
Abstract
Background
The aim of this study was to develop surgical methods for the implantation of a wireless intraocular epiretinal retina implant (EPI RET3) in Göttingen minipigs. This animal model resembles closely the anatomical conditions in humans, and is thus suitable for investigating the EPI RET3 implant as designed for the application in humans.
Methods
Phacoemulsification and vitrectomy was performed on the right eye of 16 Göttingen minipigs under general anesthesia. The implants, consisting of a receiver module and an electrode array connected via a flexible micro cable, were inserted through a corneoscleral incision. The receiver module was placed into the sulcus ciliaris and the electrode array was fixed onto the retina temporal to the optic disc with a retinal tack. Minipigs were monitored for intra- and postoperative ocular complications. Follow-up times were 3 (seven minipigs) and 12 weeks (nine minipigs).
Results
Implantation was successfully performed in all 16 minipigs. The complete implantation surgery required on average 2 hours. Intraoperative findings were a minor hemorrhage of the anterior chamber angle in two eyes, one minor iris hemorrhage, and one minor punctiform retinal hemorrhage, which were all reversible. Postoperatively, the corneoscleral incision showed good wound healing in all eyes. Intraocular reactions included mainly fibrin exudation (six eyes) and formation of iris synechiae with the receiver module of the implants (three eyes).
Conclusions
The performed implantation procedures of the intraocular EPI RET3 implant are feasible and reproducible within an acceptable surgical time. The development of inflammatory responses is a specific predisposition of the minipig following any intraocular intervention; nevertheless, the surgical techniques should be further improved to minimize procedure-related reactions. Our results provide a step towards the application of the EPI RET3 system in clinical studies.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Retinitis pigmentosa (RP) is a hereditary progressive retinal dystrophy of the photoreceptors or the retinal pigment epithelium that may lead in advanced stages to irreversible loss of vision. To date, more than 50 genes and loci are known to be involved in the pathogenesis of RP, and it is assumed that many more RP genes will be found in the future [1, 2]. Worldwide, about 2 million people are suffering from RP [3], in Germany 30,000 to 40,000 patients are affected with this currently untreatable disease. The worldwide prevalence is about one in 4,000 individuals [4].
A large percentage of the inner retinal neurons remains histologically intact [5], and electrical stimulation of the retina can be used to elicit phosphenes in blind individuals suffering from RP [6–8]. In order to restore vision in RP patients, different approaches to the development of electronic visual retinal prostheses are currently being investigated, which comprise epiretinal [6, 9–13], subretinal [14–16], transchoroidal [17], and episcleral [18] systems.
While most current retinal implant concepts require a cable connection to extraocular electronic components passing the eye’s wall [11, 19, 20], the EPI RET3 retina implant system is implanted entirely within the eye, and is wirelessly provided with data and energy via an external transmitter unit [21–23].
In the present study, the development of the optimal surgical implantation techniques of the intraocular EPI RET3 retina implant are described in Göttingen minipigs. This animal model has been proved to be suitable for the research on visual prostheses in numerous previous studies, as the anatomy and surgical conditions exhibit close similarity with the human eye [20, 24–28].
Material and methods
The present study was performed in minipigs (Göttingen minipig, Ellegaard, Denmark). All animals were treated according to the “Principles of Laboratory Animal Care” (NIH publication No. 85–23, revised 1985), and the OPRR Public Health Service Policy on the Humane Care and Use of Laboratory Animals (revised 1986). The German Law on the Protection of Animals (published 2006) was followed, and the study was approved by the Düsseldorf district government (North Rhine Westphalia, Germany).
Implantation of the EPI RET3 retina implant system and postoperative treatment
Sixteen Göttingen minipigs were premedicated by intramuscular injection of atropine sulfate (0.05 mg/kg body weight (BW); Atropinsulfat B. Braun 0.5 mg/ml; B. Braun Melsungen AG, Melsungen, Germany), azaperone (2 mg/kg BW; Stresnil; Janssen-Cilag GmbH, Neuss, Germany), and ketamine (30 mg/kg BW; Ketamin 10%; Ceva Tiergesundheit GmbH, Düsseldorf, Germany). Subsequently, anesthesia was maintained using sevoflurane (Sevorane; Abbott GmbH & Co. KG, Wiesbaden, Germany) via orotracheal intubation. Animals were artificially ventilated, and body temperature, blood oxygen, and ECG were monitored. Only the right eye was treated in each individual, with positioning of the animals on their left side. The operation field was rinsed with povidone–iodine solution (Betaisodona; Mundipharma GmbH, Limburg, Germany). Through a corneoscleral incision of 3-mm width, a capsulorhexis was created under viscoelastic material. The lens and capsule were hydrodissected, and phacoemulsification was performed. The corneoscleral incision was temporarily sutured. Following complete three-port pars plana vitrectomy using an indirect ophthalmomicroscope (BIOM; Oculus Optikgeräte GmbH, Wetzlar, Germany), the posterior capsule was opened using a lance and the opening was enlarged with the vitrectome. After maintaining the anterior segment with hyaluronic acid, the corneoscleral incision was extended to 11-mm width to allow insertion of the EPI RET3 implant (Fig. 1). For implantation, the electrode array was bent towards the receiver module (Fig. 2a), and both parts of the implant were held with anatomical forceps (Fig. 2b). In this position, the implant length was halved. The implant was inserted with the micro cable first using angled anatomical forceps (Fig. 3a,b). Then the receiver module and the electrode array were inserted through the corneoscleral incision (Fig. 3c,d). The electrode array was inserted through the anterior and posterior capsulorhexis into the vitreous cavity, and the receiver module was placed into the sulcus ciliaris (Fig. 3e,f). The corneoscleral incision was closed with absorbable suture material to avoid later removal of sutures requiring general anesthesia. After the anterior segment-tightness was ascertained, surgery proceeded at the retinal site using the indirect ophthalmomicroscope (BIOM). The electrode array was placed temporal to the papilla and fixed with one titanium retinal tack (Geuder, Heidelberg, Germany; Fig. 3g,h) to prevent possible micro movements of the array caused by eye movements in the awake animal. Afterwards, acetylcholine chloride intraocular solution (Miochol E; Novartis GmbH, Nürnberg, Germany) was given to induce pupil constriction, thus providing a stable position of the receiver module behind the iris in the sulcus ciliaris (Fig. 4a,b). Prior to suturing the conjunctiva, the area was rinsed again with povidone–iodine solution to reduce the risk of postoperative inflammation. Postoperatively, the animals were treated with antibiotic- and cortisone-containing eye ointment (Dexamytrex; gentamicin sulfate 5 mg/g, dexamethasone 0.3 mg/g, Dr. Mann Pharma, Berlin, Germany) twice daily for 14 days. Additionally, analgesic medicaments were given (Carprofen 4 mg/kg SID PO for 3 days, Rimadyl chewable tablets; Pfizer GmbH, Berlin, Germany).

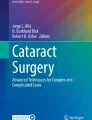
EPI RET3 retina implant as used in the present study. Left, the IOL-type receiver unit encapsulated with silicone, including the receiver coil, receiver chip and stimulation chip. This part is placed into the sulcus ciliaris. The right portion depicts the electrode array with 25 IrOx stimulation electrodes, which will be fixed epiretinally with a retinal tack in the oval fixation lug (blue arrow). Inset: SEM micrograph of one 3D-stimulation electrode. Electrode diameter = 100 μm. Source: IWE1, RWTH Aachen Germany

Handling of the EPI RET3 device: Preparation for implantation. The electrode array is taken at the terminal fixation lug (a) and bent towards the receiver module; both parts of the implant are safely held with anatomical forceps (b), (above b in schematic side view). af, anatomical forceps; ea, electrode array; mc, micro cable; rm, receiver module

Implantation procedure of the EPI RET3 retina implant. a, c, e, g Schematic diagrams of the implantation steps, cross-sectional view. b, d, f, h Photographs of the corresponding surgical steps in one minipig. a Insertion of the implant with the micro cable first using angled anatomical forceps. b Corresponding to a. c Insertion of the receiver module and electrode array through the corneoscleral incision. d Corresponding to c. e Insertion of the electrode array through the anterior and posterior capsulorhexis into the vitreous cavity and placement of the receiver module into the sulcus ciliaris. f Corresponding to e. g Implant in situ with retinal tack fixation of the electrode array. h Corresponding to g. Funduscopic view showing the retinal tack, the electrode array, and the terminal fixation lug (from left to right)

Stabilization of the receiver module of the EPI RET3 device in posterior chamber position. a Injection of acetylcholine chloride intraocular solution with dilated pupil, the receiver coil is visible in the posterior chamber (asterisk). b Pupil constriction, receiver module completely behind the iris and centered
Altogether, 16 sterile EPI RET3 systems were implanted. Animals were observed for a period of 3 weeks (seven minipigs) or 12 weeks postoperatively (nine minipigs) respectively, and then sacrificed.
Concept and technical specifications of the EPI RET3 system
The EPI RET3 system comprises an extraocular and an intraocular component (Fig. 5). The extraocular part includes a computer system, a transmitter unit, and a transmitter coil integrated into a holder positioned in front of the eye. The intraocular implant is composed of a receiver module and an array of stimulation electrodes; both parts are connected via a flexible micro cable (Figs. 1 and 5). The receiver unit includes a receiver coil, a receiver microchip, and a stimulation chip (Figs. 1 and 5). Computer generated stimulation data and control signals are wirelessly transmitted to the intraocular receiver coil from where they are passed to the receiver microchip (Fig. 5). The stimulation chip generates stimulation pulses, which are forwarded via the micro cable to the epiretinally fixed electrode array where selected electrodes are activated [29]. All electronic components of the intraocular part of the EPI RET3 retina implant are mounted on a flexible polyimide foil of 40-mm length and 10-μm thickness. The planar receiver coil, the metal wiring and the electrodes are formed by microelectroplating of gold. The hexagonal electrode array contains 25 3D IrOx electrodes (Fig. 1, inset), each with a diameter of 100 μm and 25 μm height and a center-to-center distance of 500 μm [30, 31]. The electrodes are covered with a thin film of iridium oxide [32]. The entire implant is coated with parylene C, and the active surface of the stimulation electrodes is exposed by plasma etching. The receiver coil, receiver microchip and stimulation chip are integrated in an intraocular lens (IOL) structure which is, together with a short part of the outgoing micro cable, finally encapsulated with a two-component silicone material used for intraocular lens fabrication. The IOL structure of the receiver module has a diameter of 10.5 mm and is designed with a central hole of 3.5 mm diameter to enable posterior insight (Fig. 1). The encapsulated implant is sterilized by ethylene oxide [33]. The EPI RET3 retina implant used in the present study has been evaluated according to DIN EN ISO 10993 standards, and meets the requirements for an application as medical device in clinical studies.

Principle of the EPI RET3 system. Data and energy are wirelessly transmitted from a transmitter coil to the receiver module of the implant, positioned in the posterior chamber. Signals are transmitted via a flexible micro cable to an array of 25 3D stimulation electrodes. Stable epiretinal position of the stimulator is ensured by retinal tack fixation ([44], modified)
Results
The implantation of the EPI RET3 systems was successfully performed in all 16 minipigs without major complications. Due to the narrow palpebral fissure in the minipig, a different surgical position from the superior one in humans is required. Surgery performed from the nasal part of the eye proved to be the optimal one.
In the beginning of the implantation series the receiver module could not be placed completely behind the iris in five animals, and subsequently an iris capture occurred in three minipigs. In the surgeries which followed, this problem was avoided by a maximal pupil dilatation prior to surgery (Fig. 4a) — and application of acetylcholine chloride intraocular solution after insertion of the receiver module into the sulcus ciliaris. Pupil constriction was obtained shortly after injection, with the result that the receiver module remained in a stable and well-centered position behind the iris in the sulcus ciliaris (Fig. 4b).
Together with the use of an indirect ophthalmomicroscope (BIOM) the central hole of 3.5 mm diameter in the receiver module (Fig. 1) provided a sufficient viewing angle for bimanual handling, positioning, and fixation of the electrode array onto the retinal surface with a retinal tack.
Although the implant design allowed fixation of the electrode array at two sides of the array in various positions (Fig. 1), fixation with one retinal tack in the oval lug (Fig. 1, blue arrow) was sufficient to obtain a stable and attached position of the electrode array onto the retina, as confirmed by funduscopy (Fig. 3h). The implant design was optimal with regard to the length of the flexible connecting cable between the receiver module and the electrode array: In all eyes, the micro cable remained in stable position following the retinal curvature after fixation of the electrode array. In none of the surgeries did retinal detachment occur, thus silicone oil was not required. The duration of the complete implantation surgery was on average 2 hours. All minipigs showed good recovery from the general anesthesia.
Implantation of the receiver module required a large corneoscleral incision, resulting in an intraocular hypotension for the approximately 1.5 minutes of the insertion time. During this time, a reversible hemorrhage of the chamber angle occurred in two eyes. In one eye the receiver module slightly scraped the iris, causing a minor reversible iris hemorrhage. In one case, a minor reversible punctiform hemorrhage of the retina was noted.
In the postoperative follow-up, the corneoscleral incision showed good wound healing without any complications. The corneal surface was clear and smooth. In four eyes, a slight corneal haze restricted to the area of the incision was observed, developing within 1 to 10 weeks postoperatively (Fig. 6a). Three to 4 weeks postoperatively, two eyes showed corneal vascularisations starting at the incision area (Fig. 6b). Intraocular reactions included fibrin exudations commencing in the first postoperative week (six eyes). One to 3 weeks postoperatively, formation of iris synechiae at the central part of the receiver module was noted (three eyes, Fig. 6a,b). One eye showed an iris hyperemia 10 weeks after surgery. The intraocular reactions were treated with antibiotic and cortisone eye ointment (gentamicin sulfate 5 mg/g, dexamethasone 0.3 mg/g).

Postoperative follow-up. a One week postoperatively, minimal corneal haze developed at the area of the incision (black arrow); the corneal surface is otherwise clear and smooth. The pupil is in normal transverse-oval shape. The receiver coil is visible behind the iris; some synechiae developed between the iris and the central part of receiver module (white arrow). b Another minipig 3 weeks postoperative, showing vascularisations starting from the incision (black arrow) and some iris synechiae with the central part of receiver module (white arrow)
Discussion
Currently developed retinal implants aim to partially restore vision in blind RP patients by electrical stimulation of intact inner retinal neurons. One concept of bypassing the damaged retinal tissue is an epiretinal placement of an electrode array in the area of the posterior pole, and direct stimulation of ganglia using signals from an external camera and power sent from an external transmitter. The resulting specific activation of the visual cortex has been demonstrated in experimental animal models [24, 25, 34, 35] as well as in blind subjects by recording of visual perceptions [12, 13, 29].
The present study describes surgical techniques for implantation of an advanced epiretinal wireless retina implant in Göttingen minipigs. The minipig eye is a suitable model for the research on visual prostheses based on the close similarity of anatomical features and surgical conditions with the human eye [24, 27, 28]. The EPI RET3 retina implant used in our study is unique, as it is designed as a completely intraocular device that is wirelessly provided with data and energy via an external transmitter unit [21–23]. To our knowledge, all other currently developed epiretinal and subretinal implants require a cable connection from the intraocular stimulator to external components that may be placed episclerally [19] or subcutaneously behind the ear [11, 20]. The advantages of an entirely intraocular visual prosthesis in comparison to systems that require an external cable connection are a reduced risk of infections, a shorter surgery, and the absence of long-term mechanical stress. Moreover, a wireless data and energy transmission to the implant allows totally unrestricted eye movements, and is therefore suitable for the long-term use in amaurotic patients.
Our method of complete intraocular implantation of the current EPI RET3 implant requires a complex surgical procedure including lens removal, vitrectomy, and an extension of the corneoscleral incision to 11 mm prior to inserting the device. While lens extraction and vitrectomy are standard ophthalmic surgical procedures, the large corneoscleral incision requires careful handling. Intraoperative maintenance of intraocular pressure and the tight closure of the incision following surgery are important features that must be met. Considering the complex implantation procedure, only few minor intraoperative problems occurred. The observed chamber angle hemorrhages in two eyes were due to ocular hypotension following the enlargement of the corneoscleral incision, and were reversible without consequences. From the total surgical time of about 2 hours, the corneoscleral opening existed for less than 2 minutes, and after insertion of the implant an immediate first adapting suture was placed to balance the intraocular pressure. A similar risk of hemorrhage is found for example in penetrating keratoplasty [36, 37], where a comparable period of hypotonia occurs during the open sky wound prior to placement of the transplant. In addition, intracapsular cataract extraction was generally performed using a 10-mm incision [38] before the technique of phacoemulsification through small-sized corneal or corneoscleral incisions was introduced [39]. Nevertheless, a future EPI RET implant should be designed with a smaller receiver module, to minimize the corneal incision size. Considering the rapidly developing miniaturization of electronic systems and the continuous progress in biomaterial research, we assess the realization of this improvement as feasible. One possible approach is the development of a slightly thinner and more flexible receiver module that could be folded once, reducing its diameter to approximately 6 mm. Intraoperatively, a safe handling and insertion of the implant as illustrated in Figs. 2 and 3 were possible using anatomical forceps that made it possible to hold the implant reliably without causing any damage to it, as they lack sharp edges.
The retinal tack fixation of the electrode array was controlled by binocular funduscopy, and showed optimal attachment of the array to the retinal surface. This is a prerequisite for successful neuronal stimulation with minimal thresholds [21, 22, 40]. The uncomplicated use of retinal tacks has already been shown in previous animal experiments [41–43]. The design of the implant used in the present study allows tack fixation at four different positions thus facilitating optimal positioning of the electrode array onto the retina without any tension when only two tacks are used. In addition, the device is designed for easy explantation due to the open loop arrangement of three of the tack positions. Implants that are fixed using the oval lug may also be easily detached from the retina by opening the lug with micro scissors. Uncomplicated and safe tack fixation of stimulator modules has been shown for the EPI RET3 retina implant in a clinical study on six patients with blindness and RP [44], and has also been used successfully in other epiretinal prosthesis projects [45, 46]. As the tack fixation nevertheless perforates the retinal tissue, alternative methods of electrode array fixation should be investigated in future studies. A promising approach may be the use of bioadhesive materials. Recently developed tissue adhesives provided short-term nontoxic, noninflammatory retinal adhesion in vivo [47]. However, for a long-term application as in retinal implants, their performance needs yet to be tested.
The total implantation surgery required on average 2 hours. We assess this surgical time as acceptable, considering the complexity of the surgery. The implantation time of a subretinal visual prosthesis with external connections was significantly longer lasting 6 to 7 hours in a human study [48]. A long surgical duration, requiring an extended time of anesthesia, is not only undesirable for the patient, but may also be a critical factor in animal experiments. This is particularly the case for the pig model, where severe arrhythmias may occur and sensitivity to malignant hyperthermia during general anesthesia has been shown [49, 50]. Gekeler et al. [20] reported that three pigs of a total of 11 animals died during recovery from general anesthesia following a 5- to 9-hour implantation procedure of subretinal prostheses.
Postoperatively, the uncomplicated healing of the corneoscleral incision was a positive result found in all animals. The observed slight corneal haze at the incision area is caused by an inflammatory reaction to the absorbable suture material used herein. In using absorbable sutures, we avoided a further general anesthesia in the minipigs. Non-resorbable sutures are applied in humans with easy removal using topical anesthetics. The described postoperative fibrin exudations and formation of synechiae reflect to a certain extent a species-specific predisposition to develop inflammatory reactions following any intraocular intervention [28], as observed in other studies as well [20]. But apart from these species-related characteristics, the surgical procedure itself may also induce inflammatory reactions. Four of six RP patients of the clinical EPI RET3 study also showed inflammatory responses after receiving the retina implant, but these were considerably less pronounced and transient [44]. Long-term studies in the minipig model are required to further optimize the implantation procedure and to reduce the risk for postoperative inflammation. As the EPI RET3 implant used in the present study meets the requirements for an application as medical device in clinical studies (biocompatibility approved according to DIN EN ISO 10993 standards), the observed inflammatory reactions are unlikely to be caused by incompatibility to the implant materials. Another feature that is characteristic for the minipig iris is an increased vascularisation in comparison to the human iris [27], which explains the comparatively higher risk of intraoperative iris hemorrhage, as well as the postoperative development of iris hyperemia. The results of the EPI RET3 clinical study support these assessments: During the 4 weeks of follow-up, an iris hyperemia or iris hemorrhage did not occur [44].
With regard to the possible benefit for blind RP patients to achieve to a certain extent an artificial visual function with the EPI RET3 device, the described intra- and postoperative findings are acceptable. In addition to the topics investigated in the present study, retinal stimulation experiments with the EPI RET3 implant and a histological evaluation of tissue responses to implantation and stimulation are of interest, and will be addressed in separate publications.
In conclusion, the present study shows that the performed surgical implantation procedures are feasible and reproducible. The advantages of the EPI RET3 retina implant are its complete implantability into the eye, combined with a wireless energy and data transmission via inductive coupling.
References
Daiger SP, Bowne SJ, Sullivan LS (2007) Perspective on genes and mutations causing retinitis pigmentosa. Arch Ophthalmol 125:151–158
Aldahmesh MA, Safieh LA, Alkuraya H, Al-Rajhi A, Shamseldin H, Hashem M, Alzahrani F, Khan AO, Alqahtani F, Rahbeeni Z, Alowain M, Khalak H, Al-Hazzaa S, Meyer BF, Alkuraya FS (2009) Molecular characterization of retinitis pigmentosa in Saudi Arabia. Mol Vis 15:2464–2469
Margolis DJ, Detwiler PB (2011) Cellular origin of spontaneous ganglion cell spike activity in animal models of retinitis pigmentosa. J Ophthalmol. doi:10.1155/2011/507037
Hartong DT, Berson EL, Dryja TP (2006) Retinitis pigmentosa. Lancet 368:1795–1809
Santos A, Humayun MS, de Juan E Jr, Greenburg RJ, Marsh MJ, Klock IB, Milam AH (1997) Preservation of the inner retina in retinitis pigmentosa. A morphometric analysis. Arch Ophthalmol 115:511–515
Rizzo JF, Wyatt J, Loewenstein J, Kelly S, Shire D (2003) Methods and perceptual thresholds for short term electrical stimulation of human retina with microelectrode arrays. Invest Ophthalmol Vis Sci 44:5355–5361
Fujikado T, Morimoto T, Kanda H, Kusaka S, Nakauchi K, Ozawa M, Matsushita K, Sakaguchi H, Ikuno Y, Kamei M, Tano Y (2007) Evaluation of phosphenes elicited by extraocular stimulation in normals and by suprachoroidal–transretinal stimulation in patients with retinitis pigmentosa. Graefes Arch Clin Exp Ophthalmol 245:1411–1419
Nanduri D, Humayun MS, Greenberg RJ, McMahon MJ, Weiland JD (2008) Retinal prosthesis phosphene shape analysis. Conf Proc IEEE Eng Med Biol Soc 2008:1785–1788
Walter P, Mokwa W (2005) Epiretinal visual prosthesis. Ophthalmologe 102:933–940
Güven D, Weiland JD, Fujii G, Mech BV, Mahadevappa M, Greenberg R, Roizenblatt R, Qiu G, Labree L, Wang X, Hinton D, Humayun MS (2005) Long-term stimulation by active epiretinal implants in normal and RCD1 dogs. J Neural Eng 2:65–73
Yanai D, Weiland JD, Mahadevappa M, Greenberg RJ, Fine I, Humayun MS (2007) Visual performance using a retinal prosthesis in three subjects with retinitis pigmentosa. Am J Ophthalmol 143:820–827
Humayun MS, Dorn JD, Ahuja AK, Caspi A, Filley E, Dagnelie G, Salzmann J, Santos A, Duncan J, daCruz L, Mohand-Said S, Eliott D, McMahon MJ, Greenberg RJ (2009) Preliminary 6-month results from the ARGUS II epiretinal prosthesis feasibility study. Conf Proc IEEE Eng Med Biol Soc 2009:4566–4568
Caspi A, Dorn JD, McClure KH, Humayun MS, Greenberg RJ, McMahon MJ (2009) Feasibility study of a retinal prosthesis: spatial vision with a 16-electrode implant. Arch Ophthalmol 127:398–401
Chow AY, Chow VY, Packo KH, Pollack JS, Peyman GA, Schuchard R (2004) The artificial silicon retina microchip for the treatment of vision loss from retinitis pigmentosa. Arch Ophthalmol 122:460–469
Zrenner E, Gekeler F, Gabel VP, Graf HG, Graf M, Guenther E, Haemmerle H, Hoefflinger B, Kobuch K, Kohler K, Nisch W, Sachs H, Schlosshauer B, Schubert M, Schwahn H, Stelzle M, Stett A, Troeger B, Weiss S (2001) Subretinales Mikrophotodioden-Array als Ersatz für degenerierte Photorezeptoren? Ophthalmologe 98:357–363
Zrenner E, Wilke R, Zabel T, Sachs H, Bartz-Schmidt K, Gekeler F, Wilhelm B, Greppmaier U, Stett A, SUBRET Study Group (2007) Psychometric analysis of visual sensations mediated by subretinal microelectrode arrays implanted into blind retinitis pigmentosa patients. Invest Ophthalmol Vis Sci 48:E-abstract 659
Sakaguchi H, Fujikado T, Fang X, Kanda H, Osanai M, Nakauchi K, Ikuno Y, Kamei M, Yagi T, Nishimura S, Ohji M, Yagi T, Tano Y (2004) Transretinal electrical stimulation with a suprachoroidal multichannel electrode in rabbit eyes. Jpn J Ophthalmol 48:256–261
Chowdhury V, Morley JW, Coroneo MT (2005) Feasibility of extraocular stimulation for a retinal prosthesis. Can J Ophthalmol 40:563–572
Richard G, Hornig R, Keserü M, Feucht M (2007) Chronic epiretinal chip implant in blind patients with retinitis pigmentosa: long term clinical results. Invest Ophthalmol Vis Sci 48:E-Abstract 666
Gekeler F, Szurman P, Grisanti S, Weiler U, Claus R, Greiner T-O, Völker M, Kohler K, Zrenner E, Bartz-Schmidt KU (2007) Compound subretinal prosthesis with extra-ocular parts designed for human trials: successful long-term implantation in pigs. Graefes Arch Clin Exp Ophthalmol 245:230–241
Koch C, Goertz M, Mokwa W, Trieu HK, EPI-RET-3 Group (2008) The EPI-RET-3 wireless intraocular retina implant system: technical features — fabrication and assembly techniques. Invest Ophthalmol Vis Sci 49:E-Abstract 1780
Krisch I, Goertz M, Hosticka B, EPIRET 3 Group (2008) A wireless epiretinal prosthesis: the technical features - communication, power management and signal processing. Invest Ophthalmol Vis Sci 49:E-Abstract 3026
Mokwa W, Goertz M, Koch C, Krisch I, Trieu HK, Walter P (2008) Intraocular epiretinal prosthesis to restore vision in blind humans. Conf Proc IEEE Eng Med Biol Soc: 5790–5793
Laube T, Schanze T, Brockmann C, Bolle I, Stieglitz T, Bornfeld N (2003) Chronically implanted epidural electrodes in Göttinger minipigs allow function tests of epiretinal implants. Graefes Arch Clin Exp Ophthalmol 241:1013–1019
Laube T, Akguel H, Schanze T, Goertz M, Bolle I, Brockmann C, Bornfeld N, EPI RET Group (2004) First time successful epiretinal stimulation with active wireless retinal implants in Göttinger minipigs. Invest Ophthalmol Vis Sci 45:E-Abstract 4188
Akguel H, Laube T, Brockmann C, Bolle I, Bornfeld N, Schilling H, Luedtke-Handjery HC (2004) Verification of threshold parameters and tissue compatibility of IrOx film-electrodes on epiretinal electrical stimulation of retina in mini pigs. Invest Ophthalmol Vis Sci 45:E-Abstract 4184
Prince JH, Diesem CD, Eglitis I, Ruskell GL (1960) Anatomy and histology of the eye and orbit in domestic animals. Charles C Thomas, Springfield
Bertschinger DR, Beknazar E, Simonutti M, Safran AB, Sahel JA, Rosolen SG, Picaud S, Salzmann J (2008) A review of in vivo animal studies in retinal prosthesis research. Graefes Arch Clin Exp Ophthalmol 246:1505–1517
Klauke S, Goertz M, Rein S, Hoehl D, Thomas U, Eckhorn R, Bremmer F, Wachtler T (2011) Stimulation with a wireless intraocular epiretinal implant elicits visual percepts in blind humans. Invest Ophthalmol Vis Sci 52:449–455
Schwarz M, Ewe L, Hausschild R, Hosticka BJ, Huppertz J, Kolnsberg S, Mokwa W, Trieu HK (2000) Single chip CMOS imagers and flexible microelectronic stimulators for a retina implant system. Sens Actuators A83:40–46
Koch C, Fassbender H, Nolten U, Görtz M, Mokwa W (2008) Fabrication and assembly techniques for a 3rd generation wireless epiretinal prosthesis. In: Schnakenberg U (ed) Proceedings of the 19th MicroMechanics Europe Workshop 2008, Aachen, Germany. VDI/VDE IT, Berlin, pp 365–368, ISBN: 978-3-00-025529-8
Slavcheva E, Vitushinski R, Mokwa W, Schnakenberg U (2004) Sputtered iridium oxide films as charge injection material for functional electrostimulation. J Electrochem Soc 151:E226–E237
Niessing M, Messner A, Coenen PW, Röthgen H, Hoehl D, Thomas U, EPIRET 3 Group (2008) The Epiret3 wireless intraocular retina implant system: retina prosthesis production techniques. Invest Ophthalmol Vis Sci 49:E-Abstract 1782
Walter P, Kisvárday ZF, Goertz M, Alteheld N, Roessler G, Stieglitz T, Eysel UT (2005) Cortical activation via an implanted wireless retinal prosthesis. Invest Ophthalmol Vis Sci 46:1780–1785
Walter P, Heimann K (2000) Evoked cortical potentials after electrical stimulation of the inner retina in rabbits. Graefes Arch Clin Exp Ophthalmol 238:315–318
Duncker GIW, Rochels R (1996) Delayed suprachoroidal hemorrhage after penetrating keratoplasty. Int Ophthalmol 19:173–176
Rothman JS, Abad JC, Kornmehl EW (2009) Intraoperative complications of penetrating keratoplasty. In: Brightbill FS (ed) Corneal surgery — theory, technique and tissue. Mosby Elsevier, St. Louis, p 454
Alio JL, Rodriguez Rats JL, Galal A (2005) Microincision cataract surgery. In: Vajpayee RB, Sharma N, Pandey SK, Titiyal JS (eds) Phacoemulsification surgery. Jaypee Brothers Medical Publishers Ltd, New Delhi, p 162
Savini G, Zanini M, Buratto L (2003) Incisions. In: Buratto L, Werner L, Zanini M, Apple D (eds) Phacoemulsification principles and techniques. Slack Inc, Thorofare NJ, pp 69–79
Schanze T, Wilms M, Eger M, Hesse L, Eckhorn R (2002) Activation zones in cat visual cortex evoked by electrical retina stimulation. Graefes Arch Clin Exp Ophthalmol 240:947–954
Laube T, Bornfeld N (1999) Evaluation of stability and position of epi-retinal implants with the RetCam 120™ digital fundus camera. Invest Ophthalmol Vis Sci 40:E-Abstract 3888
Walter P, Szurman P, Vobig M, Berk H, Lüdtke-Handjery HC, Richter H, Mittermayer C, Heimann K, Sellhaus B (1999) Successful long-term implantation of electrically inactive epiretinal microelectrode arrays in rabbits. Retina 19:546–552
Majji AB, Humayun MS, Weiland JD, Suzuki S, D'Anna SA, de Juan E Jr (1999) Long-term histological and electrophysiological results of an inactive epiretinal electrode array implantation in dogs. Invest Ophthalmol Vis Sci 40:2073–2081
Roessler G, Laube T, Brockmann C, Kirschkamp T, Mazinani B, Goertz M, Koch C, Krisch I, Sellhaus B, Trieu HK, Weis J, Bornfeld N, Röthgen H, Messner A, Mokwa W, Walter P (2009) Implantation and explantation of a wireless epiretinal retina implant device: observations during the EPIRET3 prospective clinical trial. Invest Ophthalmol Vis Sci 50:3003–3008
Humayun MS, Weiland JD, Fujii GY, Greenberg R, Williamson R, Little J, Mech B, Cimmarusti V, Van Boemel G, Dagnelie G, de Juan E Jr (2003) Visual perception in a blind subject with a chronic microelectronic retinal prosthesis. Vision Res 43:2573–2581
Humayun MS (2009) Preliminary results from the Argus II feasibility study: a 60 electrode epiretinal prosthesis. Invest Ophthalmol Vis Sci 50:E-Abstract 4744
Tunc M, Humayun M, Xuanhong C, Ratner BD (2008) A reversible thermosensitive adhesive for retinal implants - in vivo experience with plasma-deposited poly(N-isopropyl acrylamide). Retina 28:1338–1343
Besch D, Sachs H, Szurman P, Gülicher D, Wilke R, Reinert S, Zrenner E, Bartz-Schmidt KU, Gekeler F (2008) Extraocular surgery for implantation of an active subretinal visual prosthesis with external connections: feasibility and outcome in seven patients. Br J Ophthalmol 92:1361–1368
Lucke JN, Hall GM, Lister D (1977) Anaesthesia of pigs sensitive to malignant hyperthermia. Vet Record 100:45–48
Lorkin PA, Lehmann H (1983) Investigation of malignant hyperthermia: analysis of skeletal muscle proteins from normal and halothane sensitive pigs by two dimensional gel electrophoresis. J Med Genetics 20:18–24
Acknowledgements
The authors would like to thank all co-workers of the EPI RET work group. This study was supported by grants from the Federal Ministry of Education and Research (01KP0402, 01KP0403). Shirley Heinen is acknowledged for linguistic improvement of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have full control of all primary data, and they agree to allow Graefe's Archive for Clinical and Experimental Ophthalmology to review their data upon request.
Rights and permissions
About this article
Cite this article
Laube, T., Brockmann, C., Roessler, G. et al. Development of surgical techniques for implantation of a wireless intraocular epiretinal retina implant in Göttingen minipigs. Graefes Arch Clin Exp Ophthalmol 250, 51–59 (2012). https://doi.org/10.1007/s00417-011-1756-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-011-1756-z