
Abstract
After spinal cord injury (SCI) skeletal muscle decreases in size, increases in intramuscular fat, and has potential declines in mitochondrial function. Reduced mitochondrial function has been linked to the development of metabolic disease. The aim of this study was to measure mitochondrial function in persons with SCI using near-infrared spectroscopy (NIRS). Oxygen consumption of the vastus lateralis muscle was measured with NIRS during repeated short-duration arterial occlusions in nine able-bodied (AB) and nine persons with motor complete SCI. Skeletal muscle oxidative capacity (V max) was evaluated with two approaches: (1) rate constant of the recovery of oxygen consumption after exercise and (2) extrapolated maximum oxygen consumption from a progressive work test. V max as indicated by the rate constant (k) from the recovery kinetics test was lower in SCI compared with AB participants (k: SCI 0.7 ± 0.3 vs. AB 1.9 ± 0.4 min−1; p < 0.001). Time constants were SCI 91.9 ± 37.8 vs. AB 33.6 ± 8.3 s. V max from the progressive work test approached a significant difference between groups (SCI 5.1 ± 2.9 vs. AB 9.8 ± 5.5 % Hb-Mb/s; p = 0.06). NIRS measurements of V max suggest a deficit of 50–60 % in participants with SCI compared with AB controls, consistent with previous studies using 31P-MRS and muscle biopsies. NIRS measurements can assess mitochondrial capacity in people with SCI and potentially other injured/diseased populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Spinal cord injuries (SCI) were estimated to affect 273,000 persons in the US, including an additional 12,000 new injuries reported each year (Spinal Cord Injury: facts and figures at a glance 2013). With improvements in medical care, all-cause cardiovascular disease has become a major health concern in persons with paraplegia (Soden et al. 2000). Diabetes is also more prevalent in people with SCI (Elder et al. 2004). Altered mitochondrial function has been associated with diabetes mellitus (Befroy et al. 2007; Anderson et al. 2009; Petersen et al. 2004). The links between mitochondrial function and disease (Ballinger 2005) support the need to assess and understand mitochondrial function in persons after SCI.
Several studies have suggested that mitochondrial function is reduced after SCI. These include ~50 % reduction of enzyme levels from muscle biopsies (Castro et al. 2000; Chilibeck et al. 1999; Martin et al. 1992). Limitations to the biopsy approach include the invasive nature of the measurement in a vulnerable population, and also enzymatic measurements may not reflect in vivo mitochondrial function. Recently, magnetic resonance spectroscopy (31P-MRS) has reported ~50 % reduction in the rate of phosphocreatine recovery after exercise in skeletal muscle of persons with SCI (McCully et al. 2011b). Limitations to MRS measurements include the high cost of testing, the limited number of locations that this technology is available, and the need to clear metallic implants for study in high strength magnetic fields. A more affordable and practical non-invasive measurement is needed to assess mitochondrial function after SCI.
Near-infrared spectroscopy (NIRS) is an optical method that relies on the oxygen-dependent changes in near-infrared light absorption and scattering characteristics. NIRS has been used to measure changes in skeletal muscle oxygen levels during exercise (Chance et al. 1992; Wolf et al. 2007; Hamaoka et al. 2007; Ferrari et al. 1997), skeletal muscle blood flow (van Beekvelt et al. 2001b; DeBlasi et al. 1994; Nioka et al. 2006), and skeletal muscle oxygen consumption (van Beekvelt et al. 2001b; Malagoni et al. 2010). A NIRS method has been developed that measures mitochondrial capacity by assessing the rate of recovery of oxygen consumption after exercise using multiple arterial occlusions (Motobe et al. 2004; Buchheit et al. 2011). This technique has recently been used in combination with a blood volume correction algorithm to improve the reliability of oxygen consumption measurements (Ryan et al. 2012). The NIRS approach of measuring mitochondrial capacity has been used on healthy and highly trained populations (Brizendine et al. 2013), but to date has not been applied to the study of skeletal muscle from injured or diseased populations.
The purpose of the present study was to measure mitochondrial capacity in persons with SCI and able-bodied (AB) controls using NIRS. The approach used repeated cuff occlusions after exercise and the blood volume correction algorithm. We used two different approaches to evaluate mitochondrial capacity: the progressive work test and the recovery kinetics test. It was hypothesized that mitochondrial capacity would be reduced in persons with SCI when compared with AB individuals measured with NIRS, similar to previously reported MRS measurements (McCully et al. 2011a).
Methods
Study participants
Participants with motor complete or sensory incomplete SCI as measured by the American spinal injury association impairment scale (AIS) level A or B were recruited for participation in this study. The recovery rate measurements include the results from four participants with SCI used in a previous study (Ryan et al. 2012). AB participants, who were not performing regular moderate to high-intensity exercise, as measured by the International Physical Activity Questionnaire (Hagströmer et al. 2006), were recruited as controls. The study was approved by the Institutional Review Board at the University of Georgia and by the Research Review Committee at the Shepherd Center (Atlanta, GA). We certify that all applicable instructional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. All participants provided written informed consent prior to data collection. Data was collected from October 2011 to August 2012.
To be eligible for the study, participants with SCI had to be able to tolerate sitting upright on an exam table for 60 min without skin compromise or other physical problems. The exclusion criteria were as follows: those with pressure sores on the buttocks and lower extremities, those with orthopedic injuries in the lower extremities, those with a history of severe autonomic dysreflexia, and all females who were pregnant or believed they could be pregnant.
Study design and experimental protocol
This was a cross-sectional study comparing persons with SCI and AB participants. Testing consisted of NIRS measurements of mitochondrial capacity in the vastus lateralis muscle.
Participants were seated upright on a padded table and remained seated upright throughout the duration of the testing session. Legs were positioned straight. The foot of the tested leg was secured in a home-built stabilization holder, which rested on the padded table. The purpose of the foot holder was to minimize motion artifact. SCI participants who did not have abdominal activation placed their hands on the table for additional stability. The NIRS probe (Oxymon MK III, Artinis medical systems, the Netherlands) was placed over the surface of the vastus lateralis muscle and secured on the leg with biadhesive tape and a Velcro strap. The NIRS probe, assembled with two channels, was placed approximately 10 cm proximal to the superior aspect of the patella. Both channels were placed on the same anatomical location, but measured different depths of muscle tissue. NIRS data were sampled at 1,000 Hz and displayed at 10 Hz. A Hokanson vascular cuff (SC 12D or SC 12L depending on leg circumference) was wrapped around the upper thigh, as high as anatomically possible, proximal to the NIRS optode. The cuff was fit to the circumference of the limb. The vascular cuff was attached to a Hokanson AG101 Rapid Cuff Inflation system (Hokanson E20 control box and AG101 compressor). During the experimental setup, the tested leg was lifted up from the table for assembly of the cuff and NIRS probe. After setup was complete, the leg was placed back on the table in a straight position. Participants were encouraged to remain as still as possible to avoid motion artifact during testing.
Adipose tissue overlying the muscle of interest influences NIRS measurements (van Beekvelt et al. 2001a). To control for this, adipose tissue thickness (ATT) was measured for each participant using B-Mode imaging (LOGIQ e; GE Healthcare, USA) at the start of each NIRS protocol. Based on the ATT measurement, the NIRS interoptode distance was adjusted to produce optimal signal-to-noise ratio. For example, channel 1 was set at a distance approximately twice the ATT. This was done to ensure that NIRS light penetration was deep enough to reach active skeletal muscle. The second channel was always set 10 mm longer than channel 1 and this allowed for slightly deeper light penetration into the muscle.
Four homemade aluminum foil electrodes 5 × 5 cm were attached to a Theratouch 4.7 stimulator (Rich-Mar, Inola OK) and positioned over the vastus lateralis muscle as previously described (McCully et al. 2011a). Ultrasound gel was used as a conduction medium between all electrodes and the skin. Pre-wrap was used to keep electrodes in proper position. Electrical stimulation intensity (mA) for AB participants was selected based on the highest tolerable current and ranged from 80 to 160 mA. This was determined individually for each participant and they were encouraged to tolerate high levels of stimulation to ensure muscle activation in the NIRS measurement site. Electrical stimulation intensity for participants with SCI was selected based on producing vigorous muscle contractions of the quadriceps muscles that visually resembled contractions of AB participants at the highest tolerable currents. Electrical stimulation intensities in SCI participants ranged from 100 to 200 mA. NIRS measured recovery rates have been shown to be independent of the amount of muscle activation (Ryan et al. 2013).
NIRS measurements
Skeletal muscle oxygen consumption (mVO2) was measured as the rate of change in muscle oxygenation during brief arterial occlusions from changes in NIRS signals using linear regression. Hemoglobin and myoglobin chromophores both contribute to changes in the NIRS signals (Lutjemeier et al. 2008). This technique assumes that NIRS signal changes are proportional to mitochondrial oxygen consumption due to relative changes in hemoglobin and myoglobin saturation.
Small shifts in blood volume can occur during arterial occlusions due to blood redistribution from high- to low-pressure arterioles. This blood volume shift is detected by NIRS and may mask oxygen consumption measurements, leading to errors in the calculation of mVO2. In this study, the NIRS signals were corrected for this blood volume shift as previously described (Ryan et al. 2012). The correction approach subtracts blood volume shift contributions from the NIRS signal so that changes in the oxygenated hemoglobin signal (O2HB) and changes in the deoxygenated hemoglobin signal (HHB) are symmetrical. The underlying assumption is that arterial occlusion induces a closed system, thus O2HB and HHB are stoichiometrically equivalent. Each arterial occlusion was analyzed and corrected for individually.
Four resting arterial occlusions were performed (10–60 s) and the average of all four occlusions was used. An average of 7–30 s of NIRS data from the occlusions was used, so the linear regression calculation consisted of 70–300 points.
Skeletal muscle oxidative capacity (V max) was determined by two ways: with a progressive work test and a recovery kinetics test. These two approaches have been used previously to measure muscle metabolism with MRS (McCully et al. 1999). The exercise stimulus for the progressive work test and the recovery kinetics test was 15 s of continuous electrical stimulation. The purpose of the exercise stimulus was to activate mitochondrial respiration, and short bouts of electrical stimulation have been used previously to achieve this (Walter et al. 1997; Ryan et al. 2012; McCully et al. 2011a). The advantage of using short-duration stimulation for studying paralyzed skeletal muscle is that previous studies have shown increased fatigability and muscle damage after electrical stimulation (Slade et al. 2004; Bickel et al. 2004b; Mahoney et al. 2007).
The progressive work test was modeled after the transfer function experiments perform using MRS (Chance et al. 1985). This model assumes that ATP breakdown is tightly coupled to ATP synthesis and that the main controlling chemical of mitochondrial oxidative phosphorylation is ADP. Thus, increasing levels of work (i.e. electrical stimulation twitch frequency) correspond directly to increasing levels of ADP. This test began with approximately 1 min of rest followed by five 15-s bouts of electrical stimulation at the following frequencies: 2, 3, 5, 6, and 7 Hz (Pulse duration/interval 200/50 μs) in ascending order. One minute of rest was provided between bouts of electrical stimulation. mVO2 was measured by a 10-s arterial occlusion (250–280 mmHg) performed immediately after cessation of electrical stimulation. mVO2 was calculated by applying linear regression to the linear part of the NIRS slope. The initial linear part of the slope was chosen by eye starting approximately one second into the ischemic test period. For faster metabolic rates, approximately 3 s were chosen so 30 points were used. For slower metabolic rates, approximately 7 s were chosen so 70 points were used. Motion artifact from rapid cuff inflation and deflation was avoided when selecting slopes.
Data from the progressive work test was linearized and extrapolated using the Eadie-Hofstee plot (Lehninger 1976), where mVO2 is equivalent to the velocity, and electrical stimulation frequency was used as a surrogate for substrate concentration (i.e. [ADP]). mVO2 was plotted on the x axis and mVO2/electrical stimulation frequency was plotted on the y axis and slope-intercept equations were determined. According to Eadie-Hofstee plot, V max is equal to the y intercept.
The recovery kinetics test consisted of measuring the recovery rate of mVO2 after exercise (Ryan et al. 2012). Electrical stimulation (15 s at 4 Hz) was used to increase mVO2. Immediately following the electrical stimulation a series of short duration cuffs (5–10 s) were performed as follows: cuffs 1–5 (5 s on/5 s off), cuffs 6–10 (5 s on/10 s off), and cuffs 11– (10 s on/20 s off) over 5 min. To accommodate for the predicted slower recovery rates of people with SCI additional cuff measurements were performed at the end of the cuff protocol described above. mVO2 for each cuff was calculated using linear regression as described above. Post-exercise mVO2 measurements were fit to an exponential curve and rate constants (V max) were calculated, which are proportional to mitochondrial capacity (Forbes et al. 2009; McCully et al. 1993; Richardson et al. 2002).
A physiological calibration was performed and used to normalize NIRS signals for every NIRS test. The calibration provides a range of NIRS optical density unit changes, thus allowing for accurate interpretation of changes in raw NIRS data. The physiological range provides a reference point of 0 % oxygen saturation in the muscle during ischemia and a reference point of 100 % oxygen saturation during reactive hyperemia. Changes in NIRS signal during cuff measurements where normalized within this range and reported as % Hb-Mb/sec. The experimental procedure for the physiological calibration involved electrical stimulation for 10 s followed by a long-duration arterial cuff occlusion (3–5 min) at 250–280 mmHg of pressure.
Statistical analysis
Data are presented as mean ± SD. V max comparisons from progressive work test and recovery kinetics test were made between AB controls and participants with SCI using a Student’s unpaired t test. Significance was accepted when p < 0.05.
Results
Nine participants with SCI and nine AB controls were tested. SCI participants varied in level of injured vertebrae, with a range of C3-T6. Injury duration ranged from 2.7 to 22.1 years. Average age of the SCI group was different than average age of the AB group (43.3 ± 10.7 vs. 30.9 ± 15.8 years, p < 0.05). The SCI group consisted of seven males and two females (78 % male) and the AB group consisted of five males and four females (55 % male). The average BMI was not different between the SCI and AB group (25.1 ± 5.3 vs. 26.5 ± 5.6, p = 0.96). Individual characteristics of participants with SCI are presented in Table 1. There were no adverse events during testing.
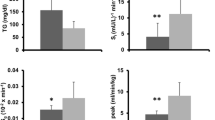
A typical NIRS test including the progressive work test and the recovery kinetics test is shown in Fig. 1. There was no difference in ATT between groups (SCI 0.90 ± 0.30 vs. AB 0.89 ± 0.34 cm; p = 0.96). Resting mVO2 was not different between groups (SCI 0.45 ± 0.29 vs. AB 0.31 ± 0.1 % Hb-Mb/sec; p = 0.14). Experimental results of the progressive work test are presented in Fig. 2. During electrical stimulation, mVO2 increased proportionally with progressive increases in frequency. Average mVO2 for each electrical stimulation frequency level in both AB and SCI groups is presented in panel A of Fig. 2. V max values from the progressive work test were extrapolated from these data using the Eadie Hofstee plot method. The average V max values for the SCI and AB groups approached a significant difference (SCI 5.1 ± 2.9 vs. AB 9.8 ± 5.5 % Hb-Mb/sec; p = 0.06). This is presented in panel B of Fig. 2. The average R 2 values for Eadie Hofstee plot linearization in the SCI group was 0.58 ± 0.26, ranging from 0.03 to 0.83. The average R 2 value for Eadie Hofstee plot linearization in the AB group was 0.69 ± 0.28, ranging from 0.02 to 1.00.

Representative NIRS oxygenated hemoglobin/myoglobin signal from a person with SCI during experimental protocol consisting of a 30-s resting oxygen consumption measurement, progressive work test, recovery kinetics test, and a 5-min physiological calibration

Panel a shows comparisons of the SCI and AB groups during the progressive work test. Average metabolic rates for both groups at each electrical stimulation frequency are presented. Error bars represent SD. Panel b shows Eadie-Hofstee transformation of SCI and AB groups. Solid lines represent average trend lines and dashed lines represent approximate extrapolation of V max values. The values for V max are the average values calculated for each individual participant in each group
A representative NIRS recovery kinetics test can be seen in Fig. 3. Monoexponential recovery curves for an AB participant and a participant with SCI can be seen in Fig. 4. On average, participants with SCI had one-third the V max, as indicated by the rate constant, compared with AB participants (SCI 0.7 ± 0.3 vs. AB 1.9 ± 0.4 min−1; p < 0.001), seen in Fig. 5. The recovery time constants (1/rate constant) were 91.9 ± 37.8 s for the SCI group and 33.6 ± 8.3 s for the AB group. There was no difference in NIRS rate constants between channel 1 (shallow) and channel 2 (deep) in either group (AB p = 0.76 and SCI p = 0.76). The average R 2 values for the exponential curve fit in the SCI group was 0.94 ± 0.06, ranging from 0.83 to 0.99. The average R 2 values for the exponential curve fit in the AB group was 0.98 ± 0.26, ranging from 0.92 to 0.99.

NIRS oxygenated hemoglobin/myoglobin signal during a recovery kinetics test in an able-bodied participant, consisting of 15 s of 4 Hz electrical stimulation followed by a series of short duration arterial occlusion cuffs

Representative NIRS recovery curves of one participant with SCI and one AB participant are presented

Results of NIRS recovery kinetics test comparing recovery rate constants between SCI and AB groups
Discussion
This is the first study to systematically report NIRS-measured mitochondrial capacity in persons with SCI and shows that NIRS is a feasible technique for mitochondrial assessment in a clinical population. NIRS testing can be completed in a time- and cost-efficient matter. This technique is non-invasive and safe for use in some vulnerable populations, as shown here in SCI. This technique can be easily exported to clinical setting and used to monitor mitochondrial responses to various pathologies or therapies.
The reported recovery rate constants extend the preliminary measurements reported in a previous study (Ryan et al. 2012). The relative magnitude of difference in mitochondrial capacity between SCI and AB in this study is similar to the relative difference found with MRS measurements of PCr recovery (Levy et al. 1993; McCully et al. 2011a) and muscle biopsies (Martin et al. 1992). Figure 6 shows the relative differences in mitochondrial function for NIRS, MRS, and muscle biopsy techniques. Furthermore, the NIRS-measured recovery time constants in this study were similar in absolute values to time constants reported for PCr recovery measurements in people with SCI (NIRS time constant = 93 s in this study vs. PCr time constant = 88 s previously reported) (McCully et al. 2011a). AB participants in this study had slightly faster recovery time constants (NIRS time constant = 33 s in this study vs. PCr time constant = 42 s previously reported) (McCully et al. 2011a); however, this difference does not change interpretation of the mitochondrial deficit seen in the SCI group. There was a 12-year difference in age between SCI and AB groups which may have contributed to the reported differences in mitochondrial capacity. However, the degree to which this age differences influence oxidative capacity may not be significant in this study (Larsen et al. 2012).

Normalized mitochondrial capacity for NIRS recovery kinetics test and progressive work test. For comparison, previous studies of mitochondrial capacity used 31P-MRS (McCully et al. 2011a) and succinate dehydrogenase (SDH) activity from muscle biopsies (Martin et al. 1992). AB values were normalized to 1 and SCI values were expressed as a percentage of AB
This study used two approaches to evaluate mitochondrial capacity (V max) with NIRS: the progressive work test (Argov et al. 1987, McCully et al. 1989) and the recovery kinetics test (McCully et al. 1999). These two approaches have been used previously to evaluate muscle metabolism using MRS (McCully et al. 1999). Lower mitochondrial capacity was observed in the SCI group compared with the AB group with both approaches. The progressive work test had inherently greater variability as supported by the R 2 values of the Eadie Hofstee linearization. Variability of this approach is due in part to data extrapolation and the need to accurately quantify work performed. In the present study, we could not verify that the stimulation level completely activated all the muscle tissue sampled by the NIRS device; thus some of the differences (or lack of differences) between the SCI and AB groups could be due to relative differences in the amount of muscle activated. We also used the contraction frequency as a surrogate for work performed (or time–tension integral for isometric contractions) which likely contributed to the variability. Short-duration twitch stimulation was used to reduced the development of muscle damage, which as been reported in previous studies (Slade et al. 2004; Bickel et al. 2004b; Mahoney et al. 2007). Another possible factor influencing variability is that time–tension integral differs between SCI and AB (Bickel et al. 2004a; Scott et al. 2006). Nonetheless, the results of the progressive work test indicate a 52 % difference in mitochondrial capacity between SCI and AB groups. This relative difference is similar to the results of the recovery kinetics test (63 %). The advantage of the recovery kinetics test approach is that it does not require quantification of work, since the rate of recovery will only be influenced by muscle that has been activated (Richardson et al. 2002). Ryan et al. (2013) showed that NIRS measured recovery rates are independent of muscle activation. For this reason, potential sources of variability due to muscle activation differences are reduced in the recovery kinetics test. Another important aspect of this approach is that it requires obtaining signals fast enough to characterize the recovery rate. A key to this approach is making measurements (arterial occlusions) fast enough to capture the recovery of mVO2, which was made possible by the use of an instantaneous arterial cuff inflation device. Overall, the progressive work test is more variable than the recovery kinetics test. This may potentially limit its use in a clinical setting, where individual test results are top priority. In comparison, the recovery kinetics approach is more ideal for a clinical setting due to reduced variability and shorter testing duration.
The variability of NIRS recovery rate constants in SCI was larger than the AB group, which was consistent with previous studies (McCully et al. 2011a; Martin et al. 1992). Characteristics that may have contributed to differences in variability could include injury duration, spasm activity, injury level, and physical activity. Participants with SCI tested in this study varied considerably within each of these categories, consistent with the variability reported in previous studies (McCully et al. 2011a; Martin et al. 1992). Establishing significant and meaningful relationships between the metabolic measurements and potential contributing factors will require larger sample sizes than the one in this study as well as previous studies. One advantage of the NIRS technique is that it is a portable technology that can be applied to studies with large sample sizes that may use multiple testing sites.
NIRS recovery rate constants were not different between shallow and deep channels, consistent with previous studies on AB individuals (Ryan et al. 2012). The deeper channel is thought to obtain signals from deeper tissues and reflect a higher proportion of skeletal muscle rather than subcutaneous non-muscle tissue (van Beekvelt et al. 2001a; Chance et al. 2006). Due to difficulties in quantifying and comparing absolute values of signals between participants that have differing amounts of ATT and muscle, and even potential differences in heme concentrations within the muscle, the use of a physiological calibration to normalize signals is important. The lack of difference between the shallow and deep channels supports the use of a physiological calibration to compare mitochondrial measurements between different groups of participants.
Conclusion
The findings from this study support the use of NIRS measurements as a valuable technique for mitochondrial assessment in a clinical population. NIRS-measured mitochondrial capacity in the SCI group had a ~63 % deficit in mitochondrial capacity compared with the AB group, consistent with previous studies that used 31P-MRS and muscle biopsies. The recovery rate approach to measuring mitochondrial capacity appeared to have less variance and to work better than the progressive work test approach. Future utilization could also involve monitoring changes in mitochondrial health in response to a drug or therapeutic intervention, which may translate to new clinical treatments.
Abbreviations
- AB:
-
Able-bodied
- AIS:
-
American Spinal Injury Association Impairment Scale
- ATP:
-
Adenosine triphosphate
- ATT:
-
Adipose tissue thickness
- MRS:
-
Magnetic Resonance Spectroscopy
- mVO2 :
-
Skeletal muscle oxygen consumption
- NIRS:
-
Near-infrared spectroscopy
- PCr:
-
Phosphocreatine
- SCI:
-
Spinal cord injury
- SDH:
-
Succinate dehydrogenase
- V max :
-
Skeletal muscle oxidative capacity
- 31P-MRS:
-
31-Phosphorous magnetic resonance spectroscopy
References
Anderson EJ, Lustig ME, Boyle KE, Woodlief TL, Kane DA, Lin CT, Price JW, Kang L, Rabinovitch PS, Szeto HH, Houmard JA, Cortright RN, Wasserman DH, Neufer PD (2009) Mitochondrial H2O2 emission and cellular redox state link excess fat intake to insulin resistance in both rodents and humans. J Clin Investig 119(3):573–581. doi:10.1172/jci37048
Argov Z, Bank W, Maris J, Chance B (1987) Bioenergetic heterogeneity of human mitochondrial myopathies: phosphorus magnetic resonance spectroscopy study. Neurology 37:257–262
Ballinger SW (2005) Mitochondrial dysfunction in cardiovascular disease. Free Radic Biol Med 38(10):1278–1295. doi:10.1016/j.freeradbiomed.2005.02.014
Befroy DE, Petersen KF, Dufour S, Mason GF, de Graaf RA, Rothman DL, Shulman GI (2007) Impaired mitochondrial substrate oxidation in muscle of insulin-resistant offspring of type 2 diabetic patients. Diabetes 56(5):1376–1381. doi:10.2337/db06-0783
Bickel CS, Slade JM, Dudley GA (2004a) Long-term spinal cord injury increases susceptibility to isometric contraction-induced muscle injury. Eur J Appl Physiol 91(2–3):308–313. doi:10.1007/S00421-003-0973-5
Bickel CS, Slade JM, Dudley GA (2004b) Long-term spinal cord injury increases susceptibility to isometric contraction-induced muscle injury. Eur J Appl Physiol 91(2–3):308–313. doi:10.1007/s00421-003-0973-5
Brizendine JT, Ryan TE, Larson RD, McCully KK (2013) Skeletal muscle metabolism in endurance athletes with near-infrared spectroscopy. Med Sci Sports Exerc 45(5):869–875
Buchheit M, Ufland P, Haydar B, Laursen PB, Ahmaidi S (2011) Reproducibility and sensitivity of muscle reoxygenation and oxygen uptake recovery kinetics following running exercise in the field. Clin Physiol Funct Imaging 31(5):337–346. doi:10.1111/j.1475-097X.2011.01020.x
Castro MJ, Apple DF Jr, Melton-Rogers S, Dudley GA (2000) Muscle fiber type-specific myofibrillar Ca(2+) ATPase activity after spinal cord injury. Muscle Nerve 23(1):119–121
Chance B, Leigh JS, Clark BJ, Maris J, Kent J, Nioka S, Smith D (1985) Control of oxidative metabolism and oxygen delivery in human skeletal muscle: a steady-state analysis of the work/energy cost transfer function. Proc Nat Acad Sci 82:8384–8388
Chance B, Dait M, Zhang C, Hamaoka T, Hagerman F (1992) Recovery from exercise induced desaturation in the quadriceps muscles of elite competitive rowers. Am J Physiol 262:C766–C775
Chance B, Im J, Nioka Shoko, Kushmerick M (2006) Skeletal muscle energetics with PNMR: personal views and historic perspectives. NMR Biomed 19(7):904–926
Chilibeck PD, Jeon J, Weiss C, Bell G, Burnham R (1999) Histochemical changes in muscle of individuals with spinal cord injury following functional electrical stimulated exercise training. Spinal Cord 37(4):264–268
DeBlasi R, Ferrari M, Natali A, Conti G, Mega A, Gasparetto A (1994) Noninvasive measurement of forearm blood flow and oxygen consumption by near-infrared spectroscopy. J Appl Physiol 76:1388–1393
Elder CP, Apple DF, Bickel CS, Meyer RA, Dudley GA (2004) Intramuscular fat and glucose tolerance after spinal cord injury: a cross-sectional study. Spinal Cord 42(12):711–716. doi:10.1038/sj.sc.31016523101652
Ferrari M, Binzoni T, Quaresima V (1997) Oxidative metabolism in muscle. Phil Trans R Soc Lond B 352:677–683
Forbes SC, Paganini AT, Slade JM, Towse TF, Meyer RA (2009) Phosphocreatine recovery kinetics following low- and high-intensity exercise in human triceps surae and rat posterior hindlimb muscles. Am J Physiol Regul Integr Comp Physiol 296(1):R161–R170. doi:90704.200810.1152/ajpregu.90704.2008
Hagströmer M, Oja P, Sjöström M (2006) The international physical activity questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr 9(6):755–762. doi:10.1079/PHN2005898
Hamaoka T, McCully KK, Quaresima V, Yamamoto K, Chance B (2007) Near-infrared spectroscopy/imaging for monitoring muscle oxygenation and oxidative metabolism in healthy and diseased humans. J Biol Opt 12(6):062105
Larsen RG, Callahan DM, Foulis SA, Kent-Braun JA (2012) Age-related changes in oxidative capacity differ between locomotory muscles and are associated with physical activity behavior. Appl Physiol Nutr Metab 37(1):88–99. doi:10.1139/h11-135
Lehninger A (1976) Biochemistry, 2nd edn. Worth Publishers, Inc., New York
Levy M, Kushnir T, Mizrahi J, Itzchak Y (1993) In vivo 31P NMR studies of paraplegics’ muscles activated by functional electrical stimulation. Magn Reson Med 29(1):53–58
Lutjemeier BJ, Ferreira LF, Poole DC, Townsend D, Barstow TJ (2008) Muscle microvascular hemoglobin concentration and oxygenation within the contraction-relaxation cycle. Respir Physiol Neurobiol 160(2):131–138. doi:S1569-9048(07)00243-110.1016/j.resp.2007.09.005
Mahoney E, Puetz TW, Dudley GA, McCully KK (2007) Low-frequency fatigue in individuals with spinal cord injury. J Spinal Cord Med 30(5):458–466
Malagoni AM, Felisatti M, Mandini S, Mascoli F, Manfredini R, Basaglia N, Zamboni P, Manfredini F (2010) Resting muscle oxygen consumption by near-infrared spectroscopy in peripheral arterial disease: a parameter to be considered in a clinical setting? Angiology 61(6):530–536. doi:10.1177/0003319710362975
Martin TP, Stein RB, Hoeppner PH, Reid DC (1992) Influence of electrical stimulation on the morphological and metabolic properties of paralyzed muscle. J Appl Physiol 72(4):1401–1406
McCully KK, Boden BP, Tuchler M, Fountain MR, Chance B (1989) Wrist flexor muscles of elite rowers measured with magnetic resonance spectroscopy. J Appl Physiol 67(3):926–932
McCully KK, Fielding RA, Evans WJ, Leigh JS Jr, Posner JD (1993) Relationships between in vivo and in vitro measurements of metabolism in young and old human calf muscles. J Appl Physiol 75(2):813–819
McCully K, Mancini D, Levine S (1999) Nuclear magnetic resonance spectroscopy: its role in providing valuable insight into diverse clinical problems. Chest 116(5):1434–1441. doi:10.1378/chest.116.5.1434
McCully KK, Mulcahy TK, Ryan TE, Zhao Q (2011a) Skeletal muscle metabolism in individuals with spinal cord injury. J Appl Physiol 111(1):143–148. doi:10.1152/japplphysiol.00094.2011
McCully KK, Mulcahy TK, Ryan TE, Zhao Q (2011b) Skeletal muscle metabolism in individuals with spinal cord injury. J Appl Physiol 111(1):143–148. doi:10.1152/japplphysiol.00094.2011
Motobe M, Murase N, Osada T, Homma T, Uedo C, Nagasawa T, Kitahara A, Ichimura S, Kurosawa Y, Katsumura T, Hoskika A, Hamaoka T (2004) Noninvasive monitoring of deterioration in skeletal muscle function with forearm cast immobilization and the prevention of deterioration. Dyn Med 3(1):2
Nioka S, Kime R, Sunar U, Im J, Izzetoglu M, Zhang J, Alacam B, Chance B (2006) A novel method to measure regional muscle blood flow continuously using NIRS kinetics information. Dyn Med 5:5. doi:10.1186/1476-5918-5-5
Petersen KF, Dufour S, Befroy D, Garcia R, Shulman GI (2004) Impaired mitochondrial activity in the insulin-resistant offspring of patients with type 2 diabetes. N Engl J Med 350(7):664–671. doi:10.1056/NEJMoa031314
Richardson RS, Noyszewski EA, Haseler LJ, Bluml S, Frank LR (2002) Evolving techniques for the investigation of muscle bioenergetics and oxygenation. Biochem Soc Trans 30(2):232–237
Ryan TE, Brizendine JT, McCully KK (2013) A comparison of exercise type and intensity on the noninvasive assessment of skeletal muscle mitochondrial function using near infrared spectroscopy. J Appl Physiol 114(2):230–237. doi:10.1152/japplphysiol.01043.2012
Ryan TE, Erickson ML, Brizendine JT, Young HJ, McCully KK (2012) Noninvasive evaluation of skeletal muscle mitochondrial capacity with near-infrared spectroscopy: correcting for blood volume changes. J Appl Physiol 113(2):175–183. doi:10.1152/japplphysiol.00319.2012
Scott WB, Lee SC, Johnston TE, Binkley J, Binder-Macleod SA (2006) Contractile properties and the force-frequency relationship of the paralyzed human quadriceps femoris muscle. Phys Ther 86(6):788–799
Slade JM, Bickel CS, Dudley GA (2004) The effect of a repeat bout of exercise on muscle injury in persons with spinal cord injury. Eur J Appl Physiol 92(3):363–366. doi:10.1007/s00421-004-1103-8
Soden RJ, Walsh J, MIddleton JW, Craven ML, Rutkowski SB, Yeo JD (2000) Causes of death after spinal cord injury. Spinal Cord 38:604–610
Spinal Cord Injury: facts and figures at a glance (2013) Spinal cord injury model system. National Spinal Cord Injury Statistical Center, Birmingham, Alabama. https://www.nscisc.uab.edu/PublicDocuments/fact_figures_docs/Facts%202013.pdf. Accessed 16 May 2013
van Beekvelt M, Borghuis M, van Engelen B, Wevers R, Colier W (2001a) Adipose tissue thickness affects in vivo quantitative near-IR spectroscopy in human skeletal muscle. Clin Sci (Lond) 101:21–28
van Beekvelt MCP, Shoemaker JK, Tschakovsky ME, Hopman MTE, Hughson R (2001b) Blood flow and muscle oxygen uptake at the onset and end of moderate and heavy dynamic forearm exercise. Am J Physiol Regul Integr Comp Physiol 280:R1741–R1747
Walter G, Vandenborne K, McCully KK, Leigh JS (1997) Noninvasive measurement of phosphocreatine recovery kinetics in single human muscles. Am J Physiol 272(2 Pt 1):C525–C534
Wolf M, Ferrari M, Quaresima V (2007) Progress of near-infrared spectroscopy and topography for brain and muscle clinical applications. J Biomed Opt 12(6):062104. doi:10.1117/1.2804899
Acknowledgments
The authors would like to thank Jared Brizendine for his assistance in data collection. Funded in part by NIH R01 HD039676.
Conflict of interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Michael Lindinger.
Rights and permissions
About this article
Cite this article
Erickson, M.L., Ryan, T.E., Young, HJ. et al. Near-infrared assessments of skeletal muscle oxidative capacity in persons with spinal cord injury. Eur J Appl Physiol 113, 2275–2283 (2013). https://doi.org/10.1007/s00421-013-2657-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-013-2657-0