
Abstract
To prevent falls in Japan, both gait and resistance training of the lower extremities are recommended. However, resistance training for the elderly induces muscle damage. Recently, aquatic exercise using water buoyancy and resistance have commonly been performed by the elderly. We have now produced new water-resistance equipment. The purpose of the present study was to evaluate the efficacy of aquatic exercise training using the new equipment for the elderly. Subjects were divided into two groups: a resistance group of 12 subjects (using water-resistance equipment) and a non-resistance group of eight subjects (without the equipment). The aquatic exercise training was 90 min, three times per week for 8 weeks, and mostly consisted of walking. All subjects underwent anthropometric measurements, physical performance testing, and profile of mood states (POMS). Significant improvements were observed in muscle strength in plantar flexion, and the timed up and go test (TUG) in both groups. Additionally, 10-m obstacle walking and 5-m maximum walking speed and length with eye-open were significantly improved in the resistance group. Also, a low negative correlation was found between the degree of change in TUG and POMS (tension and anxiety) scores in the resistance group. As it became easier to maintain posture, stand, and move, tension and anxiety in everyday life were alleviated with improvement of strength of the lower extremities and balance function. The present aquatic exercise training using water-resistance equipment may be used by the elderly to improve balance and walking ability, which are associated with the prevention of falls.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recently, the number of elderly people has been progressively increasing. In Japan, current census data reveal that about 27 million people are over 65 years of age, and comprise 21.5% of the entire population (Cabinet Office, White Paper on Aging Society, 2008). Sarcopenia, loss of muscle mass, loss of muscle strength, and physical dysfunction with aging, induces the weakness of the lower extremities and decline of balance function (Greenlund and Nair 2003; Sayer et al. 2006). In particular, falls associated with these changes can make patients bed-ridden and decrease quality of life (QOL) (Landers et al. 2001; Wolfson et al. 1995). To prevent falls, resistance training of the lower extremities are recommended (Hauer et al. 2001). Previous studies have reported that this training can effectively improve maximum isometric strength of the quadriceps and knee extensors and balance function, and decrease the risk of falling by the elderly (Landers et al. 2001). Resistance training using body mass and machines (Liu-Ambrose et al. 2004; Potier et al. 2009) is generally performed; heavy-resistance strength training (Roth et al. 2000) by the elderly can induce muscle damage. Safer exercise training, including proper exercise intensity, is thus needed to prevent muscle damage in the elderly.
Recently, aquatic exercise using the characteristics of water viscosity, buoyancy, and water resistance has commonly been performed by the elderly. In a water environment, the viscosity and buoyancy of water prevent falling by individuals with poor balance. In fact, it has been hypothesized that viscosity and buoyancy may improve balance function (Suomi and Koceja 2000) by stimulation of muscle proprioception (Tokuno et al. 2007; Tokuno et al. 2008) and deep muscles (Kaneda et al. 2007) in water.
Since weight-bearing force on the skeletal joints during exercise is reduced by buoyancy (Konlian 1999), walking in water is often easier and safer for the elderly. Furthermore, aquatic exercise against water resistance improved muscle strength in the lower extremities (Gusi et al. 2006; Kaneda et al. 2007; Wang et al. 2007). Recently, it was reported that aquatic exercise using the Flowmill (FM1200D, Japan Aqua Tech Co., Ltd., Japan), a treadmill controlled by water flumes, significantly increased maximal oxygen uptake, walking speed, and muscle activity of the lower extremities in middle-aged women (Shono et al. 2001, 2007).
We have now produced new water-resistance equipment in association with DESCENTE, LTD. This equipment with two sacks can adjust water resistance in proportion to walking speed. It is already known that density of water is 700 times that of air (Moening et al. 1993), and water resistance is proportional to the square of speed. Water resistance should thus be enhanced associated with increase in walking speed. Furthermore, many previous studies have reported that exercise intensity can be modulated by adjusting the velocity of movement in water (Ferrell 1998; Konlian 1999). Though we did not measure the resistance using this equipment, subjects perceived that the equipment increased exertion levels. For these reasons, water resistance increases when walking speed rises, but decreases when walking speed becomes slow. We believe using this equipment would not only increase muscle activity of the lower extremities, such as the femoral region and the crus, but also prevent fall associated with balance function in the elderly.
The purposes of the present study were to evaluate the effects of aquatic exercise training using the new water-resistance equipment on exercise performance and profile of mood states (POMS) of the elderly.
Methods
Subjects
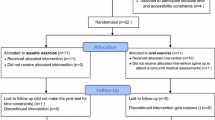
Thirty-one (9 males and 22 females) healthy elderly individuals who did not exercise regularly were recruited in this protocol. They were all over 65 years of age. Eleven subjects were excluded due to trouble in home (n = 4), falls out of the training time (n = 2), absence of the measurement (n = 2), high exercise frequency (such as three times/week) (n = 2), and infectious disease (n = 1). Finally 20 subjects (4 males and 16 females; age 69.1 ± 4.5 years, body mass 55.9 ± 9.1 kg, %fat 30.6 ± 6.1 BMI 24.1 ± 2.7 kg/m2) were recruited in this study. We randomly assigned them to two groups a resistance group of 12 subjects (1 male and 11 females; age 68.5 ± 4.2 years, body mass 54.2 ± 7.1 kg, %fat 32.3 ± 5.1, BMI 23.8 ± 2.3 kg/m2) who exercised in water with using the equipment, and a non-resistance group of eight subjects (3 males and 5 females; age 70.0 ± 5.1 years, body mass 58.6 ± 11.7 kg, %fat 28.2 ± 7.1, BMI 28.2 ± 7.1 kg/m2) who exercised in water without the equipment (Table 1). All subjects provided written informed consent for participation in the study, which was approved by the Ethics Committee of Osaka City University (Admitting No 1193).
Water-resistance equipment
The newly made water-resistance equipment (Power leg, DESCENTE Co., Ltd., Japan) with two sacks to receive water were worn one on each crus (Fig. 1). When walking forward in water using the equipment, the sacks catch water so that water resistance is increased. One of the characteristics of this equipment is that it enhances the water resistance in proportion to walking speed. So the faster one walks in water the larger the water resistance becomes.

The new water-resistance equipment with two adjunct sacks used in the resistance group. The equipment (c) enhances the water resistance in gait (a) and front kick (b)
Aquatic exercise training
The aquatic exercise training for both resistance and non-resistance groups was 90 min, three times per week for 8 weeks at the small pool of a day-care-facility in Osaka city. The water temperature was 30–32°C. Aquatic exercise was led by two trained fitness instructors and supervised by researchers. The training protocol consisted of 90 min with 15-min warm-up and flexibility exercises, 60-min endurance and strength exercises based on walking, and a 15-min cool-down. In the first week, warming-up, stretching, and walking to forward, side, and back were performed to music. In addition, rubber-tube devices were used for exercise of both leg abduction and adduction muscles. In the second week, complicated exercises, including recreation, dancing to music, abdominal twists, and elbows to knees, were performed in addition to the first-week protocol. In the third week, resistance exercise with abdominal muscles as twisting knee up, hold knee and kicking to front were performed in addition to the second-week protocol. During the fourth to eighth weeks, based on the third-week protocol, walking with long strides, abdominal twists, kicking to the front, rubber-tube exercise and recreation were performed. The intensity of the aquatic exercise was adapted to “moderately strong” RPE level. Symptoms, body temperature, and blood pressure at rest were measured before exercise each day.
Measurements
All subjects underwent anthropometric measurements (height, body mass, BMI, and percent body fat); blood pressure and physical performance tests before and after training period were performed by the same examiner. Blood pressure was measured in the sitting position after resting for 10 min. If blood pressure was equal to or higher than 180/100 mm/Hg, we measured it once again after resting for 2 or 3 min. When blood pressure did not decrease below 180/100 mm/Hg over three times measurements, these fitness tests were not performed. Percent body fat was analyzed using a bioelectrical impedance analyzer (BIA) (In body 3.0, Biospace Japan Inc., Japan). Physical performance testing consisted of sit and reach, knee extension force, 10-m obstacle walking time, 5-m maximum speed walking time, timed up and go test (TUG), and center of gravity movement. In addition to these, we measured strength of the triceps surae and tibialis anterior muscles, which control plantar flexion and dorsiflexion of the ankle joint during walking.
Knee extension force was measured using a hand-held dynamometer (GT-10, OG Giken, Okayama, Japan) in sitting position with the knee/hip and ankle flexed at about 90°. The dynamometer was pressed to the anterior or dorsal surface of the distal tibia. To keep the subject stable, the measured thigh was held strongly fixed by an assistant. Extension forces in both legs were measured three times, and the maximum value was recorded in torque. The sit-and-reach test was performed (Digital sit and reach meter T.K.K 5112, Takei Instruments., Japan). The test was chosen for lower-body flexibility (ACSM 1999) and was performed first, with a slight modification in the starting position, such that the subject began the test with the back flat against the wall and reached forward from that position. The 10-m obstacle walking time was measured as the fastest time in seconds to walk over six obstacles (20 cm height) placed at distances of 2 m from each other in seconds. A 5-m maximum walking speed test was used to measure the walking speed of subjects to detect their functional capacity in daily life; the subjects were asked to walk in a straight path as fast as they could. The time spent to complete the task was recorded in seconds. A test of TUG, evaluating balance function, was performed to measure the time required for the subject to stand up from a chair, walk a distance of 3 m, walk back to the chair, and sit down. This simple test provides a comprehensive evaluation of the subject’s balance, gait, speed, and functional ability in seconds. We supported the subject to prevent falling on standing up from the chair. On every measurement, two assessments were performed and recorded the best value. Center of gravity movement was calculated using a stabilometer (Gravicorder GS-11, ANIMA Co., Ltd., Japan) with stability index and postural sway during a static stance with both feet under eye-open and eye-closed conditions. In cases where eye-open condition, subjects watched a marker 2 m in front. Center of balance was defined as the point on the foot at which the body mass was equally distributed between the medial–lateral and anterior–posterior quadrants, and was recorded in centimeters. Stability index was defined as the mean deviation in sway around the center of balance. Postural sway was expressed as the maximum sway distance recorded (cm) in the medial–lateral and anterior–posterior directions. Furthermore, muscle strengths of the triceps surae and tibialis anterior were measured using both a tensile force attachment (Takei Instruments., Japan) and digital dynamometer (T.K.K 1269, Takei Instruments., Japan). Strength of the triceps surae muscle was measured as maximal force of plantar flexion in kilograms. Subjects were in spine position with a knee angle of near 180° (full extension) with the ankle joint at 90°. Strength of the tibialis anterior muscle was measured as maximal force of dorsiflexion in kilograms in the same position. Plantar flexion and dorsiflexion forces in both legs were measured twice of each side, and the total maximal value of each side was recorded.
Furthermore, we evaluated subjective symptoms using the POMS. The POMS questionnaire contained 65 items on mood state. Scores (on a 5-point scale of 0–4) are grouped into six subscales: tension–anxiety (T–A), depression–dejection (D), anger–hostility (A–H), vigor (V), fatigue (F), and confusion (C). Subscale scores were converted to T-scores for statistical analysis, and overall mood disturbance was also calculated.
Statistical analyses
All statistical analyses were performed using SPSS for Windows (SPSS Inc., Chicago, IL, USA). All data were normally distributed, and presented as mean ± SD. The paired Student’s t test was used to compare each variable within-group before versus after training. The significances of difference in physical characteristics and POMS score between groups were determined by two-way ANOVA. The post-hoc Tukey’s test was preformed when warranted. Correlations between variation of physical performance of TUG and POMS (T–A) score were examined by determination of Pearson’s correlation coefficients. Differences at P < 0.05 were considered significant for all statistical analyses.
Results
The mean percentage of attendance for 24 exercise training sessions was 86.7 ± 12.7%. All subjects continued this aquatic training through the full length of the study without impairment, injury, or other problematic condition.
Table 2 shows the changes in physical characteristics, fitness parameters, and POMS scores in both groups. In the resistance group, parameters of sit-and-reach, muscle strength of the triceps surae, TUG, 5-m maximum walking speed, and POMS score of fatigue (F) were significantly improved by aquatic exercise training. In the non-resistance group, only sit-and-reach, muscle strength of the triceps surae, and TUG were significantly improved.
Differences between before and after aquatic exercise training in physical characteristics, fitness parameters, and POMS scores in both groups are shown in Table 3. The 5-m maximum walking speed (P < 0.01), 10-m obstacle walking time (P < 0.05), and length with eye-open (P < 0.05) exhibited significant improvements in the resistance group compared to the non-resistance group. The rate of improvement in muscle strength of plantar flexion in the resistance group tended to be higher than that in the non-resistance group (Fig. 2). Additionally, in the resistance group, the rate of improvement of TUG was significantly correlated with the that of decrease in tension/anxiety indicated by POMS score (Fig. 3). However, in the non-resistance group, no correlation was observed between these parameters.

Comparison between resistance and non-resistance group: a 5-m maximum walking speed, b 10-m obstacle walking, c length with eye-open, and d rate of improvement in muscle strength of plantar flexion

Correlations of changes in timed up and go and changes in POMS score (tension/anxiety) in resistance group
Discussion
An aquatic exercise training, using water resistance equipment, was administered for 2 months to 20 healthy elderly individuals using a small pool in a city daycare facility. Irrespective of the use of water resistance equipment, significant improvements were observed in both groups in strength of plantar flexion, an indicator of leg muscle strength, and the TUG test, which assesses functional balance in everyday life. Furthermore, 10-m obstacle walking and 5-m maximum walking speed were significantly improved in the resistance group compared with the non-resistance group.
The first finding with the present aquatic exercise training was increased in strength of plantar flexion in both groups. This effect tended to be stronger in the resistance group than in the non-resistance group. We concluded that plantar flexion strength increased because of an increase in triceps surae strength. The triceps surae mainly functions to maintain standing posture and flex the ankle (Tokuno et al. 2007), and while walking it plays an important role in pushing off the ground with the toes. A previous study found that high-intensity plantar flexion training in the elderly increased triceps surae strength and activity (Simoneau et al. 2007). The present aquatic exercise training consisted mostly of walking training, such as long-stride walking, side walking, and kick walking. Thus, during the exercise training, the participants often exercised by pushing off the bottom of the pool with the toes. Furthermore, on kicking the leg forward in the water, water resistance causes the triceps surae of the trailing leg to become tense and support the body as the floor is gripped by the toes. Thus, exercising, frequent plantar flexion training, i.e., pushing off the floor with the toes and supporting the body, applied a great deal of stress to the triceps surae, and thus increased muscle strength. In the resistance group, muscle strength tended to increase, because this effect was further enhanced.
Compared with the non-resistance group, improvements in 5-m maximum walking speed and 10-m obstacle walking were significantly greater in the resistance group. In the 5-m maximum walking speed test, subjects walk as fast as they can, and maximum walking speed reflects motor performance, including lower muscle strength and flexibility. Moreover, in the 10-m obstacle walking test, subjects walk over obstacles, and this requires not only lower muscle strength and flexibility but also balance, precision, and speed. Both parameters thus represent overall physical fitness as reflected in walking ability, and improvement of overall physical performance in the resistance group was the most important effect of the aquatic exercise training using this resistance equipment. While kicking the legs up or walking fast in the water with the resistance equipment, it is necessary to exert considerable strength in a short period of time. Furthermore, compared with the non-resistance group, strong water resistance caused the body to sway, making it necessary to correct posture. Therefore, compared to the non-resistance group, the resistance group had more opportunities to correct body sway during exercising, and thereby exert more muscle strength. Consequently, it became easier for the resistance group to push off the ground and correct body sway while walking on land, and leading to improvements in 5-m maximum walking speed and 10-m obstacle walking, which involve muscle strength, flexibility, and balance function.
The second finding with the present aquatic exercise training was to significantly shorten TUG in both groups. Furthermore, length with eye-open in the resistance group significantly improved compared to the non-resistance group. These parameters are used to assess balance function. In particular, TUG indicates functional balance in everyday living activities, such as maintenance of standing posture, getting up, one-leg standing, and walking, and can be used to evaluate dynamic balance (Podsiadlo and Richardson 1991). When the elderly arise from a chair or change direction, their posture becomes unstable, and they often fall. However, in the water, because resistance of the water changes depending on walking speed, it is possible to adjust the exercise intensity. Compared to slow movements, such as walking (Ferrell 1998), the body is subjected to greater levels of water resistance with movements that require use of great muscle strength in a short period of time, such as speed walking and kicking forward, thus causing postural instability. Previous studies have found that by exercising in the water, where buoyancy makes it difficult to support the body, people can experience postural instability and improve dynamic balance (Devereux et al. 2005; Simmons and Hansen 1996). Furthermore, the finding of shortening of length with eye-open in the resistance group indicates improvement of static balance function. It is possible to tense each muscle group in the legs and trunk and correct postural instability utilizing the viscosity of water. In our aquatic exercise training, the elderly participants exercised by walking in water, and water resistance caused postural instability. Therefore, both dynamic and static balance improved as a result of simultaneous stimulation of not only the leg muscles but also the support muscles involved in spinal and pelvic movements.
Furthermore, with the aquatic exercise training using water-resistance equipment, a low negative correlation was found between the degree of change in TUG and the degree of change in POMS (T–A) scores. This shows that tension and anxiety in everyday living decreased in participants in whom aquatic exercise shortened TUG (Podsiadlo and Richardson 1991). As it became easier to maintain posture, stand up, and move, tension and anxiety in everyday life tended to be alleviated.
There are some potential limitations in this study. First, 11 participants dropped out during the study period due to trouble in home, falls out of the training time, absence of measurement, high exercise frequency as three times/week and infectious disease. In this aquatic training program, one of the causes of drop-out was the high frequency of training (such as three times/week), and not just only exercise intensity. We believe that exercise frequency (e.g. two times/week) suited for this elderly population to continue exercise training without drop out. The second limitation of this study is that length with eye-open and 10-m obstacle walking in the resistance group were significantly improved compared to the non-resistance group, but these items were not significantly improved from baseline data after the training session. For this reason, we selected the subjects in this study from generally living at home elderly, so we think the base line data of length with eye-open was dispread with larger standard deviation. The changes associated with training were not significant compared with baseline data.
As far as exercise safety was concerned, in the water buoyancy and viscosity lower the forces applied to body mass-bearing joints, such as the knee, and as a result the aquatic exercise did not damage muscles and joints. Moreover, in the present aquatic exercise training, the level of intensity was set at “moderately strong”. With land-based muscle strength training, excessive force on muscles can lead to muscle injury (Roth et al. 2000). However, in the water, resistance increases in relation to speed, and even when intensity is increased the risk of overload is low. It has been reported that the incidence of injury is lower for swimmers than for athletes who perform aerobic exercise on land (Pantoja et al. 2009), suggesting that aquatic exercise is safer than land-based exercise. The present study suggests that the elderly can also safely perform the present aquatic exercise training using water-resistance equipment.
Conclusion
The present aquatic exercise training using water-resistance equipment for the elderly are able to improve the physical fitness as reflected in balance function, walking ability (5-m maximum walking speed and 10-m obstacle walking), and tension and anxiety score of POMS. These data suggested the possibility of prevention of falls by the elderly.
References
Devereux K, Robertson D, Briffa NK (2005) Effects of a water-based training on women 65 years and over: a randomised controlled trial. Aust J Physiother 51:102–108
Ferrell KM (1998) Aquatics for people with arthritis. Lippincotts Prim Care Pract 2:102–104
Greenlund LJ, Nair KS (2003) Sarcopenia-consequences, mechanisms, and potential therapies. Mech Ageing Dev 124:287–299
Gusi N, Tomas-Carus P, Häkkinen A, Häkkinen K, Ortega-Alonso A (2006) Exercise in waist-high warm water decreases pain and improves health-related quality of life and strength in the lower extremities in women with fibromyalgia. Arthritis Rheum 55:66–73
Hauer K, Rost B, Rütschle K, Opitz H, Specht N, Bärtsch P, Oster P, Schlierf G (2001) Exercise training for rehabilitation and secondary prevention of falls in geriatric patients with a history of injurious falls. J Am Geriatr Soc 49:10–20
Konlian C (1999) Aquatic therapy: making a wave in the treatment of low back injuries. Orthop Nurs 18:11–18
Landers KA, Hunter GR, Wetzstein CJ, Bamman MM, Weinsier RL (2001) The interrelationship among muscle mass, strength, and the ability to perform physical tasks of daily living in younger and older women. J Gerontol A Biol Sci Med Sci 56:B443–B438
Liu-Ambrose T, Khan KM, Eng JJ, Janssen PA, Lord SR, McKay HA (2004) Resistance and agility training reduce fall risk in women aged 75 to 85 with low bone mass: a 6-month randomized, controlled trial. J Am Geriatr Soc 52:657–665
Moening D, Scheidt A, Shepardson L, Davies GJ (1993) Biomechanical comparison of water running and treadmill running. Isokinet Exerc Sci 3:207–215
Pantoja PD, Alberton CL, Pilla C, Vendrusculo AP, Kruel LF (2009) Effect of resistive exercise on muscle damage in water and on land. J Strength Cond Res 23:1051–1054
Podsiadlo D, Richardson S (1991) The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39:142–148
Potier TG, Alexander CM, Seynnes OR (2009) Effects of eccentric strength training on biceps femoris muscle architecture and knee joint range of movement. Eur J Appl Physiol 105:939–944
Roth SM, Martel GF, Ivey FM, Lemmer JT, Metter EJ, Hurley BF, Rogers MA (2000) High-volume, heavy-resistance strength training and muscle damage in young and older women. J Appl Physiol 88:1112–1118
Sayer AA, Syddall HE, Martin HJ, Dennison EM, Anderson FH, Cooper C (2006) Falls, sarcopenia, and growth in early life: findings from the Hertfordshire cohort study. Am J Epidemiol 164:665–671
Shono T, Fujishima K, Hotta N, Ogaki T, Ueda T (2001) Physiological responses to water-walking in middle aged women. J Physiol Anthropol Appl Human Sci 20:119–123
Shono T, Masumoto K, Fujishima K, Hotta N, Ogaki T, Adachi T (2007) Gait patterns and muscle activity in the lower extremities of elderly women during underwater treadmill walking against water flow. J Physiol Anthropol 26:579–586
Simmons V, Hansen PD (1996) Effectiveness of water exercise on postural mobility in the well elderly: an experimental study on balance enhancement. J Gerontol A Biol Sci Med Sci 51:M233–M238
Simoneau E, Martin A, Van Hoecke J (2007) Adaptations to long-term strength training of ankle joint muscles in old age. Eur J Appl Physiol 100:507–514
Suomi R, Koceja DM (2000) Postural sway characteristics in women with lower extremity arthritis before and after an aquatic exercise intervention. Arch Phys Med Rehabil 81:780–785
Tokuno CD, Carpenter MG, Thorstensson A, Garland SJ, Cresswell AG (2007) Control of the triceps surae during the postural sway of quiet standing. Acta Physiol 191:229–236
Tokuno CD, Garland SJ, Carpenter MG, Thorstensson A, Cresswell AG (2008) Sway-dependent modulation of the triceps surae H-reflex during standing. J Appl Physiol 104:1359–1365
Wang TJ, Belza B, Elaine Thompson F, Whitney JD, Bennett K (2007) Effects of aquatic exercise on flexibility, strength and aerobic fitness in adults with osteoarthritis of the hip or knee. J Adv Nurs 57:141–152
Wolfson L, Judge J, Whipple R, King M (1995) Strength is a major factor in balance, gait, and the occurrence of falls. Health Soc Work 50:64–67
Acknowledgments
We would like to thank the subjects who participated in the present study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Jean-René Lacour.
Rights and permissions
About this article
Cite this article
Katsura, Y., Yoshikawa, T., Ueda, SY. et al. Effects of aquatic exercise training using water-resistance equipment in elderly. Eur J Appl Physiol 108, 957–964 (2010). https://doi.org/10.1007/s00421-009-1306-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-009-1306-0