
Abstract
This study assessed interactions between mild/moderate muscle pain and inertial load on the control of human elbow-flexion movements. It is hypothesized that high inertial load combined with moderate muscle pain intensity affect the motor control more than for low inertial-load combined with low-intensity pain. Fifteen subjects performed horizontal pointing movements (70° range) under three load conditions: 0, 4, and 10 kg. Pain was induced by injection of 0.5 ml and 1.5 ml hypertonic saline into the biceps muscle. Subjects scored the muscle pain intensity on a visual analogue scale (VAS). Elbow joint position, VAS, and the electromyograms (EMG, m. biceps brachii, m. triceps brachii, m. brachioradialis, and m. trapezius) were recorded. Mild and moderate muscle pain attenuated acceleration profiles [6.1(0.9)%], effective movement amplitude [3.2 (0.7)%], peak velocity [5.8 (0.9)%] and prolonged the reaction time [21 (5)%]. No interaction between muscle pain intensity and inertial load was found for the kinematic parameters. EMG profiles from m. biceps brachii, m. triceps brachii, and m. brachioradialis were similarly attenuated [10.2 (0.80)%] by mild and moderate muscle pain in all inertial load conditions. For high inertial load, the initial agonist EMG burst activity was more attenuated [50 (5.3)%] by moderate muscle pain compared with mild muscle pain [34 (4.2)%]. These data suggest that for high effort-demanding tasks muscle pain differently affects the motor planning according to the pain-intensity level. Perturbations of motor planning lead to changes on movement strategies, which might be a potential cause of musculoskeletal problems.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Interactions between musculoskeletal pain (chronic and acute) and movement control have been investigated due to the pronounced socio-economic impact as well as the potential effects on athletes’ performance and rehabilitation programs (Ahern et al. 1988; Veiersted et al. 1990; Birch et al. 2000; Weerakkody et al. 2003).
Clinical studies, mainly related to low back pain, have extensively investigated changes on the motor control caused by chronic pain conditions (Kravitz et al. 1981; Nouwen and Bush 1984; Ahern et al. 1988). Radebold et al. (2000, 2001) showed that chronic low back pain can prolong response time of trunk muscles and change response pattern to sudden load release compared with healthy subjects. Declining integrated EMG during 3 min of trunk flexion–extension movements was found in healthy subjects in contrast to chronic low back pain patients who presented constant integrated EMG (Robinson et al. 1992). Furthermore, cleaners suffering from chronic trapezius myalgia presented decreased endurance of the forward flexor muscles compared with healthy subjects (Larsson et al. 2000). In experimental pain studies the motor control has also been shown to be changed by muscle pain. During experimentally induced muscle pain the motor-unit firing rate was inversely significantly correlated with the subjective scores of pain intensity (Farina et al. 2004). The level of maximal voluntary contraction was decreased by experimental muscle pain (Graven-Nielsen et al. 1997). However, sub-maximal contractions during experimental pain showed no changes in EMG activity and force, but reduced the endurance time compared to a non-painful condition (Ashton-Miller et al. 1990; Graven-Nielsen et al. 1997; Ciubotariu et al. 2004). Moreover, acute muscle pain has been shown to change the motor planning for step initiation (Madeleine et al. 1999a), the muscle coordination during gait (Arendt-Nielsen et al. 1996; Graven-Nielsen et al. 1997), and mastication (Svensson et al. 1997, 1998a). Finally, Birch et al. (2000) concluded that experimental muscle pain had no effect on work performance when using a computer mouse but did modulate muscle activity during a low-precision task while no effect was found during high-precision task. In line, experimentally induced muscle pain did not change the overall EMG activity during high-precision elbow-joint movements but caused EMG activity changes in the overall muscle activity and in the initial EMG burst during low-precision tasks, which suggests changes in the motor planning (Ervilha et al. 2004). Thus, it is clear that the motor strategy is disturbed by muscle pain.
Movements performed with additional inertial load have greater duration, present higher agonist and antagonist muscles activity, and decreased acceleration profiles, which might represent changes on motor planning (Corcos et al. 1989; Khan et al. 1999). However, only few studies have related motor control changes caused by muscle pain with the mechanical motor-task demand and/or the pain-intensity level.
The aim of the present human experimental study was to investigate the effect of mild and moderate muscle pain on the motor control strategies related to elbow-flexion movements performed with various inertial loads. It was hypothesized that the higher inertial-load and pain-intensity the higher the disturbance in the movement control.
Methods
Subjects
Fifteen subjects [eleven men, four women; mean (SD) age 26 (5) years, height 1.75 (0.09) m, and body mass 70 (11) kg] participated in the experiment. All subjects had no known history of locomotor apparatus disorder or musculoskeletal pain disorders. Volunteers received information about the experiment and subsequently written consents were obtained prior to inclusion. The study was approved by the local Ethics Committee and conduced according to the Helsinki Declaration. The experimental procedures used comply with the current laws in Denmark.
Apparatus and movement
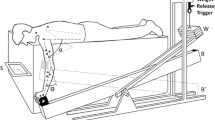
Horizontal elbow flexion movements (70° range) were performed on a manipulandum aiming at a 22°-wide target. Subjects were seated comfortably with the dominant arm in semi-prone position, strapped at an adjustable support and fixed at 45° of shoulder horizontal flexion in 90° of abduction. Shoulder angles were defined relative to the coronal plane with 0° corresponding to the arm aligned with this plane. The forearm was strapped to a light manipulandum positioned horizontally aligned with the arm support (Fig. 1). The elbow joint was positioned just above the fulcrum of the manipulandum so that only horizontal movements were permitted. The subjects were grasping a handle and were instructed to do the movements as fast and as accurately as possible immediately after hearing a beep signal (300 Hz) returning to the initial position after a second beep (600 Hz). The time between the first and second beep was fixed to 1.9 s and the time between the second beep and the next go-beep was randomized in a range from 7 to 13 s. The upper limb position was set at 45° of horizontal shoulder flexion and 115° of elbow flexion (full elbow extension equals 0°). Visual feedback of the elbow position as well as the target width and the range of motion to be performed were provided on an oscilloscope.

Experimental setup. The oscilloscope was positioned in front of the subject showing elbow movements based on electrogoniometer recordings. The final position was 115° whereas the initial position was set at 45°
Protocol
Two sessions took place 1 week apart. In one session ten elbow-flexion trials were performed with no extra load and with 4 kg added to the tip of the manipulandum in each of the four following conditions: (1) before experimental muscle pain, (2) during mild muscle pain, (3) during moderate muscle pain, and (4) 20 min after the pain had completely vanished. The sequence of conditions two and three were randomized. In another session ten elbow-flexion trials were performed with 10 kg added to the tip of the manipulandum, and the four conditions described above were repeated. The order of the sessions was randomized.
Experimental muscle pain
A bolus of 0.5 ml or 1.5 ml sterile hypertonic saline (5.8%) was injected intramuscularly into biceps muscle (lateral head), at a rate of 90 ml h−1, via a disposable stainless needle (27 g, 40 mm) connected via a tube (IVAC, G30303) to an infusion pump (ALARIS medical systems, Asena, UK). A 10-cm electronic, visual analogue scale (VAS) where 0 cm indicated “no pain” and 10 cm “intolerable pain” was used to score the pain intensity. The signal from the VAS was recorded continuously. The subjects were allowed to adjust the values using the hand not involved in the exercise and they were asked to focus on the VAS in the breaks between the individual trials. The mean VAS scores obtained during and between the trials were calculated.
Kinematic and EMG recordings
Angular position of the elbow joint and electromyograms (EMG) from m. trapezius (upper fibers), m. biceps brachii (long head), m. triceps brachii (lateral head), and m. brachioradialis were recorded. The EMG intensity of each muscle was normalized by the respective peak (average of two trials) of maximal voluntary isometric contraction recorded before the first set of trials.
An electrogoniometer (Biometrics SG110, Ladysmith, Vt.) was used to measure elbow angular position. A pair of surface electrodes (Medicotest 72001-k, ØLstykke, Denmark) was placed in the direction of the muscle fibers (2 cm apart) on shaved, abraded cleaned skin, as follows. (1) Trapezius muscle (upper portion)—2 cm lateral to the midpoint of the lead-line between the angle of the acromion and the spinal process of the seventh vertebra. (2) Biceps brachii (long head)—on the lead-line between the acromion and the fossa cubit at one-third from the fossa cubit. (3) Triceps brachii (lateral head)—1 cm lateral to the lead-line just on the mid-point between the acromion and the olecranon process. (4) Brachioradialis—on the muscle belly, 5 cm distally from the elbow joint. The EMG signals were bandpass filtered (second order, 20–500 Hz), amplified (1,000–10,000 times; CounterPoint MK2, Dantec, Skovlunde, Denmark) and sampled at 2 kHz.
Pain intensity (VAS), electrogoniometric, electromyographic, and beep signals were acquired in parallel by an analog/digital converter and stored on a personal computer.
Data analysis
Angular position was digitally filtered (low-pass, fourth order, and zero-phase-lag Butterworth filter with a 10-Hz cut-off frequency) and differentiated to obtain velocity and acceleration. Acceleration and EMG onset were automatically determined by a threshold procedure.
EMG signals were digitally band-pass filtered from 20 to 400 Hz (Butterworth), full-wave rectified, low-pass filtered (Butterworth) with a 50-Hz cut-off frequency and normalized by the maximal voluntary isometric contraction. Extracted parameters from individual trials:
-
1.
Integrated EMG amplitude over three epochs. Epoch 1: the EMG integral of 100 ms before onset of the m. biceps brachii EMG (pre-movement epoch). Epoch 2: the EMG integral from the biceps muscle EMG activity onset to the acceleration offset (movement epoch). Epoch 3: the EMG integral of 100 ms after epoch 2 (post-movement epoch). Epoch 2 was time normalized (divided by duration and multiplied by 100).
-
2.
Q 100: the integrated EMG profile (IEMG) from the m. biceps brachii activity onset to 100 ms.
-
3.
Effective movement amplitude: angular displacement between acceleration onset and acceleration offset.
-
4.
Movement time: the time from the acceleration onset to the acceleration offset.
-
5.
Peak velocity.
-
6.
Integrated acceleration profiles: the integral of acceleration from the acceleration onset to the acceleration offset.
-
7.
Reaction time: the time between the go-beep signal and the acceleration onset.
All parameters were averaged across ten trials.
Statistical analysis
Data are presented as means (SEM). Two-way repeated ANOVAs were used to examine the effects of load (0, 4, and 10 kg) and conditions (pre-pain, mild pain, moderate pain, and post-pain) on all parameters. When the ANOVA was found significant, the Student-Newman-Keuls (SNK) post hoc test was used for multiple comparisons. A significance level of P<0.05 was accepted.
Results
Injection of 1.5 ml hypertonic saline induced significantly more pain [VAS: 3.0 (0.6) cm] compared with 0.5 ml [VAS: 1.7 (0.5) cm; ANOVA: F 1,14=19, P<0.01]. The pain intensity was not different between the various loads (0, 4, 10 kg) for the two boli of same volume.
Kinematic parameters
Increasing inertial load impaired the movement kinematics inducing significantly (F 2,28=8.4, P<0.02, SNK: P<0.04) increased movement time in addition to significantly decreased acceleration profiles (F 2,28=171.5, P<0.001, SNK: P<0.001) and peak velocity (F 2,28=15, P<0.01, SNK: P<0.03). The kinematic parameters did not show significant interaction between load and pain intensity.
The integrated acceleration profiles, in both positive and negative phases and in all load conditions, were significantly (F 3,42>4.0, P<0.03) decreased in both pain conditions compared with pre-pain. The negative acceleration phase was also significantly (F 3,42>5.2, P<0.02) decreased during mild and moderate pain compared with post-pain (Fig. 2).

Mean (SEM) integrated acceleration (positive and negative phases). Data from three loads (0, 4, and 10 kg) added to the manipulandum. Integrated acceleration is significantly different among load conditions. Elbow flexions of 70° range to a 22° target-width. Before (open columns), during mild (gray columns) and moderate (hatched columns) intensity muscle pain and post-pain (filled columns) are shown. *Significantly different from pre-pain. #Significantly different from post-pain in the same load condition [Student-Newman-Keuls (SNK): P<0.05]
The effective movement amplitude was decreased in both pain conditions and in all load conditions compared with pre-pain (F 3,42>3.7, P<0.02). The movement time during pain was also significantly (F 3,42>5, P<0.02) increased compared with pre and post-pain (Table 1). During both pain conditions the peak velocity was significantly (F 3,42>4.6, P<0.02) decreased compared with the pre-pain condition and moderate pain induced significant decreased peak velocity compared with the post-pain condition as well.
The reaction times during mild and moderate pain, in all load conditions, were significantly (F 3,42>11.7, P<0.05) increased when compared with pre- and post-pain conditions. In addition, during the post-pain condition reaction time was significantly (F 3,42>13, P<0.04) longer compared with pre-pain (Table 1).
Integrated EMG
The overall EMG profiles were significantly increased when the inertial load was increased (F 2,28=3.1, P<0.04, SNK: P<0.05). However, there was no significant interaction between load and pain intensity. Thus, they will be presented as pooled data from the three load conditions.
Experimentally induced muscle pain significantly (F 3,42=3.0, P<0.05) decreased IEMG during elbow-flexion movements (Fig. 3). During movement (epoch 2) mild and moderate pain significantly (F 3,42=3.5, P<0.05) attenuated the IEMG of m. biceps brachii, m. triceps brachii, and m. brachioradialis compared with the pre-pain condition. For the biceps muscle, the IEMG during pain conditions were also significantly (F 3,42=4, P<0.03) decreased compared with the post-pain condition. In epoch 3 the IEMG for m. biceps brachii, m. triceps brachii, and m. brachioradialis were significantly (F 3,42=13, P<0.01) attenuated during post-pain and also during pain conditions compared with the pre-pain condition.

Mean (SEM) integrated EMG (IEMG) from m. biceps brachii (BB), m. triceps brachii (lateral head; TB), m. brachioradialis (BR), and m. trapezius (TZ). Pooled data from three loads (0, 4, and 10 kg) added to the manipulandum. Data from flexions of 70° range to a 22° target-width. Before (open columns), during mild (gray columns) and moderate (hatched columns) intensity muscle pain and post-pain (filled columns) are shown. Epoch 1: integrated 100 ms before the movement. Epoch 2 (movement epoch): integrated EMG from the biceps muscle activity onset to the acceleration offset. The IEMG was normalized to the epoch duration and to the maximum voluntary isometric contraction (MVIC). Epoch 3: integrated 100 ms after the movement. *Significantly different from pre-pain. #Significantly different from post-pain (SNK: P<0.05)
Initial agonistic EMG activity
In each load condition experimentally induced muscle pain significantly (F 3,42=2.2, P<0.05, SNK: P<0.05) attenuated the initial Q 100 of biceps brachii muscle during elbow flexion movements when compared with pre-pain condition (Fig. 4). Post-pain Q 100 was also significantly (F 3,42=17, P<0.01) attenuated compared with pre-pain for all load conditions and significantly (F 3,42=20, P<0.01, SNK: P<0.05) enhanced compared with moderate-pain level for the 10-kg condition. At this condition (10-kg) Q 100 was significantly (F 6,84=2.2, P<0.05, SNK: P<0.05) decreased during moderate pain compared with mild pain.

The integral of the BB IEMG burst over 100 ms from the EMG onset (Q 100 ). Data from flexions of 70° range to a 22° target-width. Before (open columns), during mild (gray columns) and moderate (hatched columns) intensity muscle pain and post-pain (filled columns) are shown. *Significantly different from pre-pain. #Significantly different from mild and post-pain (SNK: P<0.05)
Discussion
The effects of combined pain-intensity levels and inertial loads on the control of elbow-flexion movements were investigated. Mild and moderate pain in the biceps brachii muscle lowered the EMG activity profiles of agonists (m. biceps brachii), synergists (m. brachioradialis) as well as the antagonist (m. triceps brachii) with consequent adjustments in kinematic parameters, e.g. decreased elbow joint acceleration profiles, lower effective movement amplitude, and longer reaction time. Furthermore, for high inertial-load tasks, moderate muscle pain strongly attenuated the initial agonist EMG burst when compared with mild muscle pain, which suggests that for high effort-demanding tasks muscle pain differently affects the motor planning according to the pain-intensity level.
Kinematic parameters
In line with the present study, it has previously been found that the addition of inertial load impairs the movement lowering the acceleration profiles and peak velocity with consequent enlargement of movement time (Gottlieb et al. 1989; Pfann et al. 1998; Vernazza-Martin et al. 1999; Khan et al. 1999). Mild and moderate muscle pain, during movements performed with various inertial loads, acted as additional movement impairment. In all combinations of inertial load and pain intensity, the integrated acceleration and the peak velocity were attenuated by muscle pain. The lack of differences according to the pain intensity might be due to voluntary readjustment based on a complex interaction between voluntary capability to adjust minor effects caused by pain and changes on motor planning. Nonetheless, adjustments in the movement kinematic parameters during pain conditions illustrate patent movement impairment. This is in line with Howell et al. (1985) who showed a decreased elbow-joint range of motion caused by post-exercise muscle soreness, Ahern et al. (1988) and Zedka et al. (1999) who respectively concluded that chronic and acute back pain restrict trunk motion; and Madeleine et al. (1999a) who showed that acute muscle pain modulates muscle activity and work performance during standardized, low load, repetitive work tasks.
The time from a given stimulus to the beginning of muscle response is defined as reaction time (Dickstein et al. 1993). Delayed reaction time has been found after musculoskeletal injuries (Taimela and Kujala 1992). Experimental (Madeleine et al. 1999b; Ervilha et al. 2004) and clinical (Radebold et al. 2000, 2001; Hodges 2001) studies have shown that the reaction time is systematically prolonged during acute and chronic pain conditions. Moreover, Luoto et al. (1998) showed that the severity of low-back pain is associated with longer reaction times. This is however in contrast to the present study where the reaction time generally was prolonged by muscle pain but the impairment was not correlated to the pain intensity. In a psychomotor task, information processing is considered to include at least three main stages between the presentation of a stimulus and the (motor) response to it (Schmidt 1988). The first stage is the stimulus identification that includes the reception of a stimulus by sense organs and preliminary analyses of its features. The second stage is the response selection stage, which includes decision mechanisms leading to the choice of response. Finally, the third stage is the response programming that is associated with translating the abstract idea of a response into muscular action that will achieve it. The present data do not show in which of the three above cited information processing stages experimental muscle pain acts to cause delayed reaction time. However, in addition to delayed reaction time the response programming, illustrated by the initial EMG burst, is attenuated.
Integrated EMG
Epoch 1 represents the time interval of 100 ms immediately before the m. biceps brachii EMG onset and shows the muscle activity when the arm is motionless, nearly resting. Experimentally induced muscle pain did not change muscle activation during epoch 1, which contradicts the pain–spasm–pain model first proposed by Travell et al. (1942). This model predicts muscle activity enhancement (muscle spasm) as a mechanism to avoid movement of the sore segment, which in turn causes more pain forming the bases of a vicious pain–spasm–pain cycle. In a previous study, Ervilha et al. (2004) showed higher trapezius muscle pre-movement activation in only one out of four combinations of range of motion and target size during planar elbow-joint movements. However, the pre-movement muscle activity was in general not increased by experimentally induced muscle pain, which is in line with the present study. Moreover, increased resting EMG activity has not been found in many well-controlled studies (Kravitz et al. 1981; Nouwen and Bush 1984; Graven-Nielsen et al. 1997; Svensson et al. 1998b).
The most effective way to impair the movement is to decrease the agonistic muscle activity at the same time as the antagonistic muscle activity is increased. This situation is predicted in the pain-adaptation model proposed by Lund et al. (1991). During gait, pain in gastrocnemius muscle decreased the EMG activity in that muscle and increased the EMG activity of the antagonistic phase of m. tibialis anterior. The reverse occurred when pain was induced in m. tibialis anterior (Graven-Nielsen et al. 1997). Other studies presented evidences that the agonistic muscle activity is decreased during pain condition, but failed to show increased antagonistic muscle activity (Schwartz and Lund. 1995; Birch et al. 2000) or even showed decreased antagonistic muscle activity as well (Ervilha et al. 2004). Nevertheless, decreasing only the agonistic or both agonistic and antagonistic muscle activity at the same time also impairs the movement though in a less effective manner. The present data show that the overall EMG activity of the agonistics (m. biceps brachii and m. brachioradialis) and the antagonistic elbow flexor muscles were simultaneously attenuated by pain in the biceps muscle. This was the case during epoch 2 (movement epoch) and also during epoch 3 (post-movement epoch). Reduced muscle activity in both painful muscles as well as in the non-painful synergists has been shown in isometric contractions (Ciubotariu et al. 2004). In the present study, agonistic, antagonistic, and synergistic EMG activities were generally attenuated during muscle pain for a large range of movement performed to a large target, which is in contrast to a previous study where decreased muscle activity only was found during small range of movement aiming at a large target (Ervilha et al. 2004). The different findings between the present and previous study are probably a consequence of the experimental settings. In both studies the subjects performed horizontal elbow-flexion movements on a manipulandum but a handgrip was allowed only in the present study. It has been shown that for elbow-joint pointing movements slight changes in the setup can modify the EMG relationship among the involved muscles, mainly changing the amplitude of the second agonistic EMG burst during pointing movements (Gottlieb et al. 1989). For pointing movements performed with a handle grasp one can speculate that the EMG signal variability will be less pronounced compared to pointing movements performed with no hand grasping.
There was no significant interaction between pain-intensity levels and inertial loads on the overall EMG activity. Farina et al. (2004) showed that experimental muscle pain can cause decreased motor unit firing rate correlated to the pain intensity. The lack of interaction between pain-intensity and inertial load for the overall EMG activity in the present study suggests that changes caused by pain might be partially voluntarily overruled.
Initial agonistic EMG activity
The Q 100 represents the central nervous system excitation output giving an indication of the initial rate of recruitment and firing rates of alpha motoneurons (Gottlieb et al. 1989). In the present study Q 100 was systematically decreased during muscle pain suggesting that pain affects the motor programming, which is in line with previous finding reported by Ervilha et al. (2004). Interestingly, Q 100 was the only investigated parameter to show different attenuation rates according to the pain intensity and the inertial load. It was strongly attenuated during moderate muscle pain compared with mild pain (for 10-kg trials), which is in line with a study showing that progressively increased muscle pain intensity causes a gradual decrease of motor units firing rate (Farina et al. 2004). Possibly, there is no time for voluntary compensation in order to overcome pain changes on motor programming for the initial agonist EMG burst. Previous studies (Gottlieb et al. 1989; Corcos et al. 1989; Gottlieb 1998) have shown that the initial agonist EMG activity varies in diverse ways according to distinct external task demands such as target size, range of motion, and inertial load (see Gottlieb et al. 1989 for review). Therefore, decreased Q 100 during pain conditions (whether mild or moderate pain) compared with pre-pain indicates that pain acts as a potential movement restrictor that could lead to erratic movements which might, at long-term, perpetuate or even generate musculoskeletal problems. Finally, the significant difference in Q 100 between mild and moderate pain for the heavy inertial-load trials suggests that at high force demand, as present in many occupational and sports activities, the motor programming might be more attenuated by muscle pain. The present findings are based on effects of acute muscle pain where the muscle pain intensity is independent of the actual muscle activity. The relevance of such findings in case of e.g. muscle injury where muscle pain is correlated to the muscle activity level is not known.
Conclusion
The present study showed that for elbow-joint flexion movements mild and moderate acute muscle pain attenuates agonistic, antagonistic, and synergistic EMG activities with consequent changes on the movement kinematics. Mild and moderate experimental muscle pain differently affects the motor programming for high-force demand tasks. Moreover, the impairment of reaction time may have clinical importance and this finding need to be further investigated. Finally, perturbations on motor planning lead to changes on movement strategies, which might be a potential cause of musculoskeletal problems.
References
Ahern DK, Follick MJ, Council JR, Laser-Wloston N, Litchman H (1988) Comparison of lumbar paravertebral EMG patterns in chronic low back pain patients and non-patient controls. Pain 34:153–160
Arendt-Nielsen L, Graven-Nielsen T, Svanner H, Svensson P (1996) The influence of low back pain on muscle activity and coordination during gait: A clinical and experimental study. Pain 64:231–240
Ashton-Miller JA, McGlashen KM, Herzenberg JE, Stohler CS (1990) Cervical muscle myoelectric response to acute experimental sternocleidomastoid pain. Spine 15:1006–1012
Birch L, Graven-Nielsen T, Christensen H, Arendt-Nielsen L (2000) Experimental muscle pain modulates muscle activity and work performance differently during high and low precision use of a computer mouse. Eur J Appl Physiol 83:492–498
Ciubotariu A, Arendt-Nielsen L, Graven-Nielsen T (2004) The influence of muscle pain and fatigue on the activity of synergistic muscles of the leg. Eur J Appl Physiol (in press)
Corcos DM, Gottlieb GL, Gyan CA (1989) Organizing principles for single-joint movements II. A speed-sensitive strategy. J Neurophysiol 62:358–368
Dickstein R, Hocherman S, Amdor G, Pillar T, Winstein CJ, Pohl PS, Wolf SL (1993) Reaction and movement times in patients with hemiparesis for unilateral and bilateral elbow flexion. Phys Ther 73:374–385
Ervilha UF, Arendt-Nielsen L, Duarte M, Graven-Nielsen T (2004) The effect of muscle pain on elbow flexion and co-activation tasks. Exp Brain Res (in press)
Farina D, Arendt-Nielsen L, Merletti R, Graven-Nielsen T (2004) The effect of experimental muscle pain on motor unit firing rate and conduction velocity. J Neurophysiol 91:1250–1259
Gottlieb GL (1998) Muscle activation patterns during two types of voluntary single-joint movement. J Neurophysiol 80:1860–1867
Gottlieb GL, Corcos DM, Agarwal GC (1989) Strategies for the control of voluntary movements with one mechanical degree of freedom. Behav Brain Sci 12:189–210
Graven-Nielsen T, Svensson P, Arendt-Nielsen L (1997) Effects of experimental muscle pain on muscle activity and co-ordination during static and dynamic motor function. Electroencephalogr Clin Neurophysiol 105:156–164
Hodges PW (2001) Changes in motor planning of feedforward postural responses of the trunk muscles in low back pain. Exp Brain Res 141:261–266
Howell JN, Chila AG, Ford G, David D, Gates T (1985) An electromyographic study of elbow motion during postexercise muscle soreness. J Appl Physiol 58:1713–1718
Khan MA, Garry MI, Franks IM (1999) The effect of target size and inertial load on the control of rapid aiming movements. Exp Brain Res 124:151–158
Kravitz E, Moore ME, Glaros A (1981) Paralumbar muscle activity in chronic low back pain. Arch Phys Med Rehabil 62:172–176
Larsson B, Bjork J, Elert J, Gerdle B (2000) Mechanical performance and electromyography during repeated maximal isokinetic shoulder forward flexions in female cleaners with and without myalgia of the trapezius muscle and in healthy controls. Eur J Appl Physiol 83:257–267
Lund JP, Donga R, Widmer CG, Stohler CS (1991) The pain-adaptation model: A discussion of the relationship between chronic musculoskeletal pain and motor activity. Can J Physiol Pharmacol 69:683–694
Luoto S, Taimela S, Alaranta H, Hurri H (1998) Psychomotor speed in chronic low-back pain patients and healthy controls: construct validity and clinical significance of the measure. Percept Mot Skills 87:1283–1296
Madeleine P, Lundager B, Voigt M, Arendt-Nielsen L (1999a) Shoulder muscle co-ordination during chronic and acute experimental neck-shoulder pain: An occupational pain study. Eur J Appl Physiol 79:127–140
Madeleine P, Voigt M, Arendt-Nielsen L (1999b) Reorganization of human step initiation during acute experimental muscle pain. Gait Posture 10:240–247
Nouwen A, Bush C (1984) The relationship between paraspinal EMG and chronic low back pain. Pain 20:109–123
Pfann KD, Hoffman DS, Gottlieb GL, Strick PL, Corcos DM (1998) Common principles underlying the control of rapid, single degree-of-freedom movements at different joints. Exp Brain Res 118:35–51
Radebold A, Cholewicki J, Panjabi MM, Patel TC (2000) Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 25:947–954
Radebold A, Cholewicki J, Polzhofer GK, Greene HS (2001) Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine 26:724–730
Robinson ME, Cassisi JE, O’Connor PD; MacMillan M (1992) Lumbar iEMG during isotonic exercise: chronic back pain patients versus controls. J Spinal Disord 5:8–15
Schmidt RA (1988) Information processing and memory systems. In: Motor control and learning: a behavioral emphasis. Human Kinetics, Champaign, Ill. pp 75–98
Schwartz G, Lund JP (1995) Modification of rhythmical jaw movements by noxious pressure applied to the periosteum of the zygoma in decerebrate rabbits. Pain 63:153–161
Svensson P, Houe L, Arendt-Nielsen L (1997) Bilateral experimental muscle pain changes electromyographic activity of human jaw-closing muscles during mastication. Exp Brain Res 116:182–185
Svensson P, Arendt-Nielsen L, Houe L (1998a) Muscle pain modulates mastication: an experimental study in humans. J Orofac Pain 12:7–16
Svensson P, Graven-Nielsen T, Matre D, Arendt-Nielsen L (1998b) Experimental muscle pain does not cause long-lasting increases in resting electromyographic activity. Muscle Nerve 21:1382–1389
Taimela S, Kujala UM (1992) Reaction times with reference to musculoskeletal complaints in adolescence. Percept Mot Skills 75:1075–1082
Travell J, Rinzler S, Herman M (1942) Pain and disability of the shoulder and arm. JAMA 120:417–422
Veiersted KB, Westgaard RH, Andersen P (1990) Pattern of muscle activity during stereotyped work and its relation to muscle pain. Int Arch Occup Environ Health 62:31–41
Vernazza-Martin S, Martin N, Cincera M, Pedotti A, Massion J (1999) Arm raising in humans under loaded vs. unloaded and bipedal vs. unipedal conditions. Brain Res 846:12–22
Weerakkody NS, Percival P, Canny BJ, Morgan DL, Proske U (2003) Force matching at the elbow joint is disturbed by muscle soreness. Somatosens Mot Res 20:27–32
Zedka M, Prochazka A, Knight B, Gillard D, Gauthier M (1999) Voluntary and reflex control of human back muscles during induced pain. J Physiol (Lond) 520:591–604
Acknowledgement
The Danish Technical Research Council has supported this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ervilha, U.F., Arendt-Nielsen, L., Duarte, M. et al. Effect of load level and muscle pain intensity on the motor control of elbow-flexion movements. Eur J Appl Physiol 92, 168–175 (2004). https://doi.org/10.1007/s00421-004-1083-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1083-8