
Abstract
Age-related increased hip extensor recruitment during gait is a proposed compensation strategy for reduced ankle power generation and may indicate a distal-to-proximal shift in muscle function with age. Extending beyond joint level analyses, identifying age-related changes at the muscle level could capture more closely the underlying mechanisms responsible for movement. The purpose of this study was to characterize and compare muscle forces and induced accelerations during gait in healthy older adults with those of young adults. Simulations of one gait cycle for ten older (73.9 ± 5.3 years) and six young (21.0 ± 2.1 years) adults walking at their self-selected speed were analyzed. Muscle force and induced acceleration waveforms, along with kinematic, kinetic, and muscle activation waveforms, were compared between age-groups using principal component analysis. Simulations of healthy older adults had greater gluteus maximus force and vertical support contribution, but smaller iliacus force, psoas force, and psoas vertical support contribution. There were no age-group differences in distal muscle force, contribution, or ankle torque magnitudes. Later peak dorsiflexion and peak ankle angular velocity in older adults may have contributed to their greater ankle power absorption during stance. These findings reveal the complex interplay between age-related changes in neuromuscular control, kinematics, and muscle function during gait.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Walking is a generally accessible form of physical activity; however, 25% of Americans over age 55 have difficulty walking one-quarter of one mile.30 It is important for adults to preserve the ability to walk and maintain a physically active lifestyle to reduce the risk of some of the leading causes of death in older adults,5 including heart disease, some cancers, stroke, and type-2 diabetes.26
Older adults tend to walk at slower gait speeds than young adults and with altered joint kinematics and kinetics;16,28 however, these kinematic and kinetic differences persist even when walking speed is similar between age groups.10,32 Older adults tend to spend more time in the double support phase of gait17,37 and walk with increased anterior pelvic tilt.14,16,19 Some studies have also reported shorter step length in older adults;10,14,22,37 however, this finding is not ubiquitous.19,32 Reduced ankle plantarflexion power in older adults is commonly reported,10,14,16,22,28,32,37 but may not be different when correcting for differences in step length.14 Additionally, increased hip extension torque,10 decreased hip flexion torque,10,22 and increased hip power generation10,22,32 in older adults have been reported; however, differences in ankle and hip kinetics are not always observed together.16,37 Altered kinematics and kinetics during walking may be part of a strategy older adults employ to compensate for age-related muscle weakness or impaired muscle activation, or to maximize stability or velocity.34
DeVita and Hortobagyi10 suggested that older adults compensate for decreased use of the ankle plantarflexors (decreased ankle torque) and reduced power generation at the ankle by adopting a gait strategy that increases the use of the proximal hip extensors. The authors suggested this compensation was a neuromuscular adaptation characterized by a distal-to-proximal shift in motor control strategy.10 This hypothesis has been supported by investigations that found differences in joint kinetics22,32 and muscle activity29 between age groups during walking at different speeds. Age-related changes to muscle activation could affect the amount of force a muscle can produce and thus affect joint torque. Furthermore, a muscle’s moment arm, which also determines joint torque, is governed by joint kinematics. Therefore, the previously reported age-related differences in joint kinematics and kinetics may suggest differences in how older adults use their muscles during gait compared to young adults; however, muscle function during gait has not been thoroughly explored in older adults.
Muscle forces facilitate walking by accomplishing two primary functions: providing vertical support and maintaining forward progression of the body’s center-of-mass (COM).15 Several studies have assessed muscle function during walking in young adults2,20,23–25 and found that the vasti, gluteus maximus, and gluteus medius support the body and slow progression (provide braking) during early stance, the dorsiflexors contribute to support and slow the COM during the weight acceptance phase of gait, and finally, the plantarflexors are the primary contributors to support and forward progression during late stance. However, only one study has compared muscle function in healthy older adults during gait with that of young adults.19 The study reported many similarities in muscle contributions to support and progression between young and older adults, although there were age-group differences in the relative contributions to support from the vasti, gluteus medius, and gluteus maximus. However, the findings of this study may not be representative of all older adults because the average walking speed of the older subjects (1.42 m/s) was faster than the walking speeds typically reported for older adults (e.g., 1.0 m/s,14 1.19 m/s,16 1.32 m/s32). Walking speed affects kinematics and kinetics; thus, muscle function of the many older adults who walk at slower gait speeds may not be consistent with the muscle function observed by Lim et al. 19 Further research is necessary to more fully understand how healthy older adults use their muscles to facilitate gait and if this method differs from that of young adults.
Therefore, the objectives of this study were to (1) characterize muscle forces and contributions to COM accelerations (muscle function) during gait in a healthy older adult population walking at a self-selected speed and (2) compare muscle forces and function of healthy older adults with those of a young adult population walking at a self-selected speed. Furthermore, to compare the findings of this study with the current body of literature, as part of a secondary analysis we investigated kinematic and kinetic variables, as well as muscle activation patterns, in older and young adults.
We hypothesized that older adults would use similar muscles to support, brake, and propel their body during gait as have been previously observed in young adults. However, based on the hypothesis of a distal-to-proximal shift in motor control strategy with age, we hypothesized that the older adults would display greater forces and contributions to support and braking from the hip extensors (gluteus maximus and gluteus medius) and smaller forces and contributions from the ankle plantarflexors (soleus and gastrocnemius) compared to the young adults.
Methods and Materials
Subjects
Twenty healthy older adults provided written informed consent in accordance with a protocol approved by the University of Wisconsin-Madison Health Sciences Institutional Review Board as previously described.32 Briefly, each subject performed five over-ground walking trials at their preferred walking speed across a 10 m walkway. Kinematics were tracked using 23 anatomical markers placed on identifiable landmarks and 19 additional markers to aid in tracking and minimize skin motion artifact.6 Additionally, unilateral electromyography (EMG) data were collected from the vastus lateralis, rectus femoris, biceps femoris, soleus, tibialis anterior, medial gastrocnemius, and medial hamstrings. Exclusion criteria for the initial study included current or a history of orthopedic diagnosis, joint pain, or known cardiac, neurologic, gait or balance impairment. The subjects were also screened by a geriatrician and excluded from the study if they obtained a score less than 24 in the Mini Mental State Exam or were unable to perceive a 5.07 Semmes–Weinstein (10 g) monofilament in a plantar sensation test. Prior to gait analysis, each older adult completed a self-reported physical activity questionnaire.33 A subset of ten older adults was chosen for inclusion in this study based on the suitability of each subject’s data for simulation analyses; particularly, the analysis necessitated that the stance leg during the trial was also the leg from which EMG was collected. Furthermore, subjects included in this study were required to have a BMI less than 30 to be considered healthy.
Six healthy young adults who had no history of lower extremity surgery provided written informed consent in accordance with the Institutional Review Board of The Ohio State University. Each subject performed five over-ground walking trials at their preferred speed while kinematic and kinetic data were collected as previously described35 (Table 1). Whole body motion was tracked using the Point-Cluster Technique to aid in tracking and minimize skin motion artifact.3 Additionally, EMG data were collected from the vastus lateralis, rectus femoris, biceps femoris, soleus, tibialis anterior, medial gastrocnemius, gluteus maximus, and gluteus medius.
Gait Simulations
OpenSim 3.28 was used to generate simulations of one representative gait cycle for each subject. A generic musculoskeletal model with 27 degrees-of-freedom and 94 musculotendon actuators4 was used in this study. The hip was modeled as a ball and socket joint with three degrees of freedom (flexion/extension, adduction/abduction, and internal/external rotation). The knee included one degree of freedom (flexion/extension). The ankle joint was defined by one degree of freedom (dorsiflexion/plantarflexion). The metatarsophalangeal and subtalar joints were locked at 0° on each foot as suggested in the OpenSim User’s Guide.11 For each subject, the generic musculoskeletal model was scaled to match the anthropometry of each individual subject by minimizing the difference between the experimental markers’ and the virtual markers’ locations on the musculoskeletal model by achieving a maximum marker error for bony landmarks of less than 4 cm and an RMS marker error of less than 2 cm. Maximum isometric muscle forces are not affected by scaling in OpenSim and were not adjusted for the young nor older adults. Joint angle trajectories that reproduced the experimental marker data with a maximum marker error less than 4 cm and RMS error less than 2 cm were estimated using inverse kinematics.8 An inverse dynamics analysis estimated the net torques at each joint in the model that reproduced the gait kinematics. A residual reduction algorithm8 slightly adjusted model mass properties and joint kinematics to reduce dynamic inconsistency between the ground reaction forces and body segment accelerations. A static optimization (SO) with an objective function that minimized the sum of squared muscle activations7 was used to estimate muscle activations and forces in all lower extremity muscles.
There is currently no “gold-standard” metric for measuring the difference between simulated and experimental muscle activation patterns. Therefore, for this study, the difference between EMG and SO activation patterns was quantified by first normalizing the peak value of the experimental EMG to the peak value of the simulated muscle activation in the SO trial35,36 and calculating an RMS error between the simulated and experimental muscle activity waveforms for each muscle for each subject. Muscle RMS errors were averaged across subjects. Age-group averages of the RMS error for the six muscles for which both age-groups had EMG (biceps femoris, medial gastrocnemius, rectus femoris, soleus, tibialis anterior, and vastus lateralis) were compared using individual 2-sample t tests. There were no statistically significant differences between age-groups for any of the six muscles (p ≥ 0.200). Considering all 6 muscles for both age groups, RMS error ranged from 0.03 to 0.46 with a mean of 0.18 and standard deviation of 0.11. Without similar quantifications of EMG and simulated activation agreement in the literature and given expected differences in magnitude of EMG and SO activations due to the normalization procedure, an average RMS error of 0.18 is believed to represent good consistency between simulated and experimental muscle activations (Fig. A1 in Supplementary Material).
The instantaneous potential for acceleration (IPA) was calculated using a rolling on surface constraint31 to determine the potential of individual muscles to contribute to support and progression of the COM over the gait cycle.35 To determine individual muscle contributions to support, braking, and propulsion, muscle forces estimated by SO were multiplied by the IPA of each muscle for each subject.
Data Analysis
Principal component analysis (PCA)9,12 was applied using custom code in MATLAB 2014a (The MathWorks Inc, Natick, MA, USA) to assess for age-group differences in gait waveforms for individual muscle forces and individual muscle contributions to support and progression. Previous studies have used PCA to identify age-related differences in kinematics and kinetics for stair climbing in young and older adults;27 however, to our knowledge, PCA has not been used to investigate individual muscle forces or contributions to support and progression during gait.
Individual principal component models (PCMs) were created to analyze individual muscle forces, contributions to support, and contributions to progression for each of 11 muscles or muscle groups: gluteus maximus, gluteus medius, vasti (lateralis, medialis, and intermedius), tibialis anterior, soleus, medial hamstrings (semimembranosus and semitendinosus), rectus femoris, biceps femoris (long and short head), gastrocnemius, iliacus, and psoas. Each of the 33 PCMs (3 variables × 11 muscles/muscle groups) included waveforms of both the older and young adults. For all waveforms, the data were time normalized from 0 to 100% of the gait cycle in 201 time points, with each point representing 0.5% of the gait cycle.
For each PCM, an n × p matrix, X, was created such that the n rows corresponded to the 16 subjects (n = 16) and the p columns corresponded to each time point in the gait cycle (p = 201). An eigenvector decomposition of the covariance matrix of X was used to determine the eigenvector matrix, U, containing the loading vectors for the principal components (PCs). Each PC represents an independent feature of the waveform. The PCs were ordered in decreasing order of the amount of variation in the data that they explained, such that the first PC explained the largest amount of variation. The number of PCs, k, included in the final PCM of a variable was determined by the fewest number of PCs needed to explain 90% of the variation in the data. PC Z-scores were calculated as \( Z = \left( {X - \bar{X}} \right)*U \), where \( \bar{X} \) is the mean of X, as a measure of the degree to which each subject’s waveform was correlated with the given PC. A high Z-score indicated the subject’s original waveform was well correlated with that PC.18 To determine the feature described by each PC, the waveforms of the subjects with the minimum and maximum Z-scores for that PC were compared and analyzed alongside the PC’s loading vector.13
For our secondary analyses, PCA was performed to assess for age-group differences in kinematics and kinetics from RRA and SO muscle activations. Individual PCMs were created to assess five sagittal plane kinematic measures (hip flexion, knee flexion, ankle dorsiflexion, lumbar extension, and pelvic tilt). Individual PCMs were created for joint power, torque, and angular velocity for the hip, knee, and ankle and individual muscle activations of the 11 muscle groups previously defined. Joint power was calculated by multiplying joint torque and joint angular velocity. Joint torque and, consequently, joint power were normalized by subject body weight and height. Peak force and moment residuals applied to the pelvis during RRA were also determined for each subject to assess the simulation’s accuracy in tracking the subject’s kinematics and kinetics.
PCA analyzes both the spatial and temporal aspects of waveforms; therefore, to aid in the characterization of when waveform differences occurred with respect to the gait cycle (GC), GC phases were defined. Stance phase was divided into two main phases (early and late stance), each with two sub-phases. Early stance occurred from ipsilateral heel strike (0% GC) to straight leg (30% GC); late stance occurred from straight leg through ipsilateral toe-off (30% to 62–65% GC). The two sub-phases of early stance were weight acceptance, occurring from ipsilateral heel strike to contralateral toe-off, (0–15% GC), and early midstance, occurring from contralateral toe-off to straight leg (15–30% GC). The two sub-phases of late stance were late midstance, occurring from straight leg to contralateral heel strike (30–50% GC), and terminal stance, occurring from contralateral heel strike through ipsilateral toe-off (50% to 62–65% GC). Swing phase was divided into two phases: early and late swing. Early swing occurred from ipsilateral toe-off to midswing (62–65% to 80% GC); late swing occurred from midswing to ipsilateral heel strike (80–100% GC).
Statistical Analysis
Independent two-sample t tests assessed differences in demographics and stride characteristics between the young and older adults. For each of the k PCs of a PCM, independent two-sample t tests assessed age-group differences in Z-scores. A significance level of α < 0.05 was set a priori for all statistical tests. All statistics analyses were performed with Minitab Statistical Software (Minitab, Inc., State College, PA).
Results
Demographics and Stride Characteristics
There were no statistically significant differences in height, mass, BMI, step length normalized by height, or self-selected walking speed between age groups (Table 1). On average, the older adults were 0.03 m (1.7%) shorter, 4.5 kg (6.5%) lighter, and had a 0.6 (2.5%) smaller BMI than the young adults. These differences were within the standard deviations of mass and height for both age-groups. However, the older adults spent a longer percent of the gait cycle in stance (65.3 ± 2.0%) compared to young adults (62.7 ± 1.0%) (p = 0.004). The older adults also spent a longer percent of the gait cycle in double support (28.9 ± 2.7%) compared to the young adults (25.6 ± 1.2%) (p = 0.005).
Characterization of Muscle Force and Function in Healthy Older Adults
In the older adults, the muscles that produced the most force during the gait cycle, as estimated by static optimization, were not necessarily the muscles that contributed most to support and progression (Figs. 1a–1c); this observation was also true for the young adults (Figs. 1d–1f). Although biceps femoris and medial hamstrings produced the largest forces during weight acceptance, tibialis anterior contributed most to support and braking during initial weight acceptance. During the remainder of early stance, the gluteus medius produced the most force, followed by the vasti and gluteus maximus; however, the vasti contributed twice as much to support and over four times as much to braking during early stance compared to the gluteal muscles. In late stance, soleus produced the greatest force and the greatest contributions to support and propulsion. The iliacus and gluteus medius produced similar magnitudes of force as the gastrocnemius during late stance; however, gastrocnemius produced much greater contributions to support and propulsion compared to gluteus medius and iliacus.

Mean muscle force and function curves for older (a–c) and young (d–f) adults. Individual muscle forces (a/d) from static optimization and contributions to progression (b/e) and support (c/f). The y-axes of b/e and c/f represent the magnitude and direction of the muscle’s contribution to the acceleration of the center-of-mass (COM). A positive contribution to progression indicates the muscle’s force propelled the COM forward, and a negative contribution to progression indicates the muscle’s force slowed the COM. A positive contribution to support indicates the muscle’s force supported the COM against gravity, and a negative contribution to support indicates the muscle’s force assisted gravity.
Comparison of Muscle Force and Function Between Older and Young Adults
At least 90% of the variation in each of the 33 PCMs was explained by 2–6 PCs, with an average of 4 PCs. The most common number of PCs needed to explain 90% of the variation was three. Sixteen PCMs were explained by three PCs, eight were explained by four PCs, five were explained by five PCs, three were explained by two PCs (vasti-support, gluteus maximus-support, and gluteus maximus-progression), and one was explained by six PCs (gastrocnemius-progression). There were significant differences in muscle forces and contributions between older and young adults, determined by PCs with Z-scores that were statistically different between age-groups (Tables 2; A4). Each statistically different PC explained between 5% and 86% of the variation in its PCM (Table 2).
Muscle Forces
There were several age-group differences in the magnitude of proximal muscle forces. The gluteus maximus of the older adults produced greater force than the young adults’ gluteus maximus (p = 0.001; Fig. 2b). Furthermore, the gluteus medius of the older adults produced a greater peak force during early stance compared to its peak force during late stance (p = 0.024; Fig. 2g), while the gluteus medius of the young adults produced forces of similar magnitude in early and late stance. In contrast, older adults produced smaller forces in their hip flexors, iliacus (p = 0.015; Fig. 2e) and psoas (p = 0.006; Fig. 2h), compared to young adults. There were no statistically significant differences in PC Z-scores for biceps femoris or rectus femoris (all p ≥ 0.055).


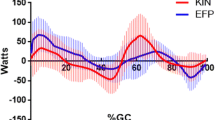
Principal component (PC) analysis results for muscle force PCs that were significantly different between older ( ) and young (
) and young ( ) adults. Loading vectors for the significant PCs (and % variance explained by the PC) are shown in the top plot for each muscle. Below each loading vector, the waveforms with the lowest (Low
) adults. Loading vectors for the significant PCs (and % variance explained by the PC) are shown in the top plot for each muscle. Below each loading vector, the waveforms with the lowest (Low  ) and highest (High
) and highest (High  ) PC Z-scores are shown. These waveforms depict which feature of the curve the PC loading vector captures.
) PC Z-scores are shown. These waveforms depict which feature of the curve the PC loading vector captures.
There were no significant differences in the magnitude of distal muscle forces between the older and young adults; however, there were several differences in the time profiles of those muscles’ forces. Compared to the young adults, the tibialis anterior of the older adults produced a later peak force during weight acceptance and sustained that force throughout early stance (p = 0.042; Fig. 2d). The older adults’ soleus produced its peak force and sustained its force longer into the gait cycle compared to the young adults’ soleus (p = 0.040; Fig. 2f). In contrast to the convex shape of the young adults’ gastrocnemius force profile during late stance, the older adults’ gastrocnemius force profile was concave in shape, with the concavity corresponding to a sharp reduction in force around 50% of the gait cycle when the peak dorsiflexion angle occurs (p = 0.005; Fig. 2c).
Additionally, both the vasti (p = 0.002; Fig. 2a) and the medial hamstrings (p = 0.002; Fig. 2i) of the older adults produced a later peak force during early stance and sustained the forces longer during stance compared to the vasti and medial hamstrings of the young adults.
Muscle Contributions to Progression and Support
To brake and propel their COM forward during gait, healthy older and young adults used similar muscles, but the magnitude and timing of the muscle contributions differed between age-groups (Fig. 3a). Age-group differences in contributions to braking were distributed across distal, intermediate, and proximal muscles (Fig. 3a). The tibialis anterior and vasti primarily contributed to braking in both groups; however, the tibialis anterior of the older adults displayed a greater contribution to braking at heel strike than the young adults’ tibialis anterior (p = 0.043; Fig. 4d). Compared to young adults, the vasti of older adults contributed longer to braking during early stance (p = 0.003; Fig. 4a). Gluteus maximus contributed earlier to braking in older adults than in young adults (p = 0.013; Fig. 4b). Age-group differences in contributions to propulsion were found in distal and proximal muscles. The gastrocnemius and the soleus were the primary muscles that contributed to forward propulsion of the COM in both the older and young adults (Fig. 3a); however, the peak weight acceptance contribution of gastrocnemius to propulsion in older adults occurred at ipsilateral heel strike, while in young adults, the gastrocnemius’ peak weight acceptance contribution occurred slightly after heel strike (p = 0.005; Fig. 4c). There was no difference in peak late stance contributions to propulsion from gastrocnemius between older and young adults. Older adults used some of their proximal muscles more than young adults to propel their COM forward during late stance. Older adults had a greater contribution to propulsion during late stance from iliacus (p = 0.038; Fig. 4e). Additionally, compared to the young adults, the older adults’ biceps femoris had a later onset of contribution to propulsion during late stance that was sustained later in the gait cycle (p = 0.002; Fig. 4f). There were no statistically significant differences between age-groups in contributions to progression from the gluteus medius, medial hamstrings, rectus femoris, soleus, or psoas (all p ≥ 0.053).

Individual muscle contributions to overall center-of-mass (COM) acceleration in the fore-aft (progression, a) and vertical (support, b) directions during stance in older and young adults. Muscle contributions are stacked on top of one another to show their relative contributions to the overall COM acceleration. Healthy older and young adults used similar muscles to support, brake, and propel their COM during gait; however the magnitude and timing of individual muscle contributions differed between age groups.

Principal component (PC) analysis results for individual muscle contribution to progression PCs that were significantly different between older () and young () adults. Loading vectors for the significant PCs (and % variance explained by the PC) are shown in the top plot for each muscle. Below each loading vector, the waveforms with the lowest (Low ) & highest (High ) PC Z-scores are shown. These waveforms depict which feature of the curve the PC loading vector captures.
To vertically support their COM during gait, older and young adults used similar muscles, but the magnitude and timing of the muscle contributions differed between age-groups (Fig. 3b). During early stance, both older adults and young adults primarily used their vasti and tibialis anterior to support their body; however the vasti of the older adults increased its contribution to support at a slower rate compared to the vasti of the young adults (p = 0.001; Fig. 5a). Older adults used their gluteus medius earlier (p = 0.024; Fig. 5f) and more of their gluteus maximus (p = 0.011; Fig. 5c) for support compared to young adults. Older adults received support later in early stance from rectus femoris (p = 0.015; Fig. 5d) compared to young adults. In the older adults, the medial hamstrings contributed more to support at heel strike, while the contribution to support from the medial hamstrings in young adults peaked slightly later during weight acceptance (p = 0.023; Fig. 5e). The onset of the contribution to support from the gastrocnemius occurred later in stance in the older adults than in the young adults (p = 0.014; Fig. 5b). Older adults had a smaller contribution to support during terminal stance from the psoas compared to young adults (p = 0.029; Fig. 5g). Thus, age-group differences in the magnitude of muscle contributions were found only in proximal muscles. However the age-group with the greater contribution from a muscle depended on the function of the muscle. Compared to young adults, older adults had a greater contribution to support from their primary hip extensor (gluteus maximus) and a smaller contribution from one of their hip flexors (psoas). There were no statistically significant differences between age-groups in contributions to support from the biceps femoris, soleus, tibialis anterior, or iliacus (all p ≥ 0.063).

Principal component (PC) analysis results for individual muscle contribution to support PCs that were significantly different between older () and young () adults. Loading vectors for the significant PCs (and % variance explained by the PC) are shown in the top plot for each muscle. Below each loading vector, the waveforms with the lowest (Low ) & highest (High ) PC Z-scores are shown. These waveforms depict which feature of the curve the PC loading vector captures.
Secondary Analyses
Joint Kinematics and Kinetics
There were no statistically significant differences between age-groups in average peak force residuals (Older: 18.2 ± 9.0 N; Young: 11.6 ± 5.6 N; p = 0.096) or average peak moment residuals (Older: 31.7 ± 8.2 Nm; Young: 35.1 ± 9.1 Nm; p = 0.464) after RRA.
Kinematic and kinetic waveforms differed between older and young adults (Table A1; Fig. A2 in Supplementary Material). At least 90% of the variation in all kinematic and kinetic PCMs was explained by 1–6 principal components. Pelvic tilt and lumbar extension angle were each explained by one PC. Hip angle, ankle angle, and ankle power were each explained by three PCs. Knee angle and ankle torque were explained by four PCs. Knee and ankle angular velocity, hip and knee joint torque, and hip joint power were explained by five PCs. Hip angular velocity was explained by six PCs.
Sagittal plane joint angles were not different between age-groups at the hip or knee; however, at the ankle, older adults produced later peak dorsiflexion and plantarflexion angles than the young adults (p = 0.001; Fig. A3-G in Supplementary Material). Pelvic tilt and lumbar extension were not different between older and young adults (Table A2).
Although joint angles were not different, joint angular velocities differed between older and young adults. The older adults’ hip angular velocity amplitude during late stance was smaller than that of the young adults (p = 0.037; Fig. A3-A in Supplementary Material) compared to the young adults. Compared to the young adults, the older adults had a later peak knee angular velocity during terminal stance and late swing (p = 0.044; Fig. A3-D in Supplementary Material). The older adults had later peak ankle angular velocities during late stance and early swing (p = 0.001; Fig. A3-H in Supplementary Material).
Differences in joint torques between older and young adults were found at the hip and knee. Consistent with the hypothesis of a distal-to-proximal shift in neuromuscular control with age, the magnitude of the hip extension torque during early stance was greater in the older adults than in the young adults (p < 0.001; Fig. A3-B in Supplementary Material). Although older adults tended to have a smaller plantarflexion torque than the young adults, there were no statistically significant differences between age groups in the PCs for ankle torque (p ≥ 0.064). At the knee, PC3 captured the older adults’ smaller knee extension torque magnitude during early stance (p < 0.001; Fig. A3-E in Supplementary Material).
Although statistically significant differences in joint torques were not observed at the ankle, joint power differed between age groups at each joint (Table A1). Compared to young adults, older adults had greater positive power at the hip (p < 0.001; Fig. A3-C in Supplementary Material); however, there was no difference between age groups in positive power at the ankle (p = 0.082). Older adults also had later peak power absorption at the knee during late stance and late swing (p = 0.004; Fig A3-F in Supplementary Material). Finally, older adults had greater negative power at the ankle during late stance than the young adults (p = 0.002; Fig. A3-I in Supplementary Material).
Muscle Activations
There were several differences in the magnitude of proximal muscle activations generated from SO between age-groups (Table A3). The gluteus maximus of the older adults had a greater activation than the young adults’ gluteus maximus (p = 0.007; Fig. A4-B in Supplementary Material). Furthermore, the gluteus medius of the older adults had a greater activation during early stance than in late stance (p = 0.001; Fig. A4-H in Supplementary Material), while the gluteus medius of the young adults displayed similar activation magnitudes in early and late stance. The biceps femoris of the older adults displayed greater activation during early stance and terminal stance compared to the biceps femoris of the young adults (p = 0.042; Fig. A4-F in Supplementary Material). During late stance, the hip flexors, iliacus (p = 0.019; Fig. A4-E in Supplementary Material) and psoas (p = 0.005; Fig. A4-I in Supplementary Material), of the older adults were activated less than those of the young adults.
Activation magnitude and timing of three of the distal muscles differed between older and young adults. The tibialis anterior of the older adults displayed a higher activation during early stance (p = 0.024; Fig. A4-D in Supplementary Material). The older adults’ gastrocnemius was activated later and its activation peaked later, compared to the activation of the young adults’ gastrocnemius (p = 0.045; Fig. A4-C in Supplementary Material). The soleus of the older adults also displayed later peak activation (p = 0.025; Fig. A4-G in Supplementary Material). Additionally, the vasti of the older adults displayed later peak activation during early stance and more sustained activation during stance compared to the vasti of the young adults (p < 0.001; Fig. A4-A in Supplementary Material). Finally, compared to the medial hamstrings of the young adults, the older adults’ medial hamstrings displayed smaller activation immediately after heel strike (p = 0.034; Fig. A4-J in Supplementary Material) but greater activation throughout the rest of early stance (p = 0.046; Fig. A4-K in Supplementary Material). There were no statistically significant differences between age-groups in rectus femoris activation waveform features (all p ≥ 0.096).
Discussion
This study aimed to characterize muscle forces and function in healthy older adults and compare healthy older adult muscle function to that of young adults. The study’s approach leveraged dynamic simulations to investigate the hypothesis of an age-related distal-to-proximal shift in neuromuscular control at the muscle level. This hypothesis was previously proposed based on an observed redistribution of joint torque and power,10 which was only partially confirmed in this cohort of healthy older and young adults. We chose PCA because of its capacity to identify differences in spatial as well as temporal characteristics of a data set. Although we found that healthy older and young adults used similar muscles to accelerate their COM during gait, there were many differences between age-groups in the magnitude and timing of muscle forces and contributions to support and progression.
In partial support of our hypothesis and similar to the findings of others,19 the healthy older adults’ gluteus maximus produced a greater force and contribution to support than the young adults’ gluteus maximus in the simulations. However, while the soleus and vasti contributions to support during early stance were, on average, greater in young adults compared to healthy older adults, the differences were not statistically significant. Therefore, the greater role of the gluteus maximus in supporting the COM of the healthy older adults does not appear to be due to a significant decrease in muscle contributions to support of any one muscle or muscles at a single joint.
Contrary to our hypothesis, there were no differences between age-groups in the magnitude of ankle plantarflexor forces and contributions to support and progression. Furthermore, no differences in ankle torque were observed between age groups. It should be noted, however, that the healthy older adults tended to have smaller plantarflexion torques than the young adults. Although the healthy older adults in this study had greater negative ankle power, there was no significant difference in peak positive plantarflexion power between age-groups. These findings are in contrast to previous studies that reported decreased ankle torque and positive power in older adults.10,22,32 There are a few potential reasons for this discrepancy. In the current study, torque and power were normalized to subject weight and height; however, these values were not normalized in DeVita and Hortobagyi.10 Although the subjects in the DeVita and Hortobagyi study were not significantly different in mass or height, the large standard deviations in subject mass and height indicate that individual subject calculations of joint torque and power could have been affected by these parameters. Additionally, in previous studies that reported differences in ankle kinetics, the older adults walked with a significantly smaller stride length than young adults;10,22 however, in the present study, the healthy older and young adults walked with similar step lengths. Shorter stride lengths are associated with decreased ankle torques,1 which may indicate adjustments in stride length are responsible for the previously observed redistribution of lower-limb joint torques rather than an age-related change in neuromuscular control.19 Differences in gait speed may have also contributed to the discrepancy in findings at the ankle. Silder et al. 32 found age-group differences in ankle power at a fast speed (1.58 m/s), but not at a self-selected speed (1.32 m/s), both of which were faster than the average self-selected speed of the healthy older adults included in the current study (1.25 m/s).
Age-related differences in muscle activation patterns, as estimated by simulation, may have contributed to some of the differences in muscle function observed at the hip. The healthy older adults’ gluteus maximus activation was greater than that of the young adults, which likely influenced the greater gluteus maximus force observed in the older adults in this study. Furthermore, the healthy older adults’ iliacus and psoas activations were less than that of the young adults. The decreased activations of the iliacus and psoas during late stance were reflected in the smaller forces observed for these two muscles in the older adults. The increased activation of the primary hip extensor (gluteus maximus) and decreased activation of the hip flexors (iliacus and psoas) in the healthy older adults compared to the young adults may reflect a change in neuromuscular control at the hip. This change in hip muscle activity is consistent with the increased hip extension torque found in the current study and previously reported by DeVita and Hortobagyi.10
Differences in muscle activation magnitude or timing between age-groups did not necessarily correspond to similar differences in muscle force or function. For example, although the healthy older adults’ iliacus had a smaller activation and produced a smaller force during late stance compared to the young adults’ iliacus, the older adults had a larger contribution to propulsion from iliacus during late stance. Kinematic differences could also influence differences in muscle force or function. Kinematics affect muscle moment arms ([R]), a muscle’s location on its force–length-velocity curve (and thus its force (f)), and the orientation and inertial properties of the body segments (the mass matrix: [M]−1), which together determine muscle contributions to acceleration (\( \textit{\"{q}} \))23:
Compared to young adults, older adults may have differences in muscle strength, joint laxity, proprioception, and muscle contraction velocity, any of which could cause a complex chain of reactions resulting in changes to neuromuscular control and altered muscle forces or joint kinematics, which affect muscle induced accelerations (Eq. (2)). A decrease in muscle contribution from a muscle or muscle group at one point in the gait cycle could be made up for by another muscle or muscle group at a different point in the gait cycle. Future work is needed to determine the exact cause or causes of age-related changes in neuromuscular control. For example, forward dynamic simulations could be used to predict emergent behavior or selective weakening could identify compensation strategies for muscle weakness in a particular muscle group.
Although kinematic differences between older and young adults have been observed in previous studies,19,32 the healthy older and young adults in this study walked at similar speeds with joint angles that were not statistically different in magnitude. However, age-group differences in joint angular velocities were observed. The healthy older adults in our study spent a longer percent of the gait cycle in stance compared to young adults, which is consistent with the findings of previous studies.10,19 The later peak plantarflexion angle observed in the older adults is likely due to this longer stance phase. Despite no difference in ankle torque, the healthy older adults had greater power absorption at the ankle compared to young adults, which appeared to be due to differences in joint angular velocity rather than muscle function. However, due to a lack of statistical significance in hip flexion angle magnitude (p = 0.177), we were not able to confirm DeVita and Hortobagyi’s hypothesis that older adults adopt a gait strategy that increases hip flexion to compensate for reduced power generation at the ankle. It is possible that the proposed distal-to-proximal shift that has been suggested based on differences in joint torque and power may not be observed as differences in muscle contributions to support and progression. Differences between older and young adults observed using metrics of joint torques and powers have been hypothesized to be indicative of a change in the locus of muscle function with age; therefore, we suggested this change in muscle function should be evident at the muscle level. We used dynamic simulations to explore these muscle forces, which give rise to joint torques, and their primary function of contributing to the support and progression of the center of mass. However, whether the muscle level or the joint level is better to characterize motor control remains an open question in the field.
The findings of this study may be limited by the small sample size of the two subject groups. The discrepancies in age-related differences in ankle kinematics and kinetics, particularly ankle power generation, between this study and some previous studies of older adult gait may be attributable to the small sample sizes leading to potential type II error in the statistical analyses. However, there are discrepancies in the literature regarding age-related differences in ankle power. Our findings agree with other previous studies that have found no differences in ankle power generation between healthy older and healthy young adults14 and between healthy older and healthy young women,21 particularly when accounting for differences in step length between subjects.14 Additionally, isometric muscle strength was not measured for the subjects; therefore, differences in the muscle strength of the healthy older and young adults are unknown and could not be modeled. However, the healthy older adults in this study were very active, as evidenced by their high scores on a self-reported physical activity questionnaire.32 The same cost function, the sum of muscle activations squared, was used in SO for both older and young adults. However, it is unknown if this cost function commonly used for estimations of muscle activations and forces in young adults is also appropriate for estimating muscle activations and force in older adults. Future work should determine if there is a more appropriate cost function for older adults than the sum of muscle activations squared. Finally, age-related changes in muscle–tendon parameters, which could affect muscle forces and moment arms, were not modeled in this study. The effects of peak isometric muscle force values and strength distribution of the older adult models on the findings of this study were assessed by applying simulated (1) 10% global weakness, (2) 35% global weakness, and (3) 30% plantarflexor weakness in the models of the older adults (Appendix B). A comparison of RMS errors between EMG and activations estimated by SO in the full strength, globally weakened, and plantarflexor weakened cases indicated that agreement between experimental and simulation activations was generally worse with global and local muscle weakening. Furthermore, SO assumes an inelastic tendon. Therefore, altering muscle tendon parameters would not affect muscle forces or activations estimated by SO. Future studies should examine the effects of age-related changes to neuromuscular properties on muscle function during gait.
The findings of this study provide new insights concerning the hypothesis of an age-related distal-to-proximal shift in neuromuscular control, which was initially formulated based on joint level analyses.10 The greater involvement of the gluteus maximus and gluteus medius in braking and supporting the COM during early stance in the older adults in this study suggests these muscles are preferentially recruited in healthy older adults. However, this study did not observe smaller muscle forces or reduced function at the ankle in the healthy older adults. Rather, the changes in kinematics at the ankle may be associated with the greater power absorption observed at the ankle in the older adults. Thus, the results of this study suggest age-related alterations at the muscle level drive differences at the hip, while kinematic modifications dominate adjustments seen at the ankle in healthy older adults. The combined effects of muscular and kinematic adjustments may lead to the observed differences in gait between healthy older and young adults. There is a need to better understand the interplay between neuromuscular control, kinematics, and muscle function during gait in older adults in order to further identify neuromuscular and biomechanical factors essential to the ability to walk and remain physically active.
References
Allet, L., H. IJzerman, K. Meijer, P. Willems, and H. Savelberg. The influence of stride-length on plantar foot-pressures and joint moments. Gait Posture 34:300–306, 2011.
Anderson, F. C., and M. G. Pandy. Individual muscle contributions to support in normal walking. Gait & Posture 17:159–169, 2003.
Andriacchi, T. P., E. J. Alexander, M. K. Toney, C. Dyrby, and J. Sum. A point cluster method for in vivo motion analysis: applied to a study of knee kinematics. J Biomech Eng 120:743–749, 1998.
Arnold, E. M., S. R. Ward, R. L. Lieber, and S. L. Delp. A model of the lower limb for analysis of human movement. Ann Biomed Eng 38:269–279, 2010.
Bureau U.S.C. 65+ in the United States: 2010. 2014, pp. 23–212.
Cappozzo, A., F. Catani, U. D. Croce, and A. Leardini. Position and orientation in space of bones during movement: anatomical frame definition and determination. Clin Biomech 10:171–178, 1995.
Crowninshield, R. D., and R. A. Brand. A physiologically based criterion of muscle force prediction in locomotion. J Biomech (Bristol, Avon) 14:793–801, 1981.
Delp, S. L., F. C. Anderson, A. S. Arnold, P. Loan, A. Habib, C. T. John, E. Guendelman, and D. G. Thelen. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans Biomed Eng 54:1940–1950, 2007.
Deluzio, K. J., U. P. Wyss, B. Zee, P. A. Costigan, and C. Sorbie. Principal component models of knee kinematics and kinetics: normal vs. pathological gait patterns. Hum Mov Sci 16:201–217, 1997.
DeVita, P., and T. Hortobagyi. Age causes a redistribution of joint torques and powers during gait. J Appl Physiol 88:1804–1811, 2000.
Hicks, J. L., OpenSim User’s Guide, 2016, 2012.
Hubley-Kozey, C. L., K. J. Deluzio, S. C. Landry, J. S. McNutt, and W. D. Stanish. Neuromuscular alterations during walking in persons with moderate knee osteoarthritis. J Electromyogr Kinesiol 16:365–378, 2006.
Jones, M. C., and J. A. Rice. Displaying the important features of large collections of similar curves. Am Stat 46:140–145, 1992.
Judge, J. O., R. B. Davis, 3rd, and S. Ounpuu. Step length reductions in advanced age: the role of ankle and hip kinetics. J Gerontol A Biol Sci Med Sci 51:M303–M312, 1996.
Kepple, T. M., K. L. Siegel, and S. J. Stanhope. Relative contributions of the lower extremity joint moments to forward progression and support during gait. Gait Posture 6:1–8, 1997.
Kerrigan, D. C., M. K. Todd, U. Della Croce, L. A. Lipsitz, and J. J. Collins. Biomechanical gait alterations independent of speed in the healthy elderly: evidence for specific limiting impairments. Arch Phys Med Rehabil 79:317–322, 1998.
Lajoie, Y., N. Teasdale, C. Bard, and M. Fleury. Upright standing and gait: are there changes in attentional requirements related to normal aging? Exp Aging Res 22:185–198, 1996.
Landry, S. C., K. A. McKean, C. L. Hubley-Kozey, W. D. Stanish, and K. J. Deluzio. Knee biomechanics of moderate OA patients measured during gait at a self-selected and fast walking speed. J Biomech 40:1754–1761, 2007.
Lim, Y. P., Y. C. Lin, and M. G. Pandy. Muscle function during gait is invariant to age when walking speed is controlled. Gait Posture 38:253–259, 2013.
Liu, M. Q., F. C. Anderson, M. G. Pandy, and S. L. Delp. Muscles that support the body also modulate forward progression during walking. J Biomech 39:2623–2630, 2006.
McGibbon, C. A., and D. E. Krebs. Effects of age and functional limitation on leg joint power and work during stance phase of gait. J Rehabil Res Dev 36:173–182, 1999.
Monaco, V., L. A. Rinaldi, G. Macri, and S. Micera. During walking elders increase efforts at proximal joints and keep low kinetics at the ankle. Clin Biomech (Bristol, Avon) 24:493–498, 2009.
Neptune, R. R., S. A. Kautz, and F. E. Zajac. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J Biomech 34:1387–1398, 2001.
Neptune, R. R., F. E. Zajac, and S. A. Kautz. Muscle force redistributes segmental power for body progression during walking. Gait Posture 19:194–205, 2004.
Pandy, M. G. Computer modeling and simulation of human movement. Annu Rev Biomed Eng 3:245–273, 2001.
Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008.
Reid, S. M., R. B. Graham, and P. A. Costigan. Differentiation of young and older adult stair climbing gait using principal component analysis. Gait Posture 31:197–203, 2010.
Riley, P. O., U. DellaCroce, and D. C. Kerrigan. Effect of age on lower extremity joint moment contributions to gait speed. Gait Posture 14:264–270, 2001.
Schmitz, A., A. Silder, B. Heiderscheit, J. Mahoney, and D. G. Thelen. Differences in lower-extremity muscular activation during walking between healthy older and young adults. J Electromyogr Kinesiol 19:1085–1091, 2009.
Schoenborn, C. A. and K. M. Heyman. Healthy Characteristics of Adults Aged 55 Years and Over: United States, 2004–2007. National Health Statistics Reports No. 16, 2009.
Seth, A., M. Sherman, J. A. Reinbolt, and S. L. Delp. OpenSim: a musculoskeletal modeling and simulation framework for in silico investigations and exchange, 2011 IUTAM symposium on human body dynamics: from multibody systems to. Biomechanics 2:212–232, 2011.
Silder, A., B. Heiderscheit, and D. G. Thelen. Active and passive contributions to joint kinetics during walking in older adults. Journal of Biomechanics 41:1520–1527, 2008.
Stewart, A. L., K. M. Mills, A. C. King, W. L. Haskell, D. Gillis, and P. L. Ritter. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc 33:1126–1141, 2001.
Studenski, S. Mobility. In: Principles of geriatric medicine and gerontology, edited by W. R. Hazzard, J. P. Blass, J. B. Halter, J. G. Ouslander, and M. E. Tinetti. New York: McGraw-Hill, 2003, pp. 947–960.
Thompson, J. A., A. M. Chaudhari, L. C. Schmitt, T. M. Best, and R. A. Siston. Gluteus maximus and soleus compensate for simulated quadriceps atrophy and activation failure during walking. J Biomech 46:2165–2172, 2013.
van der Krogt, M. M., S. L. Delp, and M. H. Schwartz. How robust is human gait to muscle weakness? Gait Posture 36:113–119, 2012.
Winter, D. A., A. E. Patla, J. S. Frank, and S. E. Walt. Biomechanical walking pattern changes in the fit and healthy elderly. Phys Ther 70:340–347, 1990.
Acknowledgments
The authors would like to acknowledge Bryan Heiderscheit for his assistance with data collection. This research was supported by the National Institutes of Health (Grant No. AG24276). This material is also based upon work supported by the National Science Foundation Graduate Research Fellowship Program under Grant Nos. DGE-1343012 (SAS), DGE-0822215 (JAT), and DGE-0718123 (AS).
Conflict of interest
None of the authors have a conflict of interest regarding the contents of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Thurmon E. Lockhart oversaw the review of this article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Schloemer, S.A., Thompson, J.A., Silder, A. et al. Age-Related Differences in Gait Kinematics, Kinetics, and Muscle Function: A Principal Component Analysis. Ann Biomed Eng 45, 695–710 (2017). https://doi.org/10.1007/s10439-016-1713-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-016-1713-4