
Abstract
In the assessment of health risks after nuclear accidents, some health consequences require special attention. For example, in their 2013 report on health risk assessment after the Fukushima nuclear accident, the World Health Organisation (WHO) panel of experts considered risks of breast cancer, thyroid cancer and leukaemia. For these specific cancer types, use was made of already published excess relative risk (ERR) and excess absolute risk (EAR) models for radiation-related cancer incidence fitted to the epidemiological data from the Japanese A-bomb Life Span Study (LSS). However, it was also considered important to assess all other types of solid cancer together and the WHO, in their above-mentioned report, stated “No model to calculate the risk for all other solid cancer excluding breast and thyroid cancer risks is available from the LSS data”. Applying the LSS models for all solid cancers along with the models for the specific sites means that some cancers have an overlap in the risk evaluations. Thus, calculating the total solid cancer risk plus the breast cancer risk plus the thyroid cancer risk can overestimate the total risk by several per cent. Therefore, the purpose of this paper was to publish the required models for all other solid cancers, i.e. all solid cancers other than those types of cancer requiring special attention after a nuclear accident. The new models presented here have been fitted to the same LSS data set from which the risks provided by the WHO were derived. Although it is known already that the EAR and ERR effect modifications by sex are statistically significant for the outcome “all solid cancer”, it is shown here that sex modification is not statistically significant for the outcome “all solid cancer other than thyroid and breast cancer”. It is also shown here that the sex-averaged solid cancer risks with and without the sex modification are very similar once breast and thyroid cancers are factored out. Some other notable model differences between those already published for all solid cancers and those presented here for all other solid cancers are also given here. The models presented here can be used to improve on the methodology adopted by WHO after Fukushima and could contribute to emergency preparedness for future nuclear accidents.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In assessments of radiation-related cancer risk after nuclear accidents, estimates of all solid cancer risk and leukaemia risk per unit organ/tissue dose can broadly represent the overall impact of radiation exposure on cancer risk. Pooling radiation epidemiological data on all solid cancers together and calculating risks of this highly heterogeneous grouping with respect to one type of organ dose (e.g. colon dose) can account for radiation causing cancer in most body organs/tissues and enhance the statistical power of the risk estimates. However, in comparison with standard models for all solid cancer radiation-related risks, some organs/tissues have higher risks per unit organ dose and markedly different risk effect modification by sex, attained age and age-at-exposure. For example, in their 2013 report, UNSCEAR (2013) found strong evidence for higher risks of breast cancer, brain tumours, thyroid cancer and non-CLL leukaemia after radiation exposure in childhood compared with exposure at adult ages. For cancer sites where the relevant organ/tissue doses are highly heterogeneous (e.g. the thyroid gland, following an intake of radioactive iodine) or for sites close to the body surface (e.g. breast), the risk of all solid cancers combined with respect to colon dose will not fully account for these risks.
The World Health Organisation (WHO), in their 2013 health risk assessment (HRA) after the Fukushima nuclear accident (WHO 2013; Etherington et al. 2014; Walsh et al. 2014), presented cancer risks of leukaemia, breast cancer, thyroid cancer and all solid cancers. Calculating the total solid cancer risk plus the breast cancer risk plus the thyroid cancer risk can overestimate the total risk by several per cent. The choice of the grouping “all solid cancer combined” meant that the risks of breast and thyroid cancers had an overlap in the overall risk evaluations. This was necessary at the time because no risk models for all solid cancers other than breast and/or thyroid cancers had been published. The purpose of this article is to present such required models for all other solid cancers, i.e. all solid cancers other than those types of cancer requiring special attention after a nuclear accident.
Radiation epidemiological data from survivors of the World War II Hiroshima and Nagasaki atomic bombings were central to the WHO—Fukushima HRA (WHO 2013). The Life Span Study (LSS) of A-bomb survivors provides valuable radiation epidemiological data and quantitative assessments of the radiation-related detrimental health risks (Preston et al. 2003, 2004, 2007; Ozasa et al. 2012). The most recent data for all solid cancer incidence with 17,448 first primary cancer cases, analysed by Preston et al. (2007), are the largest data set in terms of numbers of cases currently available (i.e. compared to 8613 first primary incident solid cancers in Thompson et al. (1994) 9335 deaths from solid cancer in Preston et al. (2003) and 10,929 deaths from solid cancer in Ozasa et al. (2012). Preston et al. (2007) have already reported cancer risk models for all solid cancers and for a comprehensive set of organ/tissue sites. These are the risk models that were found to be particularly useful and applied in the WHO—Fukushima HRA (WHO 2013). For the specific cancer sites considered by WHO (2013), use was made of excess relative risk (ERR) and excess absolute risk (EAR) models for radiation-related solid cancer incidence fitted to the epidemiological data from the LSS. In this article, models are fitted to the LSS data and presented here for all other solid cancers, i.e. all solid cancers other than those types of solid cancer requiring special attention after a nuclear accident (breast and thyroid cancers). The models presented here can be used to improve on the methodology adopted by WHO after Fukushima (WHO 2013) and contribute to emergency preparedness for future nuclear accidents.
Materials and methods
Risk models and data set
The most recent all solid cancer incidence data for the follow-up 1958–1998 (Preston et al. 2007, data file: ds02can.dat, results file: ds02can.log from www.rerf.or.jp), with the DS02 dosimetry (Young and Kerr 2005) have been used. The EAR and ERR models with a linear dose response from the study by Preston et al. (2007) were applied for all solid cancers, breast and thyroid cancer incidence. The data cover the period from 1958 to 1998 with a total of 17,448 cases of solid cancers (ICD10, C00–C89), 1073 female breast cancers, 9 male breast cancers (C50) and 471 thyroid cancers (C73), amongst 111,952 persons (52 % alive) contributing almost 3 million person-years. Use is made of a general rate (hazard) model of the form
for the excess relative risk (ERR) or excess absolute risk (EAR), where λ 0(a, e, s, c, nic) is the baseline cancer death rate, at attained age, a, age-at-exposure e, with indicator variables for sex, s (M = male, F = female), city, c (H = Hiroshima, N = Nagasaki), and “not in either city at the time of the bombs”, nic. The organ absorbed doses from γ-rays and neutrons is d = d γ + RBE ∙ d n, i.e. the organ absorbed doses weighted by the relative biological effectiveness (RBE) of neutrons relative to gammas. The value of 10 for RBE has been widely used in the past for weighting the organ doses and is also applied here, in spite of indications for larger values (Kellerer et al. 2006; Rühm and Walsh 2007; Walsh 2013). Although the baseline rates can be dealt with by stratification, a fully parametric model is adopted here:
where β 0,M,…, β 14,F are fit parameters.
This is the model of Preston et al. (2007). The ERR and EAR models considered were of the form
i.e. a linear dose response with adjustments in the ERR and EAR for age-related explanatory covariables, as defined above, and sex, where s = −1 for males or +1 for females. The four fit parameters of each model are either the ERR central estimate, k d (ERR/Gy), or the EAR central estimate, k d (EAR/Gy (in cases per 10,000 person-years)), and the effect modifiers of these central risk estimates by sex, t, age-at-exposure, g e, and age attained, g a.
Model fit parameters and goodness of fit measures were obtained by optimising the models to the data via Poisson regression with the AMFIT module of the EPICURE software (Preston et al. 1993).
Results
The results are shown in Table 1 which gives the model fit parameters and deviances of a set of models, either as reported in Preston et al. (2007) (for the outcomes all solid, breast, thyroid and brain cancers) or as calculated here (for the outcomes all solid minus thyroid, all solid minus breast, all solid minus thyroid minus breast). A large number of decimal places have been retained in this table because these parameters are suitable for future applications in the calculation of lifetime attributable risks (Kellerer et al. 2001). Quantities suitable for assessing model goodness of fit to the data are also given in Table 1 (deviance and degrees of freedom), but the p values for parameter significance are only given, if >0.05. The thyroid cancer models from Preston et al. (2007) also contain an adjustment for whether or not the subjects were in the adult health survey (AHS) because baseline thyroid cancer rates in AHS participants were estimated to be about 40 % higher than those for other cohort members.
Most of the model parameters for the all solid cancer model are similar to those for the all solid minus thyroid cancer model, the all solid minus breast cancer model and the all solid minus thyroid minus breast cancer model. The linear dose response central (at a = 70, e = 30 years) estimates with standard errors for the models: all solid cancers, all solid minus thyroid, all solid minus breast and all solid minus thyroid minus breast, are 0.47 ± 0.04, 0.46 ± 0.05, 0.42 ± 0.04 and 0.42 ± 0.05 for ERR/Gy, respectively, and 51.6 ± 5.0, 51.7 ± 5.2, 47.3 ± 5.2 and 48.5 ± 5.4 for EAR/Gy (in cases per 10,000 person-years) also, respectively—i.e. all similar within 10 %. However, there are noteworthy differences in the apparent sex effect modifications, which are not found to be statistically significant for the EAR for the outcomes “all solid minus thyroid cancer” and “all solid minus breast cancer” (Table 1). Also the apparent sex effect modifications are not found to be statistically significant for either the ERR or the EAR models for the outcome “all solid minus thyroid minus breast cancer” (Table 1—where the fit parameters for the sex effect modifications correspond to a female-to-male ratio of 1.39 and 0.76 for the ERR and EAR models, respectively [compared to statistically significant ratios of 1.65 and 1.3, respectively, for the original all solid cancer model from Preston et al. (2007)]. In terms of goodness of fit, when comparing the ERR models for the outcome “all solid minus thyroid minus breast cancer” with and without the sex effect modification, there is no significant improvement in model fit when including the sex effect modification (change in deviance = 2.51). Likewise for the EAR models for the outcome “all solid minus thyroid minus breast cancer” with and without the sex effect modification (change in deviance = 2.65). Given the importance of the outcome “all solid minus thyroid minus breast cancer” as noted by the WHO in the Fukushima HRA (WHO 2013), Table 1 also gives the fit parameters for this outcome in a model without the sex modification. Omitting the sex modification causes the central estimates with standard errors (at a = 70, e = 30 years) for ERR/Gy to change from 0.42 ± 0.05 to 0.40 ± 0.05 and for EAR/Gy (in cases per 10,000 person-years) to change from 48.5 ± 5.4 to 44.7 ± 4.8. The “Appendix” Table 2 compares the lifetime attributable risk (LAR), as calculated for the all solid cancer model in the WHO Fukushima HRA (Walsh et al. 2014) with the LAR calculated with the new model presented here for the outcome all solid minus thyroid minus breast cancer without the sex modification.
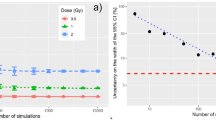
The overall sex-averaged attained-age effect modification for the outcomes of all solid cancers, all solid minus thyroid, all solid minus breast and all solid minus thyroid minus breast (computed with and without the sex modifier) is given in Fig. 1 for ERR/Gy (left-hand panels) and EAR/Gy (in cases per 10,000 person-years) (right-hand panels) for three different ages-at-exposure (i.e. e = 10 years (at the top and with inset), 30 years (in the middle) and 50 years (at the bottom). The abscissas scaling in Fig. 1 has been chosen to start from a = e + 5 years, in line with the 5-year latent period for cancer that was considered suitable by the WHO in their Fukushima HRA (WHO 2013). From Fig. 1, it can be seen that the largest differences are for ERR at young ages-at-exposure and young attained ages (see inset of Fig. 1). The attained-age effect modification is less steep in the ERR model and more steep in the EAR model for the outcome “all solid minus thyroid minus breast cancer” than for the outcome “all solid cancer”. This can be seen by comparing the fit parameters in Table 1 or from Fig. 1.

Shows, for the four different outcomes (as given in the key), the sex-averaged attained-age effect modification of the ERR/Gy colon dose (left-hand panels) and EAR/Gy colon dose (in cases per 10,000 person-years) (right-hand panels) for three different ages-at-exposure [i.e. 10 years (at the top and with inset), 30 years (in the middle) and 50 years (at the bottom)]
Discussion
The World Health Organisation (WHO), in their 2013 HRA after the Fukushima nuclear accident (WHO 2013; Etherington et al. 2014; Walsh et al. 2014), paid special attention to the outcomes leukaemia, breast cancer and thyroid cancer, but in assessing all other types of solid cancer had to use an already published model for all solid cancers. WHO 2013 noted that no risk models for all solid cancers other than breast and/or thyroid cancers had been published. The purpose of this article is therefore to present such required models for all other solid cancers, i.e. all solid cancers other than those types of cancer requiring special attention after a nuclear accident (breast cancer and thyroid cancer). It was found that for these “other solid cancer outcome groupings”, the gender effect modification is often much weaker than for the all solid cancer outcome. Also the age-attained effect modification for these “other solid cancer outcome groupings” can be weaker or stronger than in the all solid cancer model. Therefore, it is possible to improve on the methodology applied in WHO 2013, by applying models similar to those presented here for solid cancer sites other than those requiring specific attention after a nuclear accident.
Examples of results obtained with this improved methodology, specific to the situation after the Fukushima accident, are given in “Appendix” Table 2 in terms of the lifetime risk attributable to the radiation exposure, lifetime attributable risk (LAR). LAR is calculated by integrating the ERR (relative to Japanese sex-specific population cancer rates) and EAR models given in Table 1, over age attained (see WHO 2013 or Walsh et al. 2014 for a full description of the LAR calculation—the main LAR equations have also been presented in the “Appendix”). Table 2 compares the LAR, as calculated for the all solid cancer model in the WHO Fukushima HRA (Walsh et al. 2014) with the LAR calculated with the new ERR and EAR models without the sex modification presented here for the outcome all solid minus thyroid minus breast cancer. It can be seen from Table 2 that the LARs for the outcome all solid minus thyroid minus breast cancer without the ERR and EAR sex modifications are either smaller than or similar in magnitude to the LAR for the outcome all solid cancers for females or males, respectively. However, due to the low or very low doses received, the theoretically increased small radiation-related cancer risks relevant to members of the public in the Fukushima prefecture are not expected to become discernible in cancer statistics in the future (UNSCEAR 2014), and so an improvement in methodology may not be highly relevant here. On the other hand, the models presented here can be a useful contribution to emergency preparedness for future nuclear accidents.
The UNSCEAR Fukushima report (UNSCEAR 2014) made use of already published LAR results, some of which were taken from the WHO-HRA (WHO 2013). In Annex A, Table E1 (UNSCEAR 2014), the all cancer LARs with respect to colon dose was decremented by the LAR for thyroid cancer with respect to colon dose and then augmented by the thyroid cancer LAR with respect to thyroid dose. This is an approximation, because it does not fully take into account that the LAR for solid cancer has been calculated from ERR and EAR models with different risk effect-modifying factors than the ones for thyroid cancers (i.e. see Table 1, from which it can be seen that there are particularly large differences in the attained-age modification of EAR between the all solid cancer model and the thyroid model). The new models published here (in this case, the model for all solid cancers minus thyroid cancer) avert the need for this type of approximation in future health risk assessments.
As pointed out by Preston et al. (2007, p. 12) “While apparent gender effects on the ERR may reflect differences in background cancer rates and/or possible gender differences in radiosensitivity, gender differences in the EAR, which is not influenced by background rates, might be thought to be a more direct indication of gender differences in radiosensitivity”. It is therefore an interesting observation that for the cancer outcomes all solid minus thyroid and all solid minus breast, the sex modification is much weaker in the EAR models than in the ERR models. This is also further evidence for a lack of sex differences in the preferred models for the outcome all solid minus thyroid minus breast. This is in contrast to the sex specificity in the model for thyroid cancer as already pointed out (Preston et al. 2007), i.e. the gender-specific EAR estimates were 1.9 for females and 0.5 for males, and resulted in the largest female/male ratio (3.6) in the cohort—it is this effect that is possibly influencing the significant sex effect in the all solid cancer EAR model used by Preston et al. (2007).
It is also interesting to note that other practical applications in radiation health risk assessments may also need special groupings of “remainder cancers” with special radiation risk models for these remainder groupings. For example, in comparisons of brain and central nervous system (CNS) or non-CNS all solid cancer risks in studies of computer tomography (CT) risks after brain CT to the corresponding LSS risks, the already published LSS brain plus CNS risk model would be appropriate and an extra model for the outcome all solid cancers minus brain and CNS cancers. However, here both models, i.e. for the outcomes all solid cancers and all solid cancers minus CNS, are quite similar (see “Appendix” Table 3). Since UNSCEAR (2013) reported increased radiation sensitivity in children for the sites thyroid, breast, skin and brain cancers, a model for the remaining types of solid cancer could also be useful (but is not provided here). Occupational compensation claims may also require as yet unpublished groupings of different cancer types into functional groups, e.g. respiratory tract cancers or digestive tract cancers. One argument against the requirement for specially optimised remaining types or grouped types of solid cancer radiation risk models is that it is possible to combine the individual risks from the individual models for the cancer sites required (as done by UNSCEAR 2008). However, with this approach, there are many more sources of uncertainties contributing to the combined risks, i.e. one has several model parameters (each with an associated uncertainty) for each site that needs to be combined rather than just the model parameters for the one remainder grouping or special grouping.
A suggestion for further work is to update the new models provided here, when the updated LSS models, based on an extended follow-up period and more cancer cases, are published in the next few years as a contribution to emergency preparedness for future nuclear accidents.
Conclusion
Radiation risk models for all solid cancers other than those types of solid cancer requiring individual assessments after a nuclear accident (thyroid and breast cancers) have been presented here. It is shown that although it is known already that the EAR and ERR effect modifications by sex are statistically significant for the outcome “all solid cancer”, it is not statistically significant for the outcome “all solid cancer other than thyroid and breast cancer”. Some other notable model differences between those already published for all solid cancers and those presented here for all other solid cancers are also given here. It is recommended to update the new models presented here, when the new LSS data with extended follow-up and more cancer cases become available.
References
Etherington G, Zhang W, Harrison J, Walsh L (2014) Workers doses and potential health effects resulting from the accident at the Fukushima nuclear power plant in 2011. Int J Radiat Biol 16:1–24
Kellerer AM, Nekolla E, Walsh L (2001) On the conversion of solid cancer excess relative risk into lifetime attributable risk. Radiat Environ Biophys 40:249–257
Kellerer AM, Rühm W, Walsh L (2006) Indications of the neutron effect contribution in the solid cancer data of the A-bomb survivors. Health Phys 90(6):554–564
Ozasa K, Shimizu Y, Suyama A, Kasagi F, Soda M, Grant EJ, Sakata R, Sugiyama H, Kodama K (2012) Studies of the Mortality of Atomic Bomb Survivors, Report 14, 1950–2003: an overview of cancer and noncancer diseases. Radiat Res 177(3):229–243
Preston DL, Lubin JH, Pierce DA (1993) Epicure user’s guide. HiroSoft International Corp, Seattle
Preston DL, Shimizu Y, Pierce DA, Suyama A, Mabuchi K (2003) Studies of the mortality of atomic bomb survivors. Report 13: solid cancer and noncancer disease mortality: 1950–1997. Radiat Res 160:381–407
Preston DL, Pierce DA, Shimizu Y, Cullings HM, Fujita S, Funamoto S, Kodama K (2004) Effects of recent changes in atomic bomb survivors dosimetry on cancer mortality risk estimates. Radiat Res 162:377–389
Preston DL, Ron E, Tokuoka S, Funamoto S, Nishi N, Soda M, Mabuchi K, Kodama K (2007) Solid cancer incidence in atomic bomb survivors: 1958–1998. Radiat Res 168:1–64
Rühm W, Walsh L (2007) Current risk estimates based on the A-bomb survivors data—a discussion in terms of the ICRP recommendations on the neutron weighting factor. Radiat Prot Dosim 126(1–4):423–431
Thompson DE, Mabuchi K, Ron E, Soda M, Tokunaga M, Ochikubo S, Sugimoto S, Ikeda T, Terasaki M, Izumi S, Preston DL (1994) Cancer incidence in atomic bomb survivors. Part II: solid tumors, 1958–1987. Radiat Res 137:S17–S67
United Nations Effects of Ionizing Radiation (2008) United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2006 Report. Volume I. Annex A: Epidemiological studies of radiation and cancer. United Nations, New York
United Nations Effects of Ionizing Radiation (2013). United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2013 Report. Volume II. Annex B: Effects of radiation exposure of children, New York. http://www.unscear.org/docs/reports/2013/UNSCEAR_2013_Report_Annex_B_Children.pdf
United Nations Effects of Ionizing Radiation (2014) United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2013, Volume 1, Levels and effects of radiation exposure due to the nuclear accident after the 2011 great east-Japan earthquake and tsunami. United Nations Publications, New York
Walsh L (2013) Neutron relative biological effectiveness for solid cancer incidence in the Japanese A-bomb survivors—an analysis considering the degree of independent effects from γ-ray and neutron absorbed doses with hierarchical partitioning. Radiat Environ Biophys 52(1):29–36
Walsh L, Zhang W, Shore RE, Auvinen A, Laurier D, Wakeford R, Jacob P, Gent N, Anspaugh LR, Schüz J, Kesminiene A, van Deventer E, Tritscher A, del Rosario Pérez M (2014) A framework for estimating radiation-related cancer risks in Japan from the 2011 Fukushima Nuclear Accident. Radiat Res 182(5):556–572
WHO (2013) Health risk assessment from the nuclear accident after the 2011 Great East Japan Earthquake and Tsunami based on a preliminary dose estimation. WHO. http://www.who.int/ionizing_radiation/pub_meet/fukushima_risk_assessment_2013/en
Young R, Kerr GD (eds) (2005) DS02: Reassessment of the atomic bomb radiation dosimetry for Hiroshima and Nagasaki, Dosimetry System 2002, DS02 Vols 1 and 2. Radiation Effects Research Foundation, Hiroshima
Acknowledgments
This work makes use of the data obtained from the Radiation Effects Research Foundation (RERF) in Hiroshima, Japan. RERF is a private foundation funded equally by the Japanese Ministry of Health and Welfare and the US Department of Energy through the US National Academy of Sciences. The conclusions in this work are those of the author and do not necessarily reflect the scientific judgement of RERF or its funding agencies.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Although the main lifetime attributable risk (LAR) equations are presented here for the convenience of the reader, please see WHO (2013) or Walsh et al. (2014) for a full description of the LAR calculation and full details of the Japanese population statistics applied.
The lifetime attributable risk from one yearly dose (d), LAR (d, e, s), specifies the sex (s)- and age-at-exposure (e)-specific cumulative probability of specific cancer attributable to radiation exposure over a period up to a maximum age (a max). LAR is based on the combined excess risk (ER) model calculated with Japanese age- and sex-specific baseline cancer incidence rates m(a, s):
where d is the dose delivered to the organ/tissue during 1 year of exposure for age-at-exposure e and L is the minimum latency period between the delivery of the dose to the organ and the expression of the radiation-induced risk (i.e. 5 years, for the risks presented in Table 2). a max was taken to be 89 years (an arbitrary choice). The survival curve ratio, \(S_{aj} (a,\;s) /S_{aj} (e,\;s)\), is the probability of surviving to age a, adjusted for cancer-free survival, with the condition that the probability equals one at age at beginning of risk, corresponding to age-at-exposure for exposed people. LAR was obtained from Eq. 2 by numerical integration over age, a, in 1-year intervals.
The lifetime attributable risk, based on a lifetime organ/tissue dose accumulated over a maximum of 70 years, D, LAR (D, e, s), is a summation of integral terms from Eq. 2, i.e.
where d i is the yearly dose during the ith year and e is the age-at-exposure in year i (i.e. the doses were treated as age-at-exposure dependent on conferring the risk). The choice to base the LAR results given in Table 2, on 10 mGy first-year organ/tissue dose or 20 mGy lifetime organ/tissue dose is partly arbitrary because the presented risks may be linearly scaled to other doses. However, the ratio of the lifetime dose to the first-year dose, of two, came from an expert evaluation (WHO 2013) that took observations from the Chernobyl disaster, considerations of remedial environmental clean-up actions in the Fukushima prefecture and some other factors into account.
Rights and permissions
About this article

Cite this article
Walsh, L., Zhang, W. Radiation risk models for all solid cancers other than those types of cancer requiring individual assessments after a nuclear accident. Radiat Environ Biophys 55, 9–17 (2016). https://doi.org/10.1007/s00411-015-0629-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00411-015-0629-y