
Abstract
Whether an arm will buckle under an impulsive end-load should partly depend on the elastic and viscous properties of the pretensed arm muscles. In measuring these properties we hypothesized that neither age, gender, nor muscle pre-contraction level would affect the bilinear elbow or shoulder lumped rotational stiffness or damping parameters in the impulsively end-loaded upper extremity of 38 healthy men and women. Subjects were instructed to preactivate triceps to either 25, 50 or 75% of maximum myoelectric activity levels. Then a standardized impulsive end-load was applied via a 6-axis load cell to the wrist of the slightly flexed arm in the prone posture. Arm kinematic responses were acquired at 280 Hz and an inverse dynamics analysis was used to estimate the bilinear rotational stiffnesses and damping parameters at the elbow and shoulder. The results show that pre-contraction level affected normalized joint rotational stiffness and damping coefficients (p < 0.02). Age affected the initial stiffness for the elbow (p < 0.05), and gender affected that of the shoulder in the sagittal plane (p < 0.006). Arm muscle strength was positively related to normalized stiffness at the elbow, but not the shoulder. We conclude that age, gender and pre-contraction level each affect the viscoelastic behavior of the end-loaded upper extremity in healthy adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The upper extremities are the first line of defense in protecting the head and torso when arresting a fall to the ground.7 Impulsive loads on the hand can be substantial, reaching 2–3 times body weight (BW) for a fall from even half standing height5,25 and 1–4 kN for a fall from standing height,9 enough to cause wrist fracture.12 To prevent the slightly flexed limb from buckling under an impulsive load applied to the hand,5,8,22 the arm muscles acting about the elbow and shoulder need to be pre-contracted to brace the arm prior to impact.6,25,26,32 This pre-contraction is required2 because the impulsive ground reaction force on the hand peaks too rapidly5,7,9,17 for a voluntary arm muscle contraction initiated at impact to develop a significant increase in resistance before the limb has already flexed under load.24 A knowledge gap addressed by the present study concerns how arm muscle pre-contraction level affects the dynamic rotational resistance of the shoulder and elbow joints when the upper extremity is impulsively end-loaded, as in a fall arrest scenario.
Because falls are a leading cause of traumatic brain injuries, particularly among the elderly over the age of 70 years,20,21 the protective use of the upper extremities in these cases clearly was either ineffectual or simply not employed. One explanation could be concern over the possibility of wrist injury when the hand is used for protection. But in other situations the hand is often used, as Vellas et al. 33 demonstrated when studying the frequency with which different parts of the body receive the main impact in a fall: these were the hand (50% males, 33% females) and buttock (18% males, 24% females), followed by the head, knee, and arm. In older women, the most common fall-related fracture sites are the upper extremity, the hip, and the trunk or neck in that order.30 For older men a similar pattern was observed although the fracture rates were halved. In either case, a better understanding of how advancing age and muscle contraction co-contraction level affect the dynamic properties of an arm braced for impact would seem useful for teaching an individual how to arrest a fall safely.
It would helpful to better understand the effect of gender on the mechanical behavior of the braced upper extremity under impulsive end-loading. Case et al. 3 examined gender differences in upper extremity kinematics and impact loading in forward falls for young female adults to compare with the previous studies for young male adults.5,26 They found that both genders employed similar initial elbow and shoulder angles at impact with the ground, but the changes for the young women’s shoulder extension and elbow flexion angles were two and four times less, respectively, than in the young men. One interpretation of these results is that the young women favored maintaining relatively extended arm postures in order to reduce the risk that their upper extremities might deflect too much, thereby allowing their head to strike the ground. This suggests that there may be a gender difference in the dynamic properties of the braced upper extremity. Indeed, at the elbow, young females have been shown to have lower rotational stiffness and damping resistance at the elbow than young male adults of the same body size.22 However, that study was limited to a single joint, the elbow, and the end-loads applied to the hand were relatively modest step increases in load. So a third knowledge gap we wished to address is the dearth of gender-specific data on the biomechanical response of the shoulder in an impulsively end-loaded extremity.
Shoulder muscle rotational stiffness and damping properties should affect the behavior of the upper extremity under impulsive load.23 This is because, anatomically, both the anterior deltoid and pectoralis major muscles can play a role in resisting shoulder abduction and extension when arresting a forward fall, while the elbow triceps brachii are the main muscles that determine the stiffness and damping properties of the elbow when it is forcibly flexed.22 However, without stereoradiography it is difficult to measure the shoulder abduction and extension angles during impact in vivo because clavicular and scapular displacements are hidden below layers of muscle. A simplifying approach, used in the present study, is to only quantify the movement of the shoulder in two planes: shoulder flexion/extension in the sagittal plane and shoulder ad-/abduction in the frontal plane.
The goal of this paper, therefore, was to test the primary hypotheses in healthy adults that neither gender, age, or level of pre-contraction affect shoulder and elbow muscle viscoelastic properties (rotational stiffness and rotational damping coefficient) of the upper extremity under an impulsive end-load. The secondary hypothesis was that the magnitude of the elbow and shoulder stiffnesses and damping properties are proportional to arm muscle strength because this information would be useful in a rehabilitation setting. We used computer simulation to calculate the stiffness and damping coefficients from the kinematic and kinetic data using an inverse dynamics optimization algorithm.
Methods
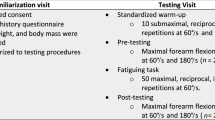
Thirty-eight healthy men and women [10 young males of mean (SD) age: 25.5 (2.7) years; 8 young females: 24.5 (3.1) years; 9 old males: 69.4 (3.4) years and 11 old females: 67.7 (2.4) years] participated in the study with written informed consent. All procedures were approvedFootnote 1 by the University of Michigan Medical School Institutional Review Board. Mean height and mass for the young males were 1.80 (0.08) m and 75.88 (6.74) kg, for the young females were 1.68 (0.06) m and 60.96 (7.67) kg, respectively and for the old males were 1.73 (0.09) m and 74.73 (11.83) kg and for the old females were 1.62 (0.04) m and 59.20 (7.01) kg, respectively.
We placed double differential surface electromyographic (EMG) electrodes and amplifiers (Trigno™ Wireless System, Delsys, Inc., Boston, MA, USA; electrode spacing of 10 mm) on the skin over the mid belly of selected arm muscles to measure non-dominant arm muscle activity. Each subject was asked to lightly exercise his/her arm and shoulder muscles by doing several push/pull ups and various stretches against a wall. We then measured subject’s resting and maximum voluntary pre-contraction (MVC) electromyographic (EMG) levels of the triceps brachii (long and lateral head), biceps brachii (short head), the anterior deltoid, pectoralis major and serratus anterior muscles during elbow and shoulder flexion, and extension and ab- and adduction by pulling up or pushing down on an handle attached to a vertical cable in series with an uniaxial force transducer (TLL-500, Transducer Techniques, Temecula, CA, USA) used for measuring maximum arm strengths. The several configurations for the elbow and shoulder muscle strength tests are described in the Appendix, Fig. A.
Next, each subject was asked to lie prone on a table with the left arm vertical and wrist positioned on a 6 axis force transducer (MC3A-1000, AMTI, Newton, MA, USA) mounted at one end of a 76 mm × 152 mm × 2,032 mm hollow aluminum beam having a rectangular cross-sectional shape and wall thickness 6.35 mm (Fig. 1). The beam was pivoted at its midpoint about a fulcrum formed from a pair of collinear needle bearings mounted on an axle in the horizontal plane. An Optotrak Certus camera (Northern Digital, Inc., Waterloo, Canada) was used to measure the displacements of 15 infrared-emitting optoelectronic markers (shown as dots in Fig. 1). A marker or marker triad were taped on the left side of the force transducer (markers #1–3), on the left aspect of the hand (#4), on the most caudal-lateral point on the radial styloid (#5), a triad on the left lateral aspect of the middle of the forearm segment (#6–8), at the most caudal point on lateral epicondyle (#9), a triad at the left lateral aspect of the mid upper arm segment (#10–12), at the center of rotation of the glenohumeral joint (#13), on the left lateral aspect of the base of the neck (#14), and over the T1 spinous process.

Schematic of testing apparatus for in vivo testing of the impulsively end loaded human upper extremity. Each subject lay on a padded table with left hand positioned on a force transducer (F). The subject was asked to concentrate on monitoring EMG biofeedback from his/her elbow extensor muscle activity provided on a display screen (S) and maintaining it at a certain level of muscular effort. A weight (W) of 23 kgf was then released by a remote trigger after a random delay to strike the end of the lever-arm (B) in order to apply an impulsive force to the wrist, thereby causing elbow flexion and shoulder adduction (the end of the lever-arm changing from B to B′). Alpha (α) and theta (θ) represent the initial shoulder extension and elbow flexion angles, respectively.
When ready, the subject was asked to hold the heel of his/her hand “lightly” in contact with the force transducer and to concentrate on monitoring EMG biofeedback from his/her lateral head of the triceps muscle on a display screen maintaining triceps activity either at rest, or 25, 50, and 75% MVC values from the main agonist muscle. A weight of 23 kgf was released (shown as “W” in Fig. 1) from a height of 720 mm to impact the top surface of the other end of the beam, thence applying an upward impulsive force to the wrist via the force transducer, thereby causing elbow flexion, shoulder extension/adduction and trunk extension. The subject was instructed “not to intervene” before, during and after the weight drop. For example, if the trial was conducted at 50% triceps MVC, the subject was instructed to contract the target muscle steadily at 50% of MVC during the test. Three trials at least were conducted at each of the three levels of muscle activation, and these were presented in randomized order.
The 3-D arm kinematics data were measured at 280 Hz. The kinematics and force data were digitally low-pass filtered (MATLAB, The MathWorks, 4th order Butterworth) with cutoff frequencies of 30 and 300 Hz. Surface electromyography (EMG) data were collected at 4 kHz. A band-pass 6th order filter with breakpoints at 40 and 500 Hz was used to attenuate any movement artefacts in the EMG signal. Then, the data were digitally low-pass 4th order Butterworth filtered with a cutoff frequency of 30 Hz. EMG data were normalized by maximum MVC values. The muscle preactivation state for each trial was determined as the mean EMG value over a 100 ms time window 50 ms before the weight drop.
Statistical Analyses
Descriptive statistics were undertaken for calculating joint marker kinematics, forces, and torques and EMG levels. A repeated measures analysis of variance (rm-ANOVA) was used to test the null hypothesis for age, gender, and three different muscle pre-contraction levels using SAS 9.3 software. A p value of less than 0.05 was considered statistically significant for the three main effects (primary hypothesis). A Bonferoni correction was used for the interactions.
Inverse Dynamics Optimization Model
An inverse dynamics optimization algorithm was used to estimate the rotational stiffness and damping at the elbow and shoulder joints using the measured impulsive moments, limb inertia (see next paragraph), and measured joint angles and wrist vertical displacement using MD Adams™ (MSC. Software Corporation, version 2010). A 3-D, sagittally-symmetric, four-link (including hand, forearm, upper arm and clavicle), lumped parameter, musculoskeletal representation was employed using equations of the form: \(\tau_{i} = K_{i} \theta_{i} + B_{i} \dot{\theta }_{i} + I_{i} \ddot{\theta }_{i}\), where \(\tau_{i}\) denotes the applied torque of each joint i, \(\theta_{i}\) is the angular displacement of each joint i, \(\dot{\theta }_{i}\) is the angular velocity of each joint i, \(\ddot{\theta }_{i}\) is the angular acceleration of each joint i, \(I_{i}\) is the calculated moment of inertia of each segment i, \(B_{i}\) is the rotational damping coefficient, and \(K_{i}\) is the rotational stiffness coefficient for each joint i. The moment of inertia was calculated by measuring the length of the limb and knowing the location of the center of mass of forearm and upper arm. The subject-specific anthropometric data are described in the next paragraph.
The model arm segments were assumed to be connected by four frictionless spherical joints at wrist, elbow, shoulder and sternoclavicular joints (Fig. 2). Segment anthropometric, mass, and inertial properties were scaled to each subject’s height and weight based upon the literature.34 The model arm muscles were represented by a bilinear torsional spring and linear damper placed in parallel at the elbow, and again at the shoulder and sternoclavicular joints. The bilinear behavior for each joint was characterized using two rotational stiffnesses (K 1 and K 2) and a single damping coefficient (B) in an optimization algorithm. Joint kinematics, including wrist angle, elbow angle, shoulder angle and wrist displacement, were measured as the arm was end loaded in a proximal direction in each impulsive loading trial. Next, an optimization routine that minimized the square of the paired differences between corresponding points on the desired and calculated (measured) joint torques was processed to find K 1, K 2 and B of each joint (Fig. 3). The Ks and B values were normalized by the product of subject body weight times height to reduce the effect of body size as a confounder in inter-subject comparisons; this also helps make the data more transferrable to other subjects.

In silico model for determining, via optimization, the lumped rotational stiffnesses (K 1 and K 2) and damping coefficients (B) for the elbow and shoulder (Left: sagittal plane, Right: transverse plane). The black dots denote spherical joints at wrist (extension), elbow (flexion), shoulder (extensor and adduction) and the sternoclavicular joint to ground.

Block diagram for describing the optimization algorithm showing the components of the muscle–joint model.
Results
Elbow and Shoulder Rotational Stiffness and Damping Coefficient Values
Sample flexion moment (torque) elbow and shoulder responses for an impulse load is shown using the broken lines in Fig. 4 (subject YMWK). The computer simulation optimized the values of K 1, K 2 and B at each joint, then the response of the model arm with these values was plotted (solid lines) in Fig. 4. The normalized mean values of elbow and shoulder rotational stiffness and damping values found for the 150 ms window after an impact are shown by gender, age and pre-contraction level in Table 1. Across all subjects, the mean (±SD) of the initial (K 1) and the second (K 2) stiffness were 0.843 (±0.605) N m rad−1 kg−1 m−1 and 0.860 (±0.321) N m rad−1 kg−1 m−1 for elbow, 1.105 (±0.663) N m rad−1 kg−1 m−1 and 0.135 (±0.126) N m rad−1 kg−1 m−1 for shoulder on transverse plane, and 9.904 (±2.795) N m rad−1 kg−1 m−1 and 0.788 (±0.422) N m rad−1 kg−1 m−1 for shoulder in the sagittal plane, respectively. For the damping, values of 0.037 (±0.032) N m s rad−1 kg−1 m−1 were found for the elbow, 0.012 (±0.013) N m s rad−1 kg−1 m−1 for the shoulder in the transverse plane, and 0.097 (±0.080) N m s rad−1 kg−1 m−1 for the shoulder in sagittal plane, respectively.

Time plot comparing the optimization results for the measured torque (broken lines from experimental data) and the computer predicted torque (solid lines from computer simulation result) at the elbow and shoulder joints. Data are from subject YMWK with pre-contraction level of 50% MVC.
Older adults had 57–95 and 76% of young adult stiffness and damping values, respectively; women had 51–80 and 66% of men’s stiffness and damping values at elbow, respectively (see Table 1 showing mean (SD) absolute values). We did not find significant age or gender differences in the normalized stiffness and damping values of the shoulder in either the sagittal or the transverse plane. However we found that the initial stiffness coefficient (K 1) of the shoulder in the sagittal plane in female adults was significantly higher than in male adults and this finding will be discussed further in next section.
In testing the primary hypothesis, main effects for age, gender, and pre-contraction level were found along with the interaction for each joint stiffness and damping value (Table 2, p < 0.05); the ANOVA demonstrated that pre-contraction level significantly affected normalized joint stiffness and damping coefficients. Age affected only the initial stiffness coefficient for the elbow (K 1) and gender affected both the initial stiffness (K 1) at the shoulder in sagittal plane and the damping coefficient (B) at the shoulder in the transverse plane. Stiffness and damping coefficients for the elbow and shoulder were proportional to higher levels of pre-contraction. However, women had a larger mean normalized stiffness value at the shoulder in both planes (Table 1).
Muscle Strength Results
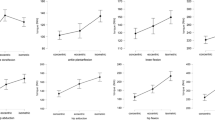
An ANOVA showing a significant effect of age and gender (p < 0.001) with men unsurprisingly being found stronger than women and young adults stronger than older adults in all six tests (Fig. 5, Table 3 and “Appendix” section). Arm muscle strength explained 30% of the variance in the normalized K 1 and 17% of the variance in K 2 at the elbow (Fig. 6). However strength did not explain a significant proportion of the variance in shoulder stiffnesses.

Scatter plot of the shoulder muscle strengths plotted against body size (height times weight) for all subjects. This plot shows the strength of the elbow flexor muscles measured in the straight arm pull up test (Appendix, Fig. A). The other muscle strengths showed similar results.

Scatter plot of the calculated elbow normalized bilinear stiffnesses at 75% MVC for all subjects. (Upper: K 1, Bottom: K 2).
Discussion
We used a novel drop weight testing apparatus to safely measure the lumped rotational stiffness and damping at the elbow and shoulder joints in non-dominant arms placed under impulsive end-loads. This is the first experimental evidence for the effect of age, gender and muscle pre-contraction level on the rotational stiffness and damping resistance of the elbow and shoulder joints. The main hypotheses were rejected in that the ANOVA (Table 2) demonstrated a significant effect of pre-contraction level on lumped upper extremity viscoelastic properties; some age and gender effects were also found. Although two significant interactions were found (for example, age × gender and age × gender × pre-contraction in Table 2) they do not profoundly affect the main conclusions.
In the current study we assumed that the rotational stiffness of the muscles acting about each joint had bilinear properties15,27 in that the initial stiffness (K 1) would typically be higher than the later stiffness (K 2) under a large deflexion, although some older adult elbow K 1 and K 2 values did not follow this tendency. If the mean of the elbow K 1 and K 2 values was calculated then the absolute values of the stiffness were 76.7 N m rad−1 for young females and 159.9 N m rad−1 for young males (Table 4). The range of non-normalized elbow stiffness and damping coefficients were consistent with a previous elbow study in healthy young adults.22
The gender and age differences found in the absolute mean values at the elbow in Table 4 were consistent with the normalized results: the older females had the lowest values, next came the young females, the older males had the third highest and the young males had the highest values (Fig. 6). These results correspond to known age- and gender-associated declines in muscle strength and power measurements in the upper extremities in women and men.10,14,28 Such findings could partially explain why older women more commonly fail to safely arrest a fall using their arms because of their loss in muscle strength and consequent reduction in viscoelastic resistance to stretch in the upper extremity protraction muscles.7,22
Although the elderly women had lower stiffness and damping coefficient values and strength than the young adults or men in the elbow muscles, there is little known about the viscoelastic properties of active shoulder muscles when the arm is subjected to impulsive end-loading. This is why we developed the present apparatus to measure the values of the rotational stiffness and damping parameters at the elbow and shoulder muscles, while subjects actively resisted an impulsive type of loading that is familiar to anyone who has used their hand to protect themselves from the ground while arresting a fall.
We found that 9.9 N m rad−1 kg−1 m−1 of the normalized stiffness mean value (K 1) and 0.097 N m rad−1 kg−1 m−1 of the normalized damping mean value (B) of the shoulder in sagittal plane (see Table 1) were an order of magnitude greater than the stiffness and 2.6 times greater than the damping measured at the elbow or the shoulder in the transverse plane. This result implies that the viscoelastic properties in resisting extension at the shoulder may be as important a factor for arresting a fall as the ad-/abduction muscles of the shoulder joint.
It was surprising that the secondary hypothesis was not supported: arm strength was not significantly correlated with normalized elbow or shoulder stiffnesses. Similarly, we did not find a significant effect of gender on the shoulder stiffnesses in the present study (K 1 and K 2, Table 2). It is well known that muscle strength decreases with advancing age, particularly in women.28 While we found age and gender differences in strength on elbow and shoulder muscles (Fig. 5), the values for maximum voluntary elbow and shoulder torques found in the literature (Table 5) do not appear to show a relationship between the mean values of flexion and extension torque within the same gender, especially at the shoulder. This may help explain why we could not find a marked relationship between the stiffness values and the maximum voluntary strength at the shoulder.
Our experimental and computational methods have several limitations. The first limitation was the relatively modest impulsive force generated by the apparatus we used: approximately 25% of body weight, which is markedly lower than the full body-weight force measured in young subjects in actual falls by DeGoede et al. 5 However, we limited the magnitude of the impulsive force to be certain that we did not injure any of the older subjects’ wrists, elbow extensor or shoulder muscles via a muscle lengthening contraction injury.1 The impulsive force induced torques of up to ~25 N m at the elbow and ~50 N m at the shoulder (Fig. 4) which are also less than those induced in a real fall.7 In addition, we did not notify subjects of the exact time of release of weight to lessen the risk that they would abruptly decide to change the desired level of precontraction just prior to impact. Nonetheless, many subjects commented that the nature of the loading felt similar to that during a real fall arrest.
A second limitation was the simplifying assumption that the proximal end of the clavicle could only rotate, but not translate, in space. Hence we may have overestimated the actual rotation at this particular joint. A third limitation was that we used only the triceps lateral brachii EMG activity to indicate the muscle pre-contraction level via biofeedback. Originally we provided feedback on both triceps and deltoid activities, but it proved too much for some subjects to maintain constant preactivation levels on both, so we elected to use one representative arm protraction muscle for biofeedback.
A fourth limitation is that stiffness and damping values may be underestimated compared to other studies11,13,29 because the present study was limited to the non-dominant side. Although sagittally-symmetric falls do occur,23 many forward fall arrests are actually asymmetrical,32 so we chose to study the non-dominant arm response as the ‘worst case’ scenario for a fall.
A fifth limitation is that the rotational stiffness and damping parameters at the elbow were considered independent of those acting about the shoulder. We limited our model to analyzing the situation in which an individual lands on the ‘heel’ of his/her hand such that little or no moment from the ground reaction force is transmitted across the wrist joint: therefore the forearm muscles played little or no role in the response of the wrist. However, anatomically portions of both biceps and triceps act across both joints so there may be some degree of co-dependency between the elbow and shoulder muscles’ resistance to arm joint rotation that was not parsed out here. This behavior might be useful to consider in future studies.
Despite these limitations, we conclude that age, gender and especially pre-contraction level do affect the rotational properties of the elbow and shoulder under impulsive arm end-loading, and these factors may therefore be anticipated to affect the buckling behavior of an upper extremity under such loading.
Notes
(Protocol #HUM00052983).
References
Brooks, S. V., E. Zerba, and J. A. F. Faulkner. Injury to muscle fibres after single stretches of passive and maximally stimulated muscles in mice. J. Physiol. 488:459–469, 1995.
Brown, I. E., and G. E. Loeb. Measured and modeled properties of mammalian skeletal muscle: IV. Dynamics of activation and deactivation. J. Muscle Res. Cell Motil. 21:33–47, 2000.
Case, L., J. Lo, and J. A. Ashton-Miller. Arrest of Forward Falls Onto Outstretched Hands in Healthy Young Women. Cleveland, OH: International Society of Biomechanics Congress, 2005.
Chaffin, D. B., G. B. J. Andersson, and B. J. Martin. Occupational Ergonomics. New Jersey: Wiley, 2006.
DeGoede, K. M., and J. A. Ashton-Miller. Fall arrest strategy affects peak hand impact force in a forward fall. J. Biomech. 35:843–848, 2002.
DeGoede, K. M., and J. A. Ashton-Miller. Biomechanical simulations of forward fall arrests: effects of upper extremity arrest strategy, gender and aging-related declines in muscle strength. J. Biomech. 36:413–420, 2003.
DeGoede, K. M., J. A. Ashton-Miller, and A. B. Schultz. Fall-related upper body injuries in the older adult: a review of the biomechanical issues. J. Biomech. 36:1043–1053, 2003.
DeGoede, K. M., J. A. Ashton-Miller, A. B. Schultz, and N. B. Alexander. Biomechanical factors affecting the peak hand reaction force during the bimanual arrest of a moving mass. J. Biomech. Eng. 124:107–112, 2002.
Dietz, V., J. Noth, and D. Schmidtbleicher. Interaction between pre-activity and stretch reflex in human triceps brachii during landing from forward falls. J. Physiol. (Lond.) 311:113–125, 1981.
Faulkner, J. A., L. M. Larkin, D. R. Claflin, and S. V. Brooks. Age-related changes in the structure and function of skeletal muscles. Clin. Exp. Pharm. Physiol. 34:1091–1096, 2007.
Frolov, A. A., R. Prokopenko, M. Dufosse, and F. B. Ouezdou. Adjustment of the human arm viscoelastic properties to the direction of reaching. Biol. Cybern. 94:97–109, 2006.
Frykman, G. Fracture of the distal radius including sequelae-shoulder-hand-finger syndrome, disturbance in the distal radio-ulnar joint and impairment of nerve function: a clinical and experimental study. Acta Orthop. Scand. 108(Suppl):14–26, 1967.
Gomi, H., and R. Osu. Task-dependent viscoelasticity of human multijoint arm and its spatial characteristics for interaction with environments. J. Neurosci. 18:8965–8978, 1998.
Goodpaster, B. H., S. W. Park, T. B. Harris, S. B. Kritchevsky, M. Nevitt, A. V. Schwartz, E. M. Simonsick, F. A. Tylavsky, M. Visser, and A. B. Newman. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J. Gerontol. A 61:1059–1064, 2006.
Grover, J. P., D. T. Corr, H. Toumi, D. M. Manthei, A. L. Oza, R. Vanderby, Jr, and T. M. Best. The effect of stretch rate and activation state on skeletal muscle force in the anatomical range. Clin. Biomech. 22:360–368, 2007.
Hagberg, M., B. Silverstein, R. Wells, M. J. Smith, H. W. Hendrick, P. Carayon, and M. Pérusse. Work Related Musculoskeletal Disorders (WMSDs): A Reference Book for Prevention. London: Taylor & Francis, 1995.
Hsiao, E., and S. Robinovitch. Common protective movements govern unexpected falls from standing height. J. Biomech. 31:1–9, 1998.
Hughes, V. A., W. R. Frontera, M. Wood, W. J. Evans, G. E. Dallal, R. Roubenoff, and M. A. F. Singh. Longitudinal muscle strength changes in older adults influence of muscle mass, physical activity, and health. J. Geront. A 56:B209–B217, 2001.
Hughes, R. E., M. E. Johnson, S. W. O’Driscoll, and K. An. Age-related changes in normal isometric shoulder strength. Am. J. Sports Med. 27:651–657, 1999.
Ingebrigtsen, T., K. Mortensen, and B. Romner. The epidemiology of hospital-referred head injury in northern Norway. Neuroepidemiology 17:139–146, 1998.
Kannus, P., M. Palvanen, and S. Niemi. Time trends in severe head injuries among elderly Finns. JAMA 286:673–674, 2001.
Lee, Y., and J. A. Ashton-Miller. The effects of gender, level of co-contraction, and initial angle on elbow extensor muscle stiffness and damping under a step increase in elbow flexion moment. Ann. Biomed. Eng. 39:2542–2549, 2011.
Lee, Y., and J. A. Ashton-Miller. Model-predicted buckling of the adult human upper extremity: effects of peak impulsive force and muscle states. Omaha, NE: American Society of Biomechanics, 2013.
Lee, Y., and J. A. Ashton-Miller. Age and gender effects on the proximal propagation of an impulsive force along the human upper extremity. Ann. Biomed. Eng. 42:25–35, 2014.
Lo, J., and J. A. Ashton-Miller. Effect of upper and lower extremity control strategies on predicted injury risk during simulated forward falls: a study in healthy young adults. J. Biomech. Eng. 130:041015, 2008.
Lo, J., G. McCabe, K. DeGoede, H. Okuizumi, and J. Ashton-Miller. On reducing hand impact force in forward falls: results of a brief intervention in young males. Clin. Biomech. 18:730–736, 2003.
Malamud, J. G., R. E. Godt, and T. R. Nichols. Relationship between short-range stiffness and yielding in type-identified, chemically skinned muscle fibers from the cat triceps surae muscles. J. Neurophysiol. 76:2280–2289, 1996.
Metter, E. J., R. Conwit, J. Tobin, and J. L. Fozard. Age-associated loss of power and strength in the upper extremities in women and men. J. Gerontol. Biol. Sci. Med. Sci. 52A:B267–B276, 1997.
Osu, R., D. W. Franklin, H. Kato, H. Gomi, K. Domen, T. Yoshioka, and M. Kawato. Short-and long-term changes in joint co-contraction associated with motor learning as revealed from surface EMG. J. Neurophysiol. 88:991–1004, 2002.
Sattin, R. W., D. A. Lambert-Huber, C. A. DeVito, J. G. Rodriguez, A. Ros, S. Bacchelli, J. A. Stevens, and R. J. Waxweiler. The incidence of fall injury events among the elderly in a defined population. Am. J. Epidemiol. 131:1028–1037, 1990.
Stobbe, T. J. The development of a practical strength testing program for industry. Ph.D. Dissertation, University of Michigan, Ann Arbor, MI. 1982.
Troy, K. L., and M. D. Grabiner. Asymmetrical ground impact of the hands after a trip-induced fall: experimental kinematics and kinetics. Clin. Biomech. 22:1088–1095, 2007.
Vellas, B. J., S. J. Wayne, P. J. Garry, and R. N. Baumgartner. A two-year longitudinal study of falls in 482 community-dwelling elderly adults. J. Gerontol. Biol. Sci. Med. Sci. 53A:M264–M274, 1998.
Winter, D. A. Biomechanics and motor control of human movement. New Jersey: Wiley, pp. 59–85, 2005.
Acknowledgments
We thank the subjects for their participation and the financial support of PHS Grant P30 AG 024824 is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Amit Gefen oversaw the review of this article.
Appendix

Rights and permissions
About this article

Cite this article
Lee, Y., Ashton-Miller, J.A. Effects of Age, Gender and Level of Co-contraction on Elbow and Shoulder Rotational Stiffness and Damping in the Impulsively End-Loaded Upper Extremity. Ann Biomed Eng 43, 1112–1122 (2015). https://doi.org/10.1007/s10439-014-1185-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-014-1185-3