition (− 32.2 ± 7.4%). The magnitude of decrease in the CON torque in the first 15 contractions in the CON-ECC (− 57.7 ± 8.9%) was greater (p < 0.01) than in the CON-only condition (− 49.5 ± 11.0%).

Rate of torque decrease (mean ± SD of 15 participants) from the first to 30th contraction (1–30), the first to 10th contraction (1–10), 11th–20th contraction (11–20) and 21st–30th contraction for concentric only (CON-only), eccentric only (ECC-only), and alternating concentric and eccentric (CON-ECC) eccentric contractions. For the CON-ECC, the torque in the concentric phase (CON phase) and that in the eccentric phase (ECC pase) are shown. *: Significantly (p < 0.05) different from the 1–10, #: Significantly (p < 0.05) different from CON-only, §: Significantly (p < 0.05) different from ECC-only, †: Significantly (p < 0.05) different from CON-ECC-CON
Changes in EMG
EMG activity of the first contraction was not significantly different between CON-only (479.2 ± 227.7 mV) and ECC-only (451.5 ± 181.1 mV), as well as concentric phase (424.1 ± 195.8 mV) and eccentric phase (561.6 ± 316.6 mV) in CON-ECC. Figure 3 shows normalised changes in EMG activity from that of the first contraction (100%) over 30 contractions for the ECC-only, CON-only, and ECC and CON phases in the CON-ECC conditions. The two-way ANOVA showed a main effect of time [F (29, 1421) = 17.34, p < 0.01, ηp2 = 0.261] but no interaction effect [F (29, 1421) = 0.986, p = 0.519, ηp2 = 0.261]. As shown in Fig. 4, EMG decreased from 1st to 30th contraction in CON-only (− 29.4 ± 24.9%), ECC-only (− 14.4 ± 25.9%), ECC-CON-CON (− 31.3 ± 27.1%) and ECC-CON-ECC (− 37.8 ± 23.9%) similarly. When looking at the changes in EMG every 10 contractions, no significant difference was evident between the first to 10th, 11th to 20th, and 21st to 30th contraction for any of the conditions.

Normalised changes (mean ± SD of 15 participants) in biceps brachii electromyographic (EMG) activity from the first contraction (100%) over 30 maximal voluntary concentric only (CON-only), eccentric only (ECC-only), and alternating concentric and eccentric (CON-ECC) eccentric contractions. For the CON-ECC, the torque in the concentric phase (CON phase) and that in the eccentric phase (ECC phase) over 30 contractions each are shown

Rate of biceps brachii electromyographic (EMG) activity change (mean ± SD of 15 participants) from the first to 30th contraction (1–30), the first to 10th contraction (1–10), 11th–20th contraction (11–20) and 21st–30th contraction for concentric only (CON-only), eccentric only (ECC-only), and alternating concentric and eccentric (CON-ECC) eccentric contractions. For the CON-ECC, the torque in the concentric phase (CON-ECC-CON) and that in the eccentric phase (CON-ECC-ECC) are shown. *: Significant (p < 0.05) decrease, #: Significantly (p < 0.05) different from CON-only
Changes in MVC-ISO torque and EMG in MVC-ISO torque measurement
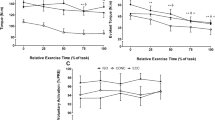
Changes in MVC-ISO torque and EMG before and after the fatigue task are shown in Fig. 5. No significant difference in MVC-ISO torque was found for the pre-exercise values (ECC-only: 65.9 ± 11.2 Nm, CON-only: 63.4 ± 10.9 Nm, CON-ECC: 64.1 ± 13.0 Nm). A significant interaction effect was evident for changes in MVC-ISO torque [F (2, 42) = 7.66, p < 0.01, ηp2 = 0.267]. Significant decreases in MVC-ISO torque were found for the ECC-only (− 40.7 ± 9.9%), CON-only (− 43.6 ± 14.2%), and CON-ECC (− 58.3 ± 7.9%) conditions (p < 0.01), but the decrease was greater (p < 0.01) for the CON-ECC than ECC-only and CON-only conditions without a significant difference between ECC-only and CON-only.

Changes (mean ± SD of 15 participants and their individual values) in maximal voluntary isometric contraction (MVC-ISO) torque (A) and normalised changes (PRE: 100%) in biceps brachii electromyographic (EMG) activity (B) before (PRE) and immediately after (POST) 30 maximal voluntary concentric only (CON-only), eccentric only (ECC-only), and alternating concentric and eccentric (CON-ECC) eccentric contractions. The change from PRE to POST is also shown for each graph. *: Significantly (p < 0.05) different from PRE, #: Significantly (p < 0.05) different from CON-only and ECC-only
Regarding EMG, no significant difference in the pre-exercise MVC-ISO torque measures was found between ECC-only (591.1 ± 274.7 mV), CON-only (586.9 ± 299.2 mV), and CON-ECC (646.7 ± 322.2 mV). The two-way repeated measures ANOVA showed no significant interaction effect [F (2, 39) = 2.72, p = 0.079, ηp2 = 0.122] but a main effect of time [F (2, 39) = 38.9, p < 0.01, ηp2 = 0.50]. In Fig. 5B, normalised changes in EMG activity from the pre-exercise (100%) to post-exercise are shown. The magnitude of decrease was − 22.5 ± 18.7% for the ECC-only, − 35.7 ± 25.3% for the CON-only, and − 48.3 ± 5.7% for the CON-ECC condition, without significant difference between conditions.
When comparing the magnitude of decrease in MVC torque from the first to 30th contraction shown in Fig. 2 and that of MVC-ISO torque from before to immediately after the 30th contraction for each condition, no significant difference was found for the CON-only (− 49.5 ± 11.0% vs. − 42.9 ± 13.8%) and CON-ECC (− 58.3 ± 7.9% vs. − 56.8 ± 9.2%) conditions. However, in the ECC-only condition, the decrease in MVC-ISO torque (− 40.7 ± 9.9%) was greater (p < 0.01) than the decrease over 30 eccentric contractions (− 32.2 ± 7.4%).
Discussion
The results showed that the torque produced in ECC contractions was approximately 40% greater than that in CON contractions (Fig. 1). The elbow flexor torque over 30 maximal contractions decreased less in ECC-only than CON-only, and in ECC than CON phase in the CON-ECC (Figs. 1 and 2). However, the magnitude of decrease in MVC-ISO torque from before to after the fatigue task was similar between ECC-only and CON-only, but it was smaller than that of CON-ECC condition (Fig. 5). The EMG decreased similarly among the conditions (Figs. 3 and 4), and the EMG during MVC-ISO torque also decreased similarly among the conditions. These results were almost in line with the hypotheses, but some discrepancies to the hypotheses were found as discussed below.
Force generation profile
The maximal torque produced in the first contraction in the ECC-only (70.6 ± 10.2 Nm) and eccentric phase in the CON-ECC (64.1 ± 10.8 Nm) were 40.3 ± 16.2% and 31.6 ± 11.7% greater than that in the CON-only (50.5 ± 6.9 Nm) and concentric phase in the CON-ECC (48.9 ± 8.3 Nm), respectively (Fig. 1). The MVC-ISO torque measured immediately before the fatigue task was 63.4 ± 12.0 Nm on average of the three conditions. Hortobágyi and Katch (1990) reported that MVC-ECC torque was 13.3–22.5% greater than MVC-ISO torque and 43.8–53.5% greater than MVC-CON torque for the elbow flexors. More recently, Sato et al. (2022b) showed that MVC-ECC torque was 37.8 ± 4.2% and 55.2 ± 3.7% greater than MVC-ISO torque and MVC-CON torque, repetitively for the elbow flexors. Thus, the results of the present study were comparable to those of the previous studies.
It is important to note that the greater torque in ECC than CON was still observed at 30th contraction such that MVC torque was 94.9 ± 42.3% greater in ECC-only than CON-only condition, and 28.5 ± 15.2% greater in the eccentric than a concentric phase in the CON-ECC condition (Fig. 1). This suggests that greater force generation capacity in eccentric than concentric contractions is preserved or even magnified in fatigued muscle. The greater maximum force generation capability in eccentric than isometric or concentric contraction has been explained to be due to the elastic structure within muscle fibres and in muscle–tendon complex (Herzog 2018). Titin that spans the half-sarcomere from Z-disk to M-band could add force to that already produced by the activated muscle fibres (Guilhem et al. 2010; Fürst et al. 1988). During eccentric contractions, the external mechanical load exerted on the solicited muscle triggers a stretching of the elastic recoil of the muscle–tendon complex system, which could contribute to additional force (Abbott et al. 1952). As discussed below, it is important to note that the mechanisms underpinning the greater force production capability in eccentric than concentric contractions are maintained in repetitive contractions.
Muscle fatiguability
The changes in the torque over 30 maximal contractions were smaller for ECC-only (− 32.2%) than CON-only (− 49.5%), and eccentric phase (− 58.9%) than concentric phase (− 62.3%) in CON-ECC (Figs. 1 and 2). Less fatiguability in eccentric than concentric contractions has been shown in previous studies (Pasquet et al. 2000; Kay et al. 2000; Souron et al. 2018; Royer et al. 2022; Nuzzo and Nosaka 2022). For example, Nuzzo and Nosaka (2022) reported that the MVC torque of the elbow flexors decreased significantly greater for concentric (− 77.9%) than for eccentric phase (− 55.3%) over 25 maximal CON-ECC contractions. Pasquet et al. (2000) showed that the rate of torque decrease over 30 consecutive maximal isokinetic (angular velocity: 50°/s) contractions of the ankle dorsiflexors was smaller in ECC-only (− 23.8%) than in CON-only contractions (− 31.6%). Furthermore, Kay et al. (2000) reported a 42.3% decrease in MVC torque of the knee extensors over CON-only contractions but no significant decrease in the torque over ECC-only contractions when they were performed over 100 s at 78° range of motion on an isokinetic dynamometer at an angular velocity of 60°/s. It was suggested that the elastic component of muscle and connective tissue contributed to minimising the force loss during repetitive eccentric contractions (Kay et al. 2000; Pasquet et al. 2000). In contrast, Beck et al. (2012) and Ye et al. (2014) reported no significant differences between CON-only and ECC-only contractions of the elbow flexors over 60 maximal repetitions. In their studies, 10 consecutive contractions were followed by a rest period of 1 or 2 min. Thus, it is possible that the rest attenuated fatiguability, especially in the concentric contractions. In fact, Pasquet et al. (2000) showed that a decrease in force over 150 maximal concentric contractions of the ankle dorsiflexors returned to the baseline level after one minute of rest. Since no rest was inserted over 30 contractions in the present study and the previous studies (Pasquet et al. 2000; Souron et al. 2018), it seems reasonable to conclude that eccentric contractions are less fatigable than concentric contractions.
It has been reported that metabolic demand and activation of motor units are lower in eccentric than concentric contractions (Kossev and Christova 1998). Peñailillo et al. (2013) reported 50% less oxygen uptake and 30% less heart rate during eccentric than concentric cycling in the same work. In a classic paper, Huxley (1957) stated that the actin-myosin links were not broken by the reversal of reaction that does not involve the splitting of a high-enrergy phosphate bands. Ryschon et al. (1997) compared concentric, eccentric, and isometric contractions of the ankle dorsiflexors to estimate ATP utilisation using P-nuclear magnetic resonance imaging and reported that the ATP production rate/work was 15.0% in concentric and 34.7% in eccentric contractions. They speculated that the higher mechanochemical efficiency of eccentric than concentric contractions was due to an alteration of the actino-myosin-ATP stoichiometry, which lowers the requirement of ATP (Ryschon et al. 1997). Therefore, less fatigue in eccentric than concentric contractions is likely due to the reduced consumption of ATP in eccentric contractions. Additionally, titin is involved in the force regulation in eccentric contraction as discussed above. Joumaa et al. (2008) showed in rabbit psoas muscle that the calcium-dependent increase in eccentric force in myofibrils that were stripped of troponin C was abolished when titin was removed by trypsin. This suggests that titin also makes eccentric contractions less fatigable than concentric contractions.
It should be noted that the magnitude of decrease in MVC-ISO torque was not significantly different between ECC-only and CON-only (Fig. 5), in spite of the significantly smaller decreases in torque over 30 contractions in ECC-only than CON-only (Figs. 1 and 2). Pasquet et al. (2000) also showed no significant difference in MVC-ISO torque reduction between CON-only (− 37.4%) and ECC-only (− 33.8%) contractions of the dorsiflexor muscles when they found smaller torque reduction over 30 consecutive maximal contractions in eccentric-only (− 23.8%) than in concentric-only contractions (− 31.6%). It is important that the changes in MVC-ISO torque or force before and after repetitive maximal dynamic contractions do not necessarily reflect the difference in fatiguability observed during the dynamic contractions. Enoka and Duchateau (2008) stated; “muscle fatigue is not the point of task failure or the moment when the muscles become exhausted, rather muscle fatigue is a decrease in the maximal force or power that the involved muscles can produce, and it develops gradually soon after the onset of the sustained physical activity. A common protocol used to quantify the development of muscle fatigue is to interrupt the fatiguing exercise with brief maximal contractions (voluntary or electrically evoked) to estimate the decline in the maximal force capacity.” Thus, the decrease in MVC-ISO torque after the repetitive maximal contractions appears to indicate “muscle fatigue.” In this sense, no difference between concentric-only and eccentric-only contractions could indicate no difference in muscle fatigue. However, as discussed above, there were distinct differences in the rate of torque decline over 30 repetitions between concentric-only and eccentric-only contractions (Figs. 1 and 2). It is interesting to examine changes in maximal voluntary concentric and eccentric contraction torque before and after ECC-only and CON-only repetitive contractions, respectively. It may be that MVC assessments with different modes of muscle contraction provide different neuromuscular fatigue profiles, which could shed light on the mechanism underpinning muscle contraction type-specific fatigue or fatiguability.
EMG profile
Despite the differences in MVC torque and MVC-ISO torque changes between ECC-only and CON-only contractions, no significant difference between the two was evident for the changes in EMG activity over 30 contractions (Figs. 3 and 4). When comparing the magnitude of decrease between the torque and EMG, both ECC-only (torque: − 32.2%, EMG: − 14.4%) and CON-only (− 49.5%, − 29.4%) showed greater decreases in torque than EMG. Enoka (1996) stated in his review article that the magnitude of the muscle activation indicated by EMG during a maximum eccentric contraction was much less than that recorded during a maximum concentric contraction. Kellis and Baltzopoulos (1996) reported that vastus lateralis EMG amplitudes during maximal eccentric isokinetic knee extensor contractions at different velocities were 11–52% lower than during concentric contractions. Pasquet et al. (2000) showed a greater reduction in EMG in concentric-only contractions of the dorsiflexors (− 26.4%) than in eccentric-only contractions (− 17.5%), when they were performed 5 sets of 30 contractions maximally. However, the present study did not observe such differences between eccentric and concentric contractions, suggesting that motor units were likely to be recruited similarly in the ECC-only and CON-only.
It should be noted that the decreases in EMG in MVC-ISO torque measures were not different between ECC-only or CON-only and CON-ECC conditions, although the decrease in MVC-ISO torque was much greater after CON-ECC (Fig. 5). Linnamo et al. (2000) examined changes in the median frequency of the EMG power spectrum during and immediately after maximal eccentric and concentric exercise consisting of 100 maximal voluntary eccentric and concentrations of the elbow flexors, respectively. They showed that although the average force was higher in eccentric than in concentric contractions, changes in the average rectified EMG (aEMG) values were the same between eccentric and concentric exercises. The results of the present study were in line with the findings by Linnamo et al. (2000).
In CON-ECC, the number of contractions was twice as large as that in the other two conditions. Therefore, it seems likely that acute neuromuscular fatigue was greater in CON-ECC than in the other two conditions, which was shown in the torque changes but not in EMG. Decreases in surface EMG activity over repeated muscle contractions represent a reduction in the central drive to the muscles (Drust et al. 2005) and reflect the recruitment and rate coding of the detected motor units in the region (François 2011). It is likely that repeating maximal muscle contractions reduced the number of motor units recruited over contractions, resulting in a decrease in RMS amplitude found in the present study. Ruas et al. (2022) reported no significant differences in MVC-ISO force, rate of force development, resting twitch force, maximal M-wave, voluntary activation, motor evoked potentials, corticospinal silent period, short interval intracortical inhibition, before, immediately after, and 1–3 days after 48 eccentric-only and 48 coupled concentric–eccentric contractions of the knee extensors, and concluded that eccentric contractions (n = 48 in both conditions) seemed to mainly mediate the neuromuscular responses. It is interesting to include the neuromuscular parameters (resting twitch force, maximal M-wave, voluntary activation, motor evoked potentials, corticospinal silent period, short interval intracortical inhibition) to compare ECC-only, CON-only and CON-ECC contractions of the elbow flexors and other muscle groups. Enoka (1996) concluded that eccentric contractions appeared to require unique activation strategies by the nervous system, including a reduced activation of muscle during maximum eccentric contractions, an altered recruitment order of motor units during submaximal eccentric contractions, a decrease in the size of the potentials evoked in muscle by transcranial and peripheral nerve stimulation, and a greater resistance to fatigue (decline in force) during repeated contractions. Further studies are required to understand possible variations in the neural strategy for eccentric versus concentric contractions.
Limitations of the study
There were several limitations in the present study. Firstly, only young men were used in the study, thus the results of the present cannot be generalized. It is necessary to replicate the study using young women and the elderly. Secondly, the participants of the present study had some resistance exercise experiences for more than six months, but they were not necessarily considered to be highly trained. It is important to investigate whether the results of the present study would be replicated by healthy adults with no or little experience in resistance exercise or more trained individuals. Thirdly, the target muscles in the present study were the elbow flexors. It is necessary to investigate other arm muscles and lower limb and trunk muscles for their fatigue profiles in a similar setting to that of the present study. Fourthly, the present study used isokinetic contractions to standardise the velocity of the movement (30°/s). It is interesting to examine different angular velocities (faster, e.g., 180°/s), and isotonic contractions. It is also important to investigate multi-joint exercises such as bench press and squat, which may be more applicable to practical settings. Fifthly, the order of the three muscle fatigue tasks may have influenced the results, although it was randomised among participants. Muscle damage is induced after an unaccustomed eccentric exercise and recovery takes more than one week (Chen and Hsieh 2001). However, the participants in the present study had been resistance training the elbow flexors for at least 6 months before the study and were familiarised with the exercise protocol one week before the first exercise. Furthermore, there were no significant differences in the baseline MVC-ISO torque among the three conditions. Therefore, it was likely that muscle damage was minimum even after ECC-only contractions. Lastly, the present study assessed biceps brachii EMG but did not include EMG from agonist and antagonist muscles nor other neuromuscular property assessments such as M-wave. In addition, the EMG analysis was limited to RMS. In future studies, mean power frequency and other parameters such as average rectified values should be analysed in EMG. Therefore, further investigations using electrical and transcranial magnetic stimulation are warranted to investigate the mechanisms underpinning less fatigue in eccentric than concentric contractions.
Practical applications
Less fatigue in eccentric than concentric repetitive contractions is important for prescribing resistance training. It is possible to minimise muscle fatigue in resistance training by eliminating concentric contractions with load and focusing on eccentric contractions. Sato et al. (2022a) compared CON-ECC, CON-only, and ECC-only resistance training of the elbow flexors performed twice a week for 5 weeks and showed that ECC-only training produced similar increases in muscle strength (16.2 ± 11.0%) and biceps brachii and brachialis muscle thickness (9.7 ± 7.2%) to those of CON-ECC training, despite the training volume being half of that of CON-ECC. Shibata et al. (2023) showed that 1.6–2.7 times greater repetitions were possible in eccentric-only than concentric-only contractions in arm curl exercise at 70–95% of respective 1-RM load. If this is also the case for other muscles, the less fatiguability in addition to the greater force generation ability in eccentric than concentric contractions is advantageous to provide greater mechanical stimulus to muscles using eccentric-only contractions in resistance training. The greater mechanical stimulus to muscle fibres and extracellular matrix provided by eccentric contractions are important in resistance training (Folland et al. 2002), and muscle fatigue does not appear to be a main factor contributing to muscle strength gain and hypertrophy (Lastayo et al.1999), eccentric-only contractions should be considered more in resistance training. However, to perform ECC-only contractions in resistance training, a specific device is necessary or a spotter is required for the concentric phase. However, it is possible to minimize fatigue by concentric contractions if the concentric phase is performed by both arms and one arm is used for the eccentric phase in an arm curl exercise. A similar arrangement is possible for many of resistance exercises performed on machines (e.g., leg press: extending both legs, bending one leg). Further studies are warranted to investigate whether ECC-only contractions are more effective than CON-only or CON-ECC contractions to maximize muscle adaptations in resistance training.
Conclusion
Greater force generation capacity with less fatiguability in 30 repetitive maximal eccentric than contractions was confirmed in the present study for the elbow flexors. However, when comparing MVC-ISO torque changes from before to immediately after the 30 maximal contractions, no significant difference in the magnitude of decrease was evident between the eccentric and concentric contractions. EMG showed similar decreases in all conditions, and the magnitude of the decrease was not associated with the decrease in MVC torque. These results suggest greater fatigue resistance over repetitive maximal eccentric than concentric contractions, but the fatigue assessed by MVC-ISO does not show the difference. Further research is needed to elucidate the mechanisms underpinning the muscle contraction mode-specific neuromuscular fatigue.
Data availability
All data generated or analysed during this study are included in the article.
Abbreviations
- ANOVA:
-
Analysis of variance
- EMG:
-
Electromyogram
- ES:
-
Effect size
- MVC-CON:
-
Maximum voluntary isometric contraction
- MVC-ECC:
-
Maximum voluntary eccentric contraction
- MVC-ISO:
-
Maximum voluntary concentric contraction
- POST:
-
Immediately after intervention
- PRE:
-
Before intervention
- RMS:
-
Root mean square
- SD:
-
Standard deviation
References
Abbott BC, Bigland B, Ritchie JM (1952) The physiological cost of negative work. J Physiol 117(3):380–390. https://doi.org/10.1113/jphysiol.1952.sp004755
Baudry S, Klass M, Pasquet B, Duchateau J (2007) Age-related fatigability of the ankle dorsiflexor muscles during concentric and eccentric contractions. Eur J Appl Physiol 100(5):515–525. https://doi.org/10.1007/s00421-006-0206-9
Chen TC, Hsieh SS (2001) Effects of a 7-day eccentric training period on muscle damage and inflammation. Med Sci Sports Exerc 33(10):1732–1738. https://doi.org/10.1097/00005768-200110000-00018
Chen TC, Tseng WC, Huang GL, Chen HL, Tseng KW, Nosaka K (2017) Superior effects of eccentric to concentric knee extensor resistance training on physical fitness, insulin sensitivity and lipid profiles of elderly men. Front Physiol 8:209. https://doi.org/10.3389/fphys.2017.00209
Cohen J (2013) Statistical power analysis for the behavioral sciences. Routledge
Čretnik K, Pleša J, Kozinc Ž, Löfler S, Šarabon N (2022) The effect of eccentric vs traditional resistance exercise on muscle strength, body composition, and functional performance in older adults: a systematic review with meta-analysis. Front Sports Act Living 4:873718. https://doi.org/10.3389/fspor.2022.873718
Doss WS, Karpovich PV (1965) A comparison of concentric, eccentric, and isometric strength of elbow flexors. J Appl 20(2):351–353. https://doi.org/10.1152/jappl.1965.20.2.351
Drust B, Rasmussen P, Mohr M, Nielsen B, Nybo L (2005) Elevations in core and muscle temperature impairs repeated sprint performance. Acta Physiol Scand 183(2):181–190. https://doi.org/10.1111/j.1365-201X.2004.01390.x
Enoka RM, Duchateau J (2008) Muscle fatigue: what, why and how it influences muscle function. J Physiol 586(1):11–23. https://doi.org/10.1113/jphysiol.2007.139477
Folland JP, Irish CS, Roberts JC, Tarr JE, Jones DA (2002) Fatigue is not a necessary stimulus for strength gains during resistance training. Br J Sports Med 36(5):370–373. https://doi.org/10.1136/bjsm.36.5.370
François B (2011) Electromyography assessment of muscle recruitment strategies during high-intensity exercise. In: Joseph M (ed) Advances in applied electromyography. IntechOpen, Rijeka, p 2. https://doi.org/10.5772/24358
Fürst DO, Osborn M, Nave R, Weber K (1988) The organization of titin filaments in the half-sarcomere revealed by monoclonal antibodies in immunoelectron microscopy: a map of ten nonrepetitive epitopes starting at the Z line extends close to the M line. J Cell Biol 106(5):1563–1572. https://doi.org/10.1083/jcb.106.5.1563
Guilhem G, Cornu C, Guével A (2010) Neuromuscular and muscle-tendon system adaptations to isotonic and isokinetic eccentric exercise. Ann Phys Rehabil Med 53(5):319–341. https://doi.org/10.1016/j.rehab.2010.04.003
Herzog W (2014) Mechanisms of enhanced force production in lengthening (eccentric) muscle contractions. J Appl Physiol 116(11):1407–1417. https://doi.org/10.1152/japplphysiol.00069.2013
Herzog W (2018) Why are muscles strong, and why do they require little energy in eccentric action? J Sport Health Sci 7(3):255–264. https://doi.org/10.1016/j.jshs.2018.05.005
Hortobágyi T, Katch FI (1990) Eccentric and concentric torque-velocity relationships during arm flexion and extension. Influence of strength level. Eur J Appl Physiol Occup Physiol 60(5):395–401. https://doi.org/10.1007/bf00713506
Kay D, St Clair Gibson A, Mitchell MJ, Lambert MI, Noakes TD (2000) Different neuromuscular recruitment patterns during eccentric, concentric and isometric contractions. J Electromyogr Kinesiol 10(6):425–431. https://doi.org/10.1016/s1050-6411(00)00031-6
Kossev A, Christova P (1998) Discharge pattern of human motor units during dynamic concentric and eccentric contractions. Electroencephalogr Clin Neurophysiol 109(3):245–255. https://doi.org/10.1016/s0924-980x(98)00012-5
Lastayo PC, Reich TE, Urquhart M, Hoppeler H, Lindstedt SL (1999) Chronic eccentric exercise: improvements in muscle strength can occur with little demand for oxygen. Am J Physiol 276(2):R611-615. https://doi.org/10.1152/ajpregu.1999.276.2.R611
Nuzzo JL, Nosaka K (2022) Comment on: Stepwise load reduction rraining: a new trainingconcept for skeletal muscle and energy systems". Sports Med 2022:1–4. https://doi.org/10.1007/s40279-022-01661-8
Pasquet B, Carpentier A, Duchateau J, Hainaut K (2000) Muscle fatigue during concentric and eccentric contractions. Muscle Nerve 23(11):1727–1735. https://doi.org/10.1002/1097-4598(200011)23:11%3c1727::aid-mus9%3e3.0.co;2-y
Peñailillo L, Blazevich A, Numazawa H, Nosaka K (2013) Metabolic and muscle damage profiles of concentric versus repeated eccentric cycling. Med Sci Sports Exerc 45(9):1773–1781. https://doi.org/10.1249/MSS.0b013e31828f8a73
Roig M, O’Brien K, Kirk G, Murray R, McKinnon P, Shadgan B, Reid WD (2009) The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. Br J Sports Med 43(8):556–568. https://doi.org/10.1136/bjsm.2008.051417
Royer N, Nosaka K, Doguet V, Jubeau M (2022) Neuromuscular responses to isometric, concentric and eccentric contractions of the knee extensors at the same torque-time integral. Eur J Appl Physiol 122(1):127–139. https://doi.org/10.1007/s00421-021-04817-y
Ruas CV, Latella C, Taylor JL, Haff GG, Nosaka K (2022) Comparison between eccentric-only and coupled concentric-eccentric contractions for neuromuscular fatigue and muscle damage. Med Sci Sports Exerc 54(10):1635–1646. https://doi.org/10.1249/mss.0000000000002959
Sato S, Yoshida R, Murakoshi F, Sasaki Y, Yahata K, Kasahara K, Nunes JP, Nosaka K, Nakamura M (2022a) Comparison between concentric-only, eccentric-only, and concentric-eccentric resistance training of the elbow flexors for their effects on muscle strength and hypertrophy. Eur J Appl Physiol. https://doi.org/10.1007/s00421-022-05035-w
Sato S, Yoshida R, Murakoshi F, Sasaki Y, Yahata K, Nosaka K, Nakamura M (2022b) Effect of daily 3-s maximum voluntary isometric, concentric or eccentric contraction on elbow flexor strength. Scand J Med Sci Sports. https://doi.org/10.1111/sms.14138
Shibata K, Yamaguchi T, Takizawa K, Nosaka K (2023) Comparison in repetitions to failure between concentric-only and eccentric-only dumbbell arm curl exercise at four different relative intensities. J Strength Cond Res. https://doi.org/10.1519/jsc.0000000000004470
Souron R, Nosaka K, Jubeau M (2018) Changes in central and peripheral neuromuscular fatigue indices after concentric versus eccentric contractions of the knee extensors. Eur J Appl Physiol 118(4):805–816. https://doi.org/10.1007/s00421-018-3816-0
Tesch PA, Dudley GA, Duvoisin MR, Hather BM, Harris RT (1990) Force and EMG signal patterns during repeated bouts of concentric or eccentric muscle actions. Acta Physiol Scand 138(3):263–271. https://doi.org/10.1111/j.1748-1716.1990.tb08846.x
Tseng WC, Nosaka K, Tseng KW, Chou TY, Chen TC (2020) Contralateral effects by unilateral eccentric versus concentric resistance training. Med Sci Sports Exerc 52(2):474–483. https://doi.org/10.1249/mss.0000000000002155
Wu Y, Li RC, Maffulli N, Chan KM, Chan JL (1997) Relationship between isokinetic concentric and eccentric contraction modes in the knee flexor and extensor muscle groups. J Orthop Sports Phys Ther 26(3):143–149. https://doi.org/10.2519/jospt.1997.26.3.143
Yoshida R, Sato S, Kasahara K, Murakami Y, Murakoshi F, Aizawa K, Koizumi R, Nosaka K, Nakamura M (2022) Greater effects by performing a small number of eccentric contractions daily than a larger number of them once a week. Scand J Med Sci Sports. https://doi.org/10.1111/sms.14220
Acknowledgements
The authors gratefully acknowledge all participants involved in this study.
Funding
This work was supported by JSPS KAKENHI #19K19890 (Masatoshi Nakamura).
Author information
Authors and Affiliations
Contributions
RY, KN and MN designed the study. RY, KK, YM and SS collected the data, and RY, KN and MN analysed the data, drafted and revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants
All procedures in the study were in accordance with the ethical standards of the institutional ethics committee. This study was approved by the Ethics Committee of Niigata University of Health and Welfare (#18202).
Informed consent
Informed consent was obtained from each participant involved in the study.
Additional information
Communicated by Michalis G Nikolaidis.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yoshida, R., Kasahara, K., Murakami, Y. et al. Less fatiguability in eccentric than concentric repetitive maximal muscle contractions. Eur J Appl Physiol 123, 1553–1565 (2023). https://doi.org/10.1007/s00421-023-05178-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-023-05178-4