
Abstract
Purpose
Old compared with young adults walk with reduced ankle and increased hip mechanical output. We examined the idea that age, leg strength, or both are related to the age-related changes in mechanical output during gait.
Methods
Healthy young (n = 32, age 21.5 years) and old adults (n = 32, age 76.8 years) participated in biomechanical gait analyses at 1.5 m/s and were also measured for maximal leg strength.
Results
Analysis 1 confirmed previous data as old compared with young adults walked with 50 % more hip positive work and 18 % less ankle positive work. Analysis 2 showed that leg strength did not affect gait kinetics in groups of subjects with similar ages. In a weak young and a strong old group, Analysis 3 showed that old adults still walked with 23 % greater hip positive work. The group by joint interaction in Analysis 4 was suggestive of an even greater reliance on hip and less reliance on ankle work in weak compared with strong old adults.
Conclusions
Age and leg strength both contribute to the age-related changes in mechanical output during gait. Exercise prescription, normally targeting the knee extensors, should also involve ankle and hip muscles.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Healthy aging is associated with visible changes in human locomotion. Old adults’ gait is characterized by slow speed, short steps, and reduced joint range of motion (Abellan van Kan et al. 2009; Beijersbergen et al. 2013; DeVita and Hortobágyi 2000). There are also less perceptible and subtle changes in joint kinetics. Biomechanical gait analyses have consistently shown that healthy old compared with young adults walk with a different configuration of mechanical output generated by the hip, knee, and ankle joints (Beijersbergen et al. 2013; DeVita and Hortobágyi 2000). Old adults’ gait is characterized by a distal-to-proximal shift in mechanical output: hip power increases and ankle power decreases with little or no change in knee joint power. This pattern of redistribution in joint powers, herein referred to as the age-related biomechanical plasticity of gait, is most often independent of gait speed, gender, and aerobic capacity (Beijersbergen et al. 2013; Boyer et al. 2012; Dingwell and Cusumano 2000; Graf et al. 2005; Judge et al. 1996; Kerrigan et al. 1998; McGibbon and Krebs 2004; Monaco et al. 2009; Savelberg et al. 2007; Silder et al. 2008; Winter et al. 1990).
While there are many possible physiological factors that can underlie the phenomenon of biomechanical plasticity, this phenomenon is most likely related to age-related changes in neural and musculoskeletal function. Healthy aging is associated with an up to 50 % reduction in the number and diameter of ventral root myelinated motoneuron axons, a loss of large-diameter axons, slowing of peripheral nerve conduction, impaired sensory fiber function, prolongation of reflex latencies, and up to a 30 % loss and subsequent remodeling of motor units (Aagaard et al. 2011). Such modifications in the trophic effect of neural organization and input to muscle by itself and coupled with age-related sarcopenia lead to a substantial loss in old adults’ ability to produce high levels of voluntary force and power (Danneskiold-Samsoe et al. 2009; Harbo et al. 2012; Hortobágyi et al. 1995; Narici and Maffulli 2011). Based on such well-documented changes in the aging neuromuscular system, it is reasonable to expect that reduction in voluntary leg strength is a mediator of the age-related reorganization of gait mechanics.
However, there is some evidence that if we controlled for physiological, neurological, and biomechanical adaptations that occur with human aging, old age, i.e., being over age 65, per se may also contribute to the biomechanical plasticity of gait. For example, there are conflicting data for the idea that loss of strength does (Anderson and Madigan 2014) or does not (Franz and Kram 2013) mediate reduced ankle mechanical power and work in old adults. The age-typical gait kinetics were present in physically active old runners and sedentary old adults during walking (Savelberg et al. 2007), in sedentary young and old adults during walking, running, and sprinting at maximal speed (Kulmala et al. 2014), and also in the comparison between mobility impaired and healthy old adults (McGibbon and Krebs 2004). It is thus possible that in addition to leg strength, age would also independently contribute to the reorganization of gait. Therefore, we devised a series of novel analyses in which we control for age, leg strength, or both and determine if the age-related gait modifications are present under each of these conditions. Because the age-related gait adaptations are robust and are present even in highly fit and trained old adults (Boyer et al. 2012; Kulmala et al. 2014; Savelberg et al. 2007), the gait adaptations represent a strategy that allows old adults to complete gait tasks despite their levels of muscle strength. Therefore, we favor the hypothesis that age and not leg strength is the defining factor in the age-related biomechanical plasticity of gait. We expect to observe gait differences in comparisons of young and old adults but not in comparisons of weaker and stronger adults. Within the age-based comparisons we expect to observe greater hip and lower ankle joint mechanical output in old compared to young adults.
Methods
Subjects and design
Ultimately 32 young and 32 old adults (28M, 36F) were enrolled in the study. Young subjects were healthy, college students recruited from the campus area. Old adults lived independently in the surrounding communities and all drove automobiles to the laboratory for all sessions. An initial telephone interview determined participants’ functional ability and health history. Subjects were included if they were healthy; defined as being free of musculoskeletal disease or injury, had body mass index (BMI) <30.0 kg/m2, were capable of participating in a maximum strength test, and could perform level walking with no difficulty. Specifically, subjects were considered unhealthy and excluded if they reported any difficulty or pain when performing daily tasks, and had a history of falls, or a history of neurological, musculoskeletal, or cardiovascular disease or injury. A geriatrics physician performed a medical exam on those who passed an initial phone screening thus ensuring all subjects were healthy and capable of participating in all study procedures. Subjects were included who took a medication, for example, to control blood pressure. All subjects completed a physical disability questionnaire to assess functional ability, and performed the testing protocol without difficulty. The University and Medical Center Institutional Review Board approved the study protocol (number 98-044). Subjects read and signed an informed consent before the start of any data collection. Young and old subjects were separated into sub-groups based on a lower extremity strength index score described below, an approach also used recently (Clark et al. 2015). There were 16 subjects in each of the four sub-groups [young weak (4M, 12F), young strong (11M, 5F), old weak (4M, 12F), old strong (9M, 7F)]. Therefore, to determine the effects of age on gait mechanics, we used all of the young (n = 32) and all of the old (n = 32 adults). To determine the effects of leg strength, we combined the weak young (n = 16) and weak old (n = 16) subjects (n = 32 total weak) and the strong young (n = 16) and strong old (n = 16) subjects (n = 32 total strong). Finally, to control for both age and leg strength, we compared the 16 weak young with the 16 strong old adults. Table 1 shows the subject characteristics.
Experimental set-up
An AMTI force platform (Watertown, Massachusetts, USA) located in the center of a 14.3-m level walkway was used to measure ground reaction forces and moments of force at a sampling rate of 960 Hz and gain of 4000. Eight infrared ProReflex cameras (Qualisys Medical AB, Göteborg, Sweden) recorded at 120 Hz 3D gait kinematics of the subjects walking at 1.5 m/s. Data were collected with Qualisys Track Manager Software (Qualisys Medical AB, Göteborg, Sweden) and analyzed with Visual 3D (C-Motion Inc., Rockville, Maryland, USA). Gait speed was measured with an infrared timing system (Brower timing systems, model IRD-T175, Salt Lake City, Utah, USA). A Kin-Com isokinetic dynamometer (Model AP125, Chattecx Corporation, Chattanooga, Tennessee, USA) was used to measure force during isokinetic and isometric leg strength testing.
Testing protocol
Subjects completed the protocol in a single, 2-h-long session. First, subjects completed a disability questionnaire concerning 16 activities of daily living by rating their difficulty doing each activity on a scale from 0 (no difficulty) to 4 (great difficulty) providing a total disability range of 0–64. Next, they performed a functional gait test to determine their habitual walking speed. Subjects walked 20 m on a straight path at a self-selected pace in a well-lit, carpeted, 30-m-long indoor corridor two times. We used gait speed during this test to characterize subjects’ functional ability. For gait analysis, subjects wore black spandex shorts, a tight-fitting T-shirt, and athletic shoes. Standing height and mass were measured. Reflective markers were placed on anatomical locations of the right leg and hip, including the right and left anterior superior iliac spine, between the 5th lumbar and 1st sacral vertebrae, the right and left, iliac crest, the right and left greater trochanter, the medial and lateral space between the femur and tibia of the right knee, and the medial and lateral malleoli of the right ankle. Rigid rectangular plates with 4 markers, each were placed on the lateral thigh and lateral shank. A three-marker triangular plate was also affixed over the midfoot and a single marker on the shoe over the calcaneus. Subjects practised on the walkway to ensure that they would step on the force platform with the right foot without altering the walking pattern or targeting the force platform. Subjects walked at a standard speed of 1.5 m/s (±5 %) for all gait analysis trials. Gait velocity was measured with a Brower infrared timing system (Model IRD-T175, Salt Lake City, Utah). Trials were discarded if the subject walked more than 5 % slower or faster compared with the 1.5 m/s target speed, the foot was not completely on the force platform, or the subject made visually obvious stride alterations to contact the force platform. Five successful trials were collected for each subject. No subjects reported fatigue during or after the test session.
Subjects performed maximal, concentric isokinetic and isometric leg presses after the gait analysis protocol on a Kin-Com dynamometer to comprehensively characterize overall lower extremity strength. Subjects sat on the dynamometer’s seat in the starting position with hip, knee, and ankle joints flexed approximately 90°, 60°, and −10° (dorsiflexed). A lap belt over the waist and a crisscross harness over the trunk stabilized the subject. Subjects performed several warm-up trials by practising the leg press movement at 50–75 % of their maximal ability until they were comfortable with the test before performing the maximal test trials. We selected the leg press because pilot experiments using electromyography showed that a maximal effort in this movement strongly activates the muscles that are also active in the stance phase of gait. The leg press attachment utilized in this protocol was different than a traditional leg press. Only the distal end of the foot made contact with the dynamometer, which forced the participant to utilize their plantarflexors in addition to their hip and knee extensors. These tests measured the combined strength of the hip and knee extensors and ankle plantarflexors. Torque production during concentric contractions of the right leg was measured in a randomized order at 30 and 60°/s. These speeds denote the rotation of lever arm, speeds of old adults were comfortable to execute in preliminary experiments. Subjects were instructed to press on the dynamometer’s footplate while extending the hip, knee, and ankle joints. To represent subjects’ comprehensive leg strength capacity, they also performed maximal isometric contractions at 15°, 45°, and 90° of knee flexion representing relatively extended to flexed lower limb positions. There was 30 s of rest between the maximal trials and 1 min of rest between the isokinetic and isometric conditions. Leg press has been used previously as a composite measure (Bean et al. 2009; Callahan et al. 2007; Claflin et al. 2011), also in the form of jumping and correlated with walking speed (Stenroth et al. 2015).
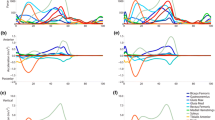
We assessed the reliability of biomechanical and leg strength data in separate experiments in 12 healthy adults (age: 49 ± 6 years). Subjects were tested twice with identical procedures 2 weeks apart. Reliabilities of joint position, torque, and power and isokinetic leg strength were assessed with intraclass correlation coefficients and paired t tests. For the biomechanical tests, comparisons of sample means for 19 variables between test sessions produced non-significant results (p values ranged from 0.180 to 0.903, paired t test). For example, the mean joint torque curves for the two tests were nearly identical at the ankle, knee, and hip joint, respectively. The intraclass correlation coefficients for the isokinetic leg strength measures ranged from 0.87 to 0.97, suggesting a high reliability. The mean knee extension torque values computed for day 1 and day 2 were statistically similar (p > 0.05). Previously, we also reported high reliability (r = 0.74–0.92) for maximal effort knee extension in healthy old adults (Hortobágyi et al. 1995).
Data analysis
We determined the peak torque by digitizing the torque-time curves for the 30 and 60°/s isokinetic and for the isometric leg press trials at 15°, 45°, and 90° knee flexion. Each of the five values was normalized by BMI. The sum of these five normalized values formed the leg press strength index, which was used to divide the old and young groups into strong and weak sub-groups. For the 20-m functional gait test, the speed of the faster of the two trials was used to categorize the subjects’ functional ability. We performed 3D inverse dynamics gait analysis using Visual 3D and custom software to compute, based on linear and angular Newtonian equations of motion, 3D joint torques at the hip, knee, and ankle of the right leg during the stance phase (DeVita and Hortobágyi 2000). Briefly, Cartesian coordinates of the reflective markers were derived from the marker position data when the right leg was in the stance phase of gait and in contact with the force platform. These kinematic data were filtered using a low-pass 2nd order Butterworth bidirectional digital filter at 6 Hz. Ground reaction forces were filtered at 45 Hz. Segmental masses, location of the mass centers, and central moments of inertia were estimated from mathematical models (Dempster 1955). The lower extremity was modeled as four rigid segments (pelvis, thigh, shank, and foot). Joint angular positions and velocities were calculated at the hip, knee, and ankle joints. Joint powers were calculated as the product of the joint torques and joint angular velocities. Positive, negative, and net joint work in all planes in the stance phase were calculated from the hip, knee, and ankle powers as the areas under the joint power-time curves. Positive and negative work indicated that the muscles generated or dissipated mechanical energy (DeVita and Hortobágyi 2000). For the present study, we included only the positive mechanical work in the sagittal plane as a dependent variable because it was 89 % of the total joint work while frontal and transverse plane work were 9 and 2 % of the total and because positive work has been used previously as the basis of mechanical plasticity with age in locomotion (DeVita and Hortobágyi 2000). We also totaled the positive work as the sum across all three joints to estimate the total leg work.
Statistical analyses
We report data as mean ± standard deviation (SD) of each group. t tests were used for age group comparisons on functional ability (i.e., self-selected gait speed) and basic gait variables such as walking speed and stride length, determined from the motion analysis. For each of the four main analyses, we performed a group by joint analysis of variance (ANOVA). The group factor either had two levels of age (young, old) or two levels of leg strength (weak, strong). The joint factor as a repeated measure had three levels: hip, knee, and ankle. Analysis 1 compared joint work between young versus old adults. Analysis 2 compared joint work between weak adults versus strong adults and was controlled for age (i.e., groups had similar age). Analysis 3 compared joint work between young versus old adults and controlled for leg strength (i.e., groups had roughly similar leg strength). Analysis 4 compared joint work in weak old adults versus strong old adults in terms of the relative contribution of hip, knee, and ankle joints to the total positive joint work and was controlled for age (i.e., groups had similar age). In case of a significant interaction effect, we used a priori planned comparisons to determine the means that were different within each joint at p < 0.05. We also examined the influence of leg strength on the shift from distal-to-proximal muscle function in old adults by regressing hip joint work on ankle joint work in old adults (n = 32) and in sub-groups of weak (n = 16) and strong old adults (n = 16).
Results
Table 1 shows that body mass, height, and BMI were similar in the two age groups. Old compared with young adults had 1.8 units higher BMI (p = 0.032), approximately 3 points greater disability on a scale of 64 (p = 0.023), and 43 % lower leg strength (p = 0.001). During the functional gait test, old compared with young adults walked 0.09 m/s or 6.4 % slower at a self-selected speed (p = 0.057). When measured in the laboratory during the gait analysis at a fixed speed of 1.5 m/s, old compared with young adults had 6 cm shorter stride length (p = 0.001) but walked nearly at an identical speed (0.3 % difference, p = 0.382).
Analysis 1
Comparison of joint work between young versus old adults: We compared young and old adults’ gait biomechanics to confirm previously reported age-related adaptations in gait. Table 2 shows the effects of age on the mass-normalized positive work at the hip, knee, and ankle joints during the stance phase of gait. The total positive work was less than 1 % different and not statistically significant (F = 0.009, p = 0.417) in young (0.648 ± 0.102 W/kg) compared with old (0.651 ± 0.117 W/kg) adults. The group (young, old) by joint (hip, knee, and ankle) interaction (F = 8.3, p = 0.001) suggests that old adults walked with 50 % more hip, similar knee, and 18 % less ankle joint positive work. Analysis 1 confirms the previously reported age-related distal-to-proximal shift in gait kinetics (Beijersbergen et al. 2013; DeVita and Hortobágyi 2000).
Analysis 2
Comparison of joint work between weak adults versus strong adults, controlled for age: We controlled for age and determined the effects of leg strength on positive joint work. All of the young (n = 32) and old (n = 32) subjects were ranked based on the leg strength index. The data were then reorganized in which the 16 weakest young subjects and the 16 weakest old subjects were combined into the “weak” sub-group and the 16 strongest young subjects and the 16 strongest old subjects were combined into the “strong” sub-group. Thus, the two sub-groups were separated by leg strength index, independent of age. The weak group had 52 % lower leg strength than the strong group. These weak and strong groups were similar in age [49.6 (±3.4) and 48.7 (±3.4) years], mass [68.8 (±13.2) and 68.9 (±10.2) kg], height [1.69 (±0.09) and 1.71 (±0.09) m], BMI [24.1 (±3.7) and 23.7 (±3.2) kg/m2], stride length [1.54 (±0.07) and 1.51 (±0.07) m], and gait speed [1.57 (±0.04) and 1.52 (±0.03) m/s] (all p > 0.05).
The lower portion of Table 3 shows that leg strength did not affect positive work at the hip, knee, and ankle joints [group (weak, strong) by joint (hip, knee, ankle) interaction, F = 0.9, p = 0.404].
Analysis 3
Comparison of joint work between young versus old adults controlled for leg strength: We examined the effects of age on gait kinetics by controlling for leg strength in a sub-group of weak young (n = 16) and a sub-group of strong old adults (n = 16). The two sub-groups were similar in body mass [70.0 (±15.2) and 70.1 (±10.6) kg], height [1.73 (±0.09) and 1.68 (±0.10) m], and BMI [23.4 (±4.2) and 24.9 (±3.6)] (all p > 0.05). The strong old group was still 13.6 % weaker than the weak young group (p = 0.002) but this difference was much smaller than the 43 % difference in Analysis 1 for all of the young (56.4 ± 13.3 Nm/kg, n = 32) and old adults (31.9 ± 8.6 Nm/kg, n = 32, p = 0.001) and also much smaller than age-based comparisons in the literature whose average is greater than 40 % (Danneskiold-Samsoe et al. 2009; Harbo et al. 2012; Hortobágyi et al. 1995; Metter et al. 1999). Weak young and strong old adults, respectively, walked with similar stride length (1.58 and 1.55 m, p = 0.080) and gait speed (1.51 and 1.52 m/s, p = 0.408) as determined by the biomechanical gait analysis. The results were similar even when we used the weakest 8 of 16 weak young and the strongest eight of strong old adults.
Table 4 shows the positive work at the hip, knee, and ankle joints in the strength-controlled sub-groups of old and young adults. There was no group (weak young, strong old) by joint (hip, knee, ankle) interaction (F = 1.2, p = 0.302). However, an analysis of individual joints revealed that strong old (0.275 J/kg) compared with weak young (0.223 J/kg) subjects walked with 23 % higher positive work generation at the hip joint (p = 0.034). The 6 % lower ankle positive work in this old versus young sub-group was statistically not different.
Analysis 4
Comparison of joint work in weak old adults versus strong old adults: We compared the relative contribution of hip, knee, and ankle joints to the total positive joint work in the stance phase of gait while controlling for age. Sub-groups of weak (n = 16) and strong old adults (n = 16) were formed by ranking old adults (n = 32) on the leg strength index. Table 5 shows that strong compared with weak old adults were 61 % stronger. These two groups of old adults were similar in age (78.1 vs. 75.4 years), mass (67.5 vs. 70.1 kg), height (1.65 vs. 1.68 m), BMI (24.8 vs. 24.9 kg/m2), and gait speed measured during the biomechanical gait analysis (both 1.51 m/s) (all p > 0.05) but weaker old adults walked 0.06 m/s slower (1.49 vs. 1.55 m/s) during the functional gait test (p = 0.023) and with 6 cm shorter stride length measured during the biomechanical gait analysis (1.49 vs. 1.55 m, p = 0.024). Weak compared with strong old subjects walked with 17 % greater contribution to the total positive work generation at the hip and 17 % less at the ankle (both p < 0.05). Despite these large and oppositely directed differences, the group (weak, strong) by joint (hip, knee, ankle) interaction effect was surprisingly not significant (F = 3.0, p = 0.057) although it is possible we have a Type II statistical error.
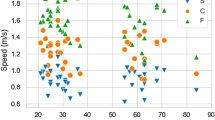
To determine if age, leg strength, or both affect gait biomechanics, we examined the relationship between hip and ankle mechanical joint work in the two sub-groups of old adults. Figure 1 shows a significant inverse relationship. Most old adults with high leg strength appear in the lower hip/higher ankle portion of the distribution and most old adults with low leg strength are in the higher hip/lower ankle area.

Influence of leg strength on the shift from distal-to-proximal muscle function in old adults by showing a significant inverse relationship between hip and ankle mechanical joint work in two sub-groups of old adults. Most old adults with high leg strength appear in the lower hip/higher ankle portion of the distribution (filled symbols, n = 16) and most old adults with low leg strength are in the higher hip/lower ankle area (unfilled symbols, n = 16). The equation y = 2.9x 2 − 2.0x + 0.551 describes the relationship in the entire sample (n = 32) (R 2 = 0.39, p = 0.001 for both linear and quadratic components)
Discussion
Four analyses of positive joint work measured in 64 healthy adults walking at 1.5 m/s confirmed the previously reported age-related distal-to-proximal shift in mechanical output. Additional analyses in sub-groups of subjects in which we controlled for age, leg strength, or both collectively revealed that, against our initial prediction, not only age but most likely it is both age and leg strength that cause the age-related biomechanical plasticity of human gait, i.e., distal-to-proximal shift in mechanical output.
There is now a growing consensus that healthy aging modifies the nature of human gait. A key element in this modification is an increase in hip and a decrease in ankle function. Even if healthy old compared with young adults walk at the same speed, old subjects tend to walk with higher hip but smaller ankle range of motion, torque, power, and work (DeVita and Hortobágyi 2000). This distal-to-proximal adaptation is not the result of altered stride parameters. Since mechanical output at the hips and ankles drive step frequency and step length, respectively (Umberger and Martin 2007), the observed mechanical plasticity is consistent with the observed differences in step length and presumably rate. The older adults walked with shorter steps and higher frequency (since gait speed was controlled) because of increased hip and decreased ankle work. Musculoskeletal modeling also suggests a reciprocal interplay between hip and ankle function during gait so that 30 % simulated reduction in ankle plantarflexor strength slowed gait and increased hip extensor net mechanical work (Goldberg and Neptune 2007). We further address this hip-ankle relationship in Fig. 1. The data for the knee joint are inconsistent because some studies report higher and other studies report lower output at this joint in old compared with young adults (Beijersbergen et al. 2013; McGibbon 2003). In the subsequent sections, we discuss how Analysis 1 confirmed the previously reported distal-to-proximal shift in joint function during gait with age (Table 2) despite the identical total positive work as young adults and provides a valid basis for Analyses 2–4, which in turn suggest that both leg strength and age play a role in the age-related reconfiguration of positive joint work measured during gait.
The age-related gait plasticity is a robust phenomenon. Compared with young males, both physically highly active (runners) and inactive old males exhibited this identical reorganization of joint torques measured during gait (Savelberg et al. 2007). The age-related reduction in ankle power was present even during running and sprinting (Kulmala et al. 2014). On the other end of the continuum, low-performing elderly compared with healthy young and old adults also showed age-related increase in hip and reduction in ankle function (McGibbon and Krebs 2004), independent of walking speed (Graf et al. 2005; Silder et al. 2008). A modeling study suggested that the age-related reorganization of mechanical output during gait is not related to age (Lim et al. 2013). However, the interpretation of the authors’ own data is problematic because the net hip extension moment was significantly greater in old compared with young adults walking with the same step length (young: 73.2 cm; old: 72.20 cm) confirming an age effect. The age-related distal-to-proximal shift in positive joint work during gait is most often interpreted as a compensatory mechanism for the greater and earlier reduction in the function of distal compared with proximal neuromuscular structures (Beijersbergen et al. 2013; Boyer et al. 2012; McGibbon 2003). The age-related distal-to-proximal shift is also resistant to exercise interventions (Beijersbergen et al. 2013). Such interventions do mitigate the effects of neuromuscular dysfunctions by increasing leg strength but still fail to transform old gait to young gait with respect to mechanical joint output. In fact, a recent study showed that increasing leg strength by a leg power intervention actually increases the correlation between hip strength and gait speed and ankle strength and gait speed (Uematsu et al. 2014).
A new finding is that strength independent of age does not mediate biomechanical gait plasticity (i.e., Analysis 2) but strength in conjunction with old age at least partially induces such plasticity (i.e., Analyses 3 and 4). Analysis 2 used a design that created two groups whose leg strength differed by 52 % but controlled for age (weak: 49.6 years; strong: 48.7 years) (Table 3). The results showed that the positive work measured during the stance phase of gait of the weak compared with the strong group differed only −4, 8, and 15 % in hip, knee, and ankle (all non-significant at 0.131 < p < 0.397). Analysis 3 controlled for leg strength by creating a weak young (age 21.1) and a strong old group (age 75.4) differing only about 14 % in leg strength compared with the 43 % difference in the overall young versus old groups (Table 1) and upwards of 40 % in most literature (Danneskiold-Samsoe et al. 2009; Harbo et al. 2012; Hortobágyi et al. 1995; Metter et al. 1999). We emphasize that the strong old group must represent a special segment of healthy old adults who are highly fit, strong, and functionally capable as indicated by the disability questionnaire showing only slightly more difficulty with daily activities in old compared to young subjects. Individual joint analysis showed that despite being similar in leg strength and walking exactly at the same speed, the strongest old adults still walked with 23 % greater hip positive work than the weakest young adults (p = 0.034). The 6 % lower ankle positive work was in the direction predicted by the concept of biomechanical plasticity but was not significant most likely due to low statistical power of 0.32 caused by large inter-subject variability within our sample. This analysis suggests that despite well-maintained lower extremity strength, healthy old adults still exhibit increased proximal hip muscle function. We speculate that this plasticity is driven by factors other than muscle strength, but not restricted to a reduced ability to activate peripheral ankle muscles (Franz and Kram 2012), decrease in foot and ankle flexibility and plantar tactile sensation (Menz et al. 2005), increase in trunk lean that affects hip and ankle muscle mechanics (Miyazaki et al. 2013), and so far not examined age-related changes in cumulative muscle activity per unit distance traveled in soleus compared with hip extensors (Carrier et al. 2011; Farris and Sawicki 2012).
The relative contribution of individual joints to total positive joint work in the stance phase of gait in weak and strong old adults operationalizes the concept of biomechanical plasticity of gait showing that large strength loss in old adults has a strong influence on the redistribution of positive joint work (Analysis 4, Table 5). The strong trend in the group by joint interaction (p = 0.057) and the statistically significant differences in the hip and ankle joint analyses revealed that weak old subjects walked with 17 % greater contribution to the total positive work generation at the hip and 17 % less at the ankle compared with strong old subjects (both p < 0.05). This strength-specific effect on the magnitude of biomechanical plasticity is analogous to Graf et al.’s data showing that while all old adults exhibited this plasticity, “low-performing,” compared to healthy old adults had greater hip and less ankle work in level walking (Graf et al. 2005). Figure 1 demonstrates the influence of leg strength on the shift from distal-to-proximal muscle function in old adults by showing a significant inverse relationship between hip and ankle work in the old subjects, an observation also born out by 30 % simulated reduction in plantarflexion muscle force in musculoskeletal modeling (Goldberg and Neptune 2007). Figure 1 shows that most old adults with high leg strength appear to walk with lower hip positive work but higher ankle positive work compared with most old adults with low leg strength who walk with higher hip positive work but lower ankle positive work. Figure 1 also identifies the upper limit of strength-mediated effect on plasticity in which there still remained 60 % unexplained variance and some weak subjects performed in the strong area and vice versa. In total, these analyses suggest that leg strength influences gait biomechanics only in combination with old age and presumably in conjunction with one or more other factors that age affects. Certainly, more work is needed to identify the precise contributions of each influential variable to mechanical plasticity in addition to the strength contribution. Indeed, data from several previous studies support this idea because the increase in hip and decrease in ankle output was present independent of physical fitness (Boyer et al. 2012; Graf et al. 2005; Kulmala et al. 2014; McGibbon and Krebs 2004; Savelberg et al. 2007). Finally, we conjecture that overall, age independent of strength may play a larger role in hip plasticity and strength may play a larger role in ankle plasticity.
The functional relevance of these cross-sectional findings is not entirely clear. Intervention studies have been successful in substantially increasing measures of neuromuscular function and also gait speed, a summed expression of the underlying biomechanics (Beijersbergen et al. 2013). While biomechanical plasticity seems to imply that exercise interventions should target the especially weakened ankle plantarflexors to slow the loss of mobility, large intervention trials instead target knee extensor function (e.g., (Fielding et al. 2011) or if the ankle is targeted (e.g., (Hartmann et al. 2009), the increase in ankle neuromuscular function does not become incorporated into gait (Beijersbergen et al. 2013). As reported in several previous studies and also shown in Table 5, the knee extensors contribute less than 15 % to the total positive work in the stance phase of gait, yet intervention studies tend to focus on the improvement of quadriceps function to improve walking ability (e.g., Clark et al. 2014). Targeting knee extensor strength is important for activities of daily living old adults who perform at a high relative effort (Hortobágyi et al. 2003). Previous studies have also drawn attention to potential hip joint dysfunctions in many old adults who present with flexion contractures (Kerrigan et al. 1998, 2001). Because even the extremely fit and strong old adults in the present study walked with about 40 % contribution from the hip extensors to the total positive work generated, a contribution that almost reached 50 % in weak old adults, even a small compromise in hip but not knee neuromuscular function would have a magnified unfavorable effect on old adults’ walking ability. In total, evidence from the present and past biomechanical studies suggest a need to re-consider the current practice of exercise prescription for maintaining and improving old adults’ walking ability that only focuses on the knee extensor mechanism rather than all lower extremity joints.
While we propose that the differences in gait are strength-related, they may be influenced by gender in which the strength groups had different numbers of men and women. In the populations of all adults and of separate young and old adults, weaker adults would be predominantly women and stronger would be predominantly men but neither group would be comprised of only one gender; some men are weaker than some women, as illustrated by the data points in Figure 1 of Lindle et al. (1997). While we are not certain of the exact overlap of the frequency distributions of males and females on strength, the gender composition in our samples coincides with the data from Lindle et al. and seems reasonable. Our weak and strong groups had more than 50 % female and more than 50 % male, respectively. Also, we point out that not all females in our samples were weaker than all males in either the young or old groups, again seemingly well matching the populations. We seek to examine the effect of strength among the populations of young and old adults, which we did by separating the participants on only this variable. The gender composition followed naturally from this procedure.
One limitation of the present study is its cross-sectional nature, a threat to external validity. Another limitation is that in Analysis 3 we were unable to fully control for leg strength, weakening but not negating the conclusions. That is, the weak, young adults were stronger than the strong, old adults and thus identifying the old as strong is a slight misnomer. However, the critical issue was that we were able to create two groups of similar ages but dissimilar strength that both contained young and old adults. The strong, old adults were certainly relatively strong for old adults. The same analysis also had somewhat low statistical power and failed to detect an effect in ankle function, an issue future studies could re-examine using an even more optimal design. We also used leg strength instead of leg power as a functional measure and perhaps the conclusion would be even more robust for such an outcome that is becoming recently especially prominent (Dalton et al. 2010, 2014; Power et al. 2014; Reid and Fielding 2012; Yamauchi et al. 2010). Future studies will have to determine: (1) The age at which biomechanical gait adaptations occur, (2) whether or not reductions in strength of individual leg muscle groups are synchronized with changes in gait biomechanics, (3) if increased ankle muscle strength would modify old adults’ gait kinetics to that of young adults (Fig. 1) (Uematsu et al. 2014), and (4) if the leg strength effects on gait depend on gender (Cf. Lindle et al. 1997). The small sample sizes in sub-groups of males and females prevented us from determining if the results are specific to gender. Additionally, walking speed was controlled in this study and the tested speed was similar to young adults’ preferred walking speed. It is possible that some of the observed differences in hip torque are a result of the increased demands of walking at this faster than preferred speed for old adults. The assessment of reliability was sub-optimal and future studies may need to assess reliability for young and old adults separately rather than for one group comprising young and old adults. Finally, we limited the present analysis to positive joint work, a critical variable in gait biomechanics but it could be helpful if future studies examined the effects of age and leg strength on other important kinematic and kinetic variables.
In conclusion, the present study has confirmed the previously reported age-related distal-to-proximal shift in mechanical output during the stance phase of gait in healthy old adults. Additional analyses on sub-groups of subjects who were matched for age, leg strength, or both revealed that mostly likely both age and muscle strength mediate the age-related redistribution of mechanical output during gait. These data could have implications for optimizing exercise prescription for old adults by emphasizing hip and ankle function.
Abbreviations
- ANOVA:
-
Analysis of variance
- BMI:
-
Body mass index
- SD:
-
Standard deviation
References
Aagaard P, Suetta C, Caserotti P, Magnusson SP, Kjaer M (2011) Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports 20:49–64
Abellan van Kan G, Rolland Y, Andrieu S, Bauer J, Beauchet O, Bonnefoy M, Cesari M, Donini LM, Gillette Guyonnet S, Inzitari M, Nourhashemi F, Onder G, Ritz P, Salva A, Visser M, Vellas B (2009) Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging 13:881–889
Anderson DE, Madigan ML (2014) Healthy older adults have insufficient hip range of motion and plantar flexor strength to walk like healthy young adults. J Biomech 47:1104–1109
Bean JF, Kiely DK, LaRose S, O’Neill E, Goldstein R, Frontera WR (2009) Increased velocity exercise specific to task training versus the National Institute on Aging’s strength training program: changes in limb power and mobility. J Gerontol A Biol Sci Med Sci 64:983–991
Beijersbergen CM, Granacher U, Vandervoort AA, DeVita P, Hortobágyi T (2013) The biomechanical mechanism of how strength and power training improves walking speed in old adults remains unknown. Ageing Res Rev 12:618–627
Boyer KA, Andriacchi TP, Beaupre GS (2012) The role of physical activity in changes in walking mechanics with age. Gait Posture 36:149–153
Callahan D, Phillips E, Carabello R, Frontera WR, Fielding RA (2007) Assessment of lower extremity muscle power in functionally-limited elders. Aging Clin Exp Res 19:194–199
Carrier DR, Anders C, Schilling N (2011) The musculoskeletal system of humans is not tuned to maximize the economy of locomotion. Proc Natl Acad Sci 108:18631–18636
Claflin DR, Larkin LM, Cederna PS, Horowitz JF, Alexander NB, Cole NM, Galecki AT, Chen S, Nyquist LV, Carlson BM, Faulkner JA, Ashton-Miller JA (2011) Effects of high- and low-velocity resistance training on the contractile properties of skeletal muscle fibers from young and older humans. J Appl Physiol (1985) 111:1021–1030
Clark DJ, Reid KF, Patten C, Phillips EM, Ring SA, Wu SS, Fielding RA (2014) Does quadriceps neuromuscular activation capability explain walking speed in older men and women? Exp Gerontol 55:49–53
Clark BC, Taylor JL, Hong SL, Law TD, Russ DW (2015) Weaker seniors exhibit motor cortex hypoexcitability and impairments in voluntary activation. J Gerontol A Biol Sci Med Sci 70(9):1112–1119
Dalton BH, Power GA, Vandervoort AA, Rice CL (2010) Power loss is greater in old men than young men during fast plantar flexion contractions. J Appl Physiol 109:1441–1447
Dalton BH, Allen MD, Power GA, Vandervoort AA, Rice CL (2014) The effect of knee joint angle on plantar flexor power in young and old men. Exp Gerontol 52:70–76
Danneskiold-Samsoe B, Bartels EM, Bulow PM, Lund H, Stockmarr A, Holm CC, Watjen I, Appleyard M, Bliddal H (2009) Isokinetic and isometric muscle strength in a healthy population with special reference to age and gender. Acta Physiol (Oxf) 197(Suppl 673):1–68
Dempster WT (1955) Space requirements of the seated operator. Wright-Patterson Air Force Base, Ohio, pp 183–197
DeVita P, Hortobágyi T (2000) Age causes a redistribution of joint torques and powers during gait. J Appl Physiol 88:1804–1811
Dingwell JB, Cusumano JP (2000) Nonlinear time series analysis of normal and pathological human walking. Chaos 10:848–863
Farris DJ, Sawicki GS (2012) The mechanics and energetics of human walking and running: a joint level perspective. J R Soc Interface 9:110–118
Fielding RA, Rejeski WJ, Blair S, Church T, Espeland MA, Gill TM, Guralnik JM, Hsu FC, Katula J, King AC, Kritchevsky SB, McDermott MM, Miller ME, Nayfield S, Newman AB, Williamson JD, Bonds D, Romashkan S, Hadley E, Pahor M (2011) The Lifestyle Interventions and Independence for Elders Study: design and methods. J Gerontol A Biol Sci Med Sci 66:1226–1237
Franz JR, Kram R (2012) The effects of grade and speed on leg muscle activations during walking. Gait Posture 35:143–147
Franz JR, Kram R (2013) How does age affect leg muscle activity/coactivity during uphill and downhill walking? Gait Posture 37:378–384
Goldberg EJ, Neptune RR (2007) Compensatory strategies during normal walking in response to muscle weakness and increased hip joint stiffness. Gait Posture 25:360–367
Graf A, Judge JO, Ounpuu S, Thelen DG (2005) The effect of walking speed on lower-extremity joint powers among elderly adults who exhibit low physical performance. Arch Phys Med Rehabil 86:2177–2183
Harbo T, Brincks J, Andersen H (2012) Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur J Appl Physiol 112:267–275
Hartmann A, Murer K, de Bie RA, de Bruin ED (2009) The effect of a foot gymnastic exercise programme on gait performance in older adults: a randomised controlled trial. Disabil Rehabil 31:2101–2110
Hortobágyi T, Zheng D, Weidner M, Lambert NJ, Westbrook S, Houmard JA (1995) The influence of aging on muscle strength and muscle fiber characteristics with special reference to eccentric strength. J Gerontol A Biol Sci Med Sci 50:B399–B406
Hortobágyi T, Mizelle C, Beam S, DeVita P (2003) Old adults perform activities of daily living near their maximal capabilities. J Gerontol A Biol Sci Med Sci 58:M453–M460
Judge JO, Davis RB 3rd, Ounpuu S (1996) Step length reductions in advanced age: the role of ankle and hip kinetics. J Gerontol A Biol Sci Med Sci 51:M303–M312
Kerrigan DC, Todd MK, Della Croce U, Lipsitz LA, Collins JJ (1998) Biomechanical gait alterations independent of speed in the healthy elderly: evidence for specific limiting impairments. Arch Phys Med Rehabil 79:317–322
Kerrigan DC, Lee LW, Collins JJ, Riley PO, Lipsitz LA (2001) Reduced hip extension during walking: healthy elderly and fallers versus young adults. Arch Phys Med Rehabil 82:26–30
Kulmala JP, Korhonen MT, Kuitunen S, Suominen H, Heinonen A, Mikkola A, Avela J (2014) Which muscles compromise human locomotor performance with age? J R Soc Interface 11:1754–1768
Lim YP, Lin YC, Pandy MG (2013) Muscle function during gait is invariant to age when walking speed is controlled. Gait Posture 38:253–259
Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, Roy TA, Hurley BF (1997) Age and gender comparisons of muscle strength in 654 women and men aged 20–93 yr. J Appl Physiol 83:1581–1587
McGibbon CA (2003) Toward a better understanding of gait changes with age and disablement: neuromuscular adaptation. Exerc Sport Sci Rev 31:102–108
McGibbon CA, Krebs DE (2004) Discriminating age and disability effects in locomotion: neuromuscular adaptations in musculoskeletal pathology. J Appl Physiol 96:149–160
Menz HB, Morris ME, Lord SR (2005) Foot and ankle characteristics associated with impaired balance and functional ability in older people. J Gerontol A Biol Sci Med Sci 60:1546–1552
Metter EJ, Lynch N, Conwit R, Lindle R, Tobin J, Hurley B (1999) Muscle quality and age: cross-sectional and longitudinal comparisons. J Gerontol A Biol Sci Med Sci 54:B207–B218
Miyazaki J, Murata S, Horie J, Uematsu A, Hortobágyi T, Suzuki S (2013) Lumbar lordosis angle (LLA) and leg strength predict walking ability in elderly males. Arch Gerontol Geriatr 56:141–147
Monaco V, Rinaldi LA, Macri G, Micera S (2009) During walking elders increase efforts at proximal joints and keep low kinetics at the ankle. Clin Biomech (Bristol, Avon) 24:493–498
Narici MV, Maffulli N (2011) Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 95:139–159
Power GA, Makrakos DP, Stevens DE, Herzog W, Rice CL, Vandervoort AA (2014) Shortening-induced torque depression in old men: Implications for age-related power loss. Exp Gerontol 57:75–80
Reid KF, Fielding RA (2012) Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Rev 40:4–12
Savelberg HH, Verdijk LB, Willems PJ, Meijer K (2007) The robustness of age-related gait adaptations: can running counterbalance the consequences of ageing? Gait Posture 25:259–266
Silder A, Heiderscheit B, Thelen DG (2008) Active and passive contributions to joint kinetics during walking in older adults. J Biomech 41:1520–1527
Stenroth L, Sillanpaa E, McPhee JS, Narici MV, Gapeyeva H, Paasuke M, Barnouin Y, Hogrel JY, Butler-Browne G, Bijlsma A, Meskers CG, Maier AB, Finni T, Sipila S (2015) Plantarflexor muscle-tendon properties are associated with mobility in healthy older adults. J Gerontol A Biol Sci Med Sci 70(8):996–1002
Uematsu A, Tsuchiya K, Kadono N, Kobayashi H, Kaetsu T, Hortobágyi T, Suzuki S (2014) A behavioral mechanism of how increases in leg strength improve old adults’ gait speed. PLoS One 9:e110350
Umberger BR, Martin PE (2007) Mechanical power and efficiency of level walking with different stride rates. J Exp Biol 210:3255–3265
Winter DA, Patla AE, Frank JS, Walt SE (1990) Biomechanical walking pattern changes in the fit and healthy elderly. Phys Ther 70:340–347
Yamauchi J, Mishima C, Nakayama S, Ishii N (2010) Aging-related differences in maximum force, unloaded velocity and power of human leg multi-joint movement. Gerontology 56:167–174
Acknowledgments
We thank Dr. Alessio Murgia for his insightful comments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Supported in part by National Institutes of Health AG024161.
Additional information
Communicated by Fausto Baldissera.
Rights and permissions
About this article

Cite this article
Hortobágyi, T., Rider, P., Gruber, A.H. et al. Age and muscle strength mediate the age-related biomechanical plasticity of gait. Eur J Appl Physiol 116, 805–814 (2016). https://doi.org/10.1007/s00421-015-3312-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-015-3312-8