
Abstract
The objectives of this study were to examine middle ear biopsies from Greenlandic patients with chronic otitis media (COM) for the presence of mucosal biofilms and the bacteria within the biofilms. Thirty-five middle ear biopsies were obtained from 32 Greenlandic COM patients admitted to ear surgery. All biopsies were examined by means of peptide nucleic acid-fluorescent in situ hybridization (PNA-FISH), and if possible culture and polymerase chain reaction (PCR) of the 16s rDNA and sequencing. Light microscopy and confocal laser scanning microscopy were used. Skin biopsies from 23 of the patients served as controls. PNA-FISH showed morphological signs of biofilms in 15 out of 35 (43 %) middle ear biopsies. In the control skin biopsies, there were signs of biofilms in eight out of 23 biopsies (30 %), probably representing skin flora. PCR and 16s sequencing detected bacteria in seven out of 20 (35 %) usable middle ear biopsies, and in two out of ten (20 %) usable control samples. There was no association between biofilm findings and PCR and 16s sequencing. Staphylococci were the most common bacteria in bacterial culture. We found evidence of bacterial biofilms in 43 % of middle ear biopsies from patients COM. The findings may indicate that biofilms are a part of the pathogenesis in recurrent episodes of ear discharge in COM, but further investigations are necessary.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Biofilms can be defined as a coherent cluster of bacterial cells imbedded in a biopolymer matrix, which, compared with planktonic (free floating) cells, shows increased tolerance to antimicrobials and resists the antimicrobial properties of the host defense [1]. Bacteria in biofilms are thus difficult to eradicate, and have been increasingly associated with chronic infections. In otorhinolaryngology, biofilms have been associated with diseases such as chronic sinusitis and otitis media with effusion (OME) [2]. Biofilms have been linked to infections in the middle ear since 1998, when Rayner et al. [3] found bacterial mRNA in patients with culture negative OME. Biofilms in the human middle ear with chronic suppurative otitis media (CSOM), were described in 2004 by Coates [4], and in 2006 Hall-Stoodley et al [5] detected biofilms in middle ear mucosa in children with OME and recurrent acute otitis media. Biofilms and OME have since been further investigated. A possible link between chronic otitis media (COM) and bacteria in biofilms has been less studied. We have previously found morphological evidence of biofilms in CSOM [6]. In addition to our results, Lee et al. [7] also detected biofilms in the middle ear in patients with CSOM. In contrast, Saunders et al. [8] found evidence of biofilms in only 1 out of 10 middle ear biopsies of patients with CSOM, while biofilms were detected in 60 % of cholesteatomas.
The prevalence of COM and CSOM among the Greenlandic population is high [9], and as a consequence hearing impairment is common. A biofilm infection in the middle ear could explain recurrent and recalcitrant episodes of otorrhea in COM, a disease otherwise characterized by a dry tympanic membrane perforation. At present, the most predominant explanations for acute exacerbation in COM are retrograde bacterial invasion from the nasopharynx or infection with entrance via the external ear canal. Thus, this study aims to examine middle ear biopsies from Greenlandic COM patients with dry perforations for the existence of mucosal biofilms and the bacteria within them. A better understanding of the disease is crucial for future treatment [10].
Material
Patients eligible for the study included 75 longitudinally enrolled Greenlandic COM patients admitted for ear surgery at the Department of Otolaryngology, Head and Neck Surgery, Rigshospitalet, Copenhagen, Denmark in the years 1993–1995. In this study, COM was defined as a dry permanent perforation of the tympanic membrane without active otorrhea or a healed tympanic membrane with evidence of recent perforation, e.g., severe atrophy. All patients had been on a waiting list for ear surgery due to COM for at least 5 years prior to ear surgery. Furthermore, all patients had been examined annually in Greenland, by a travelling otolaryngologist, confirming the chronic disease. Sixteen patients were excluded, since the biopsies had been used in other studies. In 18 patients no biopsies were taken, two patients did not undergo surgery and seven biopsies were too small for analysis. These patients were excluded as well. Thus, a total of 32 patients with available middle ear biopsies were included.
The study was approved by the local ethical committee (KF 01–060/93) and informed consent was obtained from all participants.
Methods
Middle ear biopsies were obtained during surgery and placed on a non-fluorescent sheet. Biopsies from the middle ear were obtained with cup forceps and skin biopsies with a scalpel. The biopsies were immediately frozen and stored at −80 °C in a folio bag. Thirty-one patients had biopsies taken from the middle ear mucosa (MEM) and in one patient a biopsy was taken from the tympanic membrane. Furthermore, additional biopsies from the mastoid of two patients were obtained, and from one cholesteatoma found during surgery. Thus, a total of 35 middle ear biopsies were investigated. Control specimen biopsies from retro auricular skin, the skin of the auricle or the external auditory canal, were taken in 23 patients to examine for potential contamination between the skin and the middle ear biopsies during surgery. To remove the transient bacterial flora and reduce the resident bacterial flora, surgical disinfection was performed. This included cleaning the skin twice with 0.5 % chlorhexidine digluconate around and behind the ear, in the auricle and the entrance to the external auditory canal. The control biopsies were examined blinded to the investigators. Biofilm detection by means of peptide nucleic acid-fluorescent in situ hybridization (PNA-FISH) had the highest priority and all samples were investigated by this method. The biopsies were cut in half and further examined for bacterial DNA by polymerase chain reaction (PCR) of the 16s rDNA and sequenced. Twenty middle ear biopsies and 10 control biopsies were large enough for PCR analysis and sequencing. In addition to this, tissue samples from 23 middle ear biopsies and 8 control biopsies were subjected to bacterial culturing.
PNA-FISH
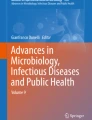
The biopsies were examined using a universal bacterial probe (16S rRNA sequence coupled to Texas red) and a species-specific Staphylococcus aureus probe (S. aureus specific 16s rRNA sequence coupled to fluorescein isothiocyanate—FITC) (AdvanDx Inc.) [11, 12]. The biopsies were fixed in 4 % paraformaldehyde, embedded in paraffin and sliced into 3–4 μm specimens before being mounted on slides. The biopsies were then deparaffinized with xylene, 2 × 5 min and rehydrated with a gradient of ethanol and water, 99 % for 2 × 3 min, 96 % for 2 × 3 min, and finally Milli-Q water for 3 × 3 min. Once dry, the samples were hybridized with fluorescently labeled PNA-FISH probes at 55 °C for 90 min followed by wash with a 1× solution of the supplied washing buffer for 30 min at 56 °C. Mounting media containing 4’,6-diamidino-2-phenylindole (DAPI) (Vector Laboratories) was used to stain DNA. Biopsies were examined with a Zeiss LSM 710 microscope at 630–1,000× magnification using 1, 4 numerical aperture objectives. Photos of fluorescent areas in tissue, including biofilms, artifacts, and autofluorescence were taken and examined unblinded. The photos were then evaluated blinded by a biofilm expert (Fig. 1a–c). Biofilms were defined by the identification of physical aggregated bacteria in clusters [13]. Inconsistencies in the results between the two evaluators were found in 14 biopsies. Twelve of these were rehybridized and examined blinded by means of confocal laser scanning microscopy (CLSM) (Fig. 1d). Rehybridization was not possible in two cases.

a Monospecies S. aureus biofilms (arrows) in a biopsy from the middle ear mucosa of a patient with COM. Biofilms were visualized with species-specific PNA-FISH and examination with immersion microscopy. The S. aureus PNA probe was coupled to fluorescein isothiocyanate (FITC). b Multispecies biofilms (arrows) in the middle ear mucosa of a patient with COM. Biofilms containing both S. aureus and other cocci were demonstrated by PNA-FISH and immersion microscopy. The eubacterial PNA probe was coupled to Texas red. c Small biofilm colony of S. aureus (arrow) in a skin biopsy. Both species-specific and universal bacterial PNA-FISH analysis was performed. The universal bacterial PNA probe was coupled to Texas red. d 3D micrograph of a combined FITC-labeled species-specific and Texas Red-labeled universal bacterial PNA-FISH probe showing a biofilm containing bacteria other than S. aureus (arrow). The micrograph was 10.83 μm deep in total and consists of 22 stacks with a step size of 0.5 μm. Photos a–c were processed for display using AxioVision LE (Carl Zeiss MicroImaging GmbH) software and Paint.NET software. Photo D was processed using ImageJ. The scale bar represents 10 μm. All micrographs were obtained using a 63 × 1.4 numerical aperture oil immersion objective
PCR and 16s sequencing
DNA from the biopsies was purified using the DNeasy Blood and Tissue kit (Qiagen GmbH). The manufacturer’s instructions were followed, but with the addition of bovine serum albumin (BSA) and lysozyme for enhanced DNA yield. This procedure included lysis of tissue for 4 h using proteinase K and the supplied chemicals followed by centrifugation through a spin column with changing buffers as described and supplied by the manufacturer. Bacterial identification was performed using a MicroSeq 500 16s rDNA bacterial identification kits (Perkin-Elmer Applied Biosystems) according to the manufacturer’s instructions. In short, once DNA had been purified, PCR was used to amplify the first 500 base pairs of the 16s rRNA on a Veriti 96-well fast thermal cycler (Applied Biosystems) according to the manufacturer’s instructions. The PCR product was purified using ExoSap-it (Affymetrix) followed by the sequencing reaction as supplied in the 16s rDNA bacterial identification kit. The samples were then purified using DTR gel filtration cartridges (EdgeBio) spin columns and subsequently sequenced using the 3130 × l Genetic Analyzer from applied biosystems. The sequence was analyzed using microseq software (Applied Biosystems).
Bacterial culture
After collection, the biopsies were placed on a sterile sheet. This sheet and the tissue attached to it were cultured for bacteria using routine microbiological culture methods and identification techniques as previously described [14].
Results
The patient population consisted of patients from towns and settlements all over Greenland. All were born and raised in Greenland. Three patients had one parent born in Denmark and one in Greenland, while the remaining had parents of Greenlandic origin. The median age was 31 years (range 17–48 years). There were 12 females and 20 males.
When answering a questionnaire, most patients declared that the ear disease started in their childhood, predominantly under the age of seven, between the ages 4–6 years (12 patients) and 1–3 years (9 patients). Two patients debuted in infancy. Three patients debuted in the school years, between 7–16 years and only four patients debuted above the age of 16. Seventeen had bilateral disease and 15 had unilateral disease. Three patients had traumatic onset of the disease; one of these was >16 years at debut.
No patients had active suppuration at the time of surgery, but 18 patients had experienced discharge within the last 6 months prior to the operation. Twenty-seven patients had central perforations, of which 22 were subtotal pars tensa perforations, four total pars tensa perforations and one total perforation including both pars tensa and pars flaccida. Three had peripheral perforations, of which one was a subtotal pars tensa perforation and two total pars tensa perforations. In two patients, the perforation could not be identified the day before surgery, but both retraction and atrophy of the tympanic membrane were present. Both had experienced periodic discharge since childhood.
The appearance of the MEM was described as normal in 14 patients. Seven patients had granulation tissue and four had tympanosclerosis. The combination of the two was seen in two patients. One patient had both granulation tissue and metaplasia. Unspecified inflammation was found in three patients and the mucosa was not described in one case.
Hearing impairment in the study group varied between the speech reception threshold (SRT) 10 dB and >105 (deaf) dB with a median SRT of 35 dB.
A schematic overview of the bacterial findings is shown in Table 1.
PNA-FISH analysis showed morphological signs of biofilms in 15 out of 35 (43 %) middle ear biopsies, all originating from the MEM. In three cases, the results remained uncertain after re-evaluation. There was no sign of biofilm formation in the biopsy from the tympanic membrane or the additional biopsies from the mastoid, and the cholesteatoma. Monospecies biofilm with S. aureus was observed in six middle ear biopsies. Biofilms consisting of an unknown bacterial species, i.e., visible bacteria (Texas red filter), but not S. aureus (bacteria not visible with the FITC filter) were also seen in six biopsies. Confirmed polymicrobial biofilms, i.e., S. aureus and bacteria other than S. aureus were observed in three middle ear biopsies. Nine patients with biofilm in the MEM biopsies had experienced discharge within the last 6 months, while six patients had not. In five biopsies, the mucosa was described as normal and with granulation tissue in three cases. Tympanosclerosis was seen in four cases and the combination in one patient. Unspecific inflammation was found in two patients with biofilms.
In the control biopsies, there were signs of biofilms in 8 out of 23 biopsies (35 %). Monospecies S. aureus biofilms were the most frequently detected bacteria in the control biopsies (see Table 1). In six of the biofilm positive control specimens, the corresponding middle ear biopsy showed no sign of biofilm, an uncertain result or biofilms with different bacteria. For the remaining two positive control specimens, the corresponding middle ear biopsies showed biofilms containing the same bacterial species.
By means of PCR and 16s sequencing, we detected bacteria in 7 out of 20 (35 %) available middle ear biopsies, while bacteria were detected in 2 out of 10 (20 %) control samples. The seven positive biopsies in the middle ear originated from the MEM. In four of the middle ear biopsies, known otopathogenic bacteria, such as Turicella otidis and S. aureus were detected. Of these nine positive biopsies, representing both the MEM and controls, biofilms were demonstrated in only four by means of PNA-FISH.
Conventional culture showed bacterial growth in 18 out of 23 middle ear biopsies. Of these, S. aureus was found in nine samples and coagulase negative staphylococci (CNST) in eight. No association was found between culture and biofilm detection. The culture from the single cholesteatoma showed bacterial growth with S. aureus, but no biofilm was found. In the control material, bacterial growth was seen in seven of eight samples. The most common finding was CNST, which were found in six biopsies, while S. aureus was seen in two biopsies. Bacterial culture of both the middle ear and the control sample from the same patient was only possible in four patients, hence the correlation between control biopsies and middle ear biopsies could not be analyzed by culture.
Discussion
We hypothesize that mucosal biofilms in the middle ear can explain the recurrent and recalcitrant episodes of otorrhea in COM patients and thereby maintain the dry tympanic membrane perforation. The middle ear is considered a sterile compartment. Therefore, a chronic perforation of the tympanic membrane may serve as an entrance for bacteria. Bacterial biofilms in the middle ear in patients with dry tympanic membrane perforations are detectable by means of PCR and PNA-FISH techniques, while bacterial culture within biofilms is more uncertain. Almost all bacteria can be found as part of a biofilm. Some bacteria, like S. aureus, Pseudomonas aeruginosa, and Escherichia coli are more likely to be found in a biofilm community than others [15]. We consider PNA-FISH analysis to be the most accurate method for biofilm detection, where bacterial clusters can be demonstrated by microscopy using species-specific or universal eubacterial PNA-FISH probes. Furthermore, verification of the PNA-FISH results with PCR and 16s sequencing or culture are desirable to confirm the microscopic findings.
In this study, the PNA-FISH analysis showed morphological evidence of bacterial biofilms in 43 % of the middle ear biopsies. Both monospecies S. aureus biofilms and biofilms containing other bacteria were seen. All biopsies were obtained in a surgical setting, minimizing the risk of contamination. Since biofilms were found in dry ears without suppuration, this indicates that biofilms may be part of the pathogenesis in COM with recurrent episodes of CSOM.
Evidence of biofilms was also found in eight (35 %) of the control biopsies. The skin is not a sterile compartment of the body and the bacterial flora on the skin also may exist in biofilm communities [16]. S. aureus is a common pathogen in CSOM [17], but can also be found as a part of the normal flora on the skin. The skin (retroauricular, auricle, and entrance to the external auditory canal) was disinfected prior to surgery. Only a few studies exist on the effect of chlorhexidine and biofilms, and we do not know if the biofilms represent living bacteria [18]. We found no correlation between biofilms in the control specimen and biofilms in the middle ear biopsies. This indicates that biofilm findings in the control specimen and in the MEM are independent of each other and not a consequence of contamination. All biopsies were analyzed by means of PNA-FISH, since this method had the highest priority. Due to small biopsies, PCR and 16s sequencing was not possible in all samples. 16s sequencing detected bacteria in 7 out of 20 (35 %) middle ear biopsies, even though some of the biopsies weighed less than one milligram. There was no association between the bacterial findings in the PCR analysis and in the PNA-FISH analysis. Furthermore, the PCR analysis may be compromised by the low bacterial load in the biopsies.
Staphylococci were the most frequently cultured bacteria in both the middle ear biopsies and in the control samples, with S. aureus the most frequently seen in middle ear biopsies. Disinfection with chlorhexidine is considered as the state of the art, but cannot be used near the middle ear due to ototoxicity. Also, it does not always remove the resident bacterial flora of the skin, and disinfecting the external auditory canal is even more difficult [19, 20]. The existence of living bacteria in control specimens is possible and could explain our findings with bacterial culture. Culturing the correlating middle ear biopsy and control biopsy could only be performed in four patients. In these patients, no pattern was seen between the bacterial findings in the middle ear and the control sample, and as a consequence, we did not find any sign of contamination. Also, no convincing association was found between biofilms with PNA-FISH and bacterial culture. These results point towards real findings, even though the relatively low number of correlating samples does not completely rule out the possibility of contamination.
Previous studies have found evidence of bacterial biofilms in the middle ear of patients with CSOM [6, 7]. We therefore, hypothesize that bacterial colonization of the middle ear in COM patients may result in chronic recurrent episodes with otorrhea in these patients. This study presents evidence of biofilms in the middle ear, but where the bacteria originally migrated from is not known. However, migration through the external auditory canal or nasopharynx is the most plausible route. Another hypothesis is that other compartments in the upper airways, e.g., the adenoids, could serve as a reservoir for sessile bacteria causing otorrhea, as suggested for recurrent acute otitis media [21]. Bacteria causing recurrent suppuration in COM patients may therefore, also derive from biofilms at other locations.
The biopsies were collected almost 15 years before the present examinations and were stored at −80 °C. It is not currently described how bacterial biofilms survive or react under such storage conditions. The weaknesses of the present study are that the biopsies obtained represent a small random sample of a part of the MEM.
A novel study of experimental OME in a chinchilla model showed that biofilms in the middle ear are present together with normal mucosa [22]. We do not know how biofilms are distributed in the middle ear of humans and the possibility of biofilm formation in other parts of the MEM may also be expected. The small sample size and the heterogenic distribution of biofilms in chronic infections [23], may explain the relatively low correlation between PNA-FISH, 16s sequencing, and culture in this study. However, we demonstrate findings of bacteria in mucosal biofilms in not actively suppurating COM without evidence of any kind of contamination. We believe this is the first study to demonstrate this.
Conclusion
To our knowledge, this study is the first to demonstrate the presence of mucosal biofilms in middle ear biopsies from patients with COM with dry perforations by means of PNA-FISH. Although, the results could not be uniformly confirmed by PCR and 16s sequencing, the findings may indicate that biofilms are a part of the pathogenesis in recurrent episodes of ear discharge in COM. However, further investigations are necessary to understand the potential pathogenic mechanisms of biofilm presence in COM.
References
Burmølle M, Thomsen TR, Fazli M, Dige I, Christensen L, Homøe P, Tvede M, Nyvad B, Tolker-Nielsen T, Givskov M, Moser C, Kirketerp-Møller K, Johansen HK, Høiby N, Jensen PØ, Sørensen SJ, Bjarnsholt T (2010) Biofilms in chronic infections—a matter of opportunity—monospecies biofilms in multispecies infections. FEMS Immunol Med Microbiol 59:324–336
Macassey E, Dawes P (2008) Biofilms and their role in otorhinolaryngological disease. J Laryngol Otol 122:1273–1278
Rayner MG, Zhang Y, Gorry MC, Chen Y, Post JC, Ehrlich GD (1998) Evidence of bacterial metabolic activity in culture—negative otitis media with effusion. JAMA 279:296–299
Coates H (2004) Chronic suppurative otitis media without cholesteatoma. In: Bluestone CD, Alper CM, Mandel EM, Dohar JE, Casselbrant ML (eds) Advanced therapy of otitis media. B.C. Decker Inc, Ontario, pp 299–305
Hall-Stoodley L, Hu FZ, Gieseke A, Nistico L, Nguyen D, Hayes J, Forbes M, Greenberg DP, Dice B, Burrows A, Wackym PA, Stoodley P, Post JC, Ehrlich GD, Kerschner JE (2006) Direct detection of bacterial biofilms on the middle-ear mucosa of children with chronic otitis media. JAMA 296:202–211
Homøe P, Bjarnsholt T, Wessman M, Sørensen HC, Johansen HK (2009) Morphological evidence of biofilm formation in Greenlanders with chronic suppurative otitis media. Eur Arch Otorhinolaryngol 266:1533–1538
Lee MR, Pawlowski KS, Luong A, Furze AD, Roland PS (2009) Biofilm presence in humans with chronic suppurative otitis media. Otolaryngol Head Neck Surg 141:567–571
Saunders J, Murray M, Alleman A (2011) Biofilms in chronic suppurative otitis media and cholesteatoma: scanning electron microscopy findings. Am J Otolaryngol 32:32–37
Homøe P, Christensen RB, Bretlau P (1996) Prevalence of otitis media in a survey of 591 unselected Greenlandic children. Int J Pediatr Otorhinolaryngol 36:215–230
Jensen RG, Koch A, Homøe P (2012) Long-term tympanic membrane pathology dynamics and spontaneous healing in chronic suppurative otitis media. Pediatr Infect Dis J 31:139–144
Perry-O’Keefe H, Rigby S, Oliveira K, Sorensen D, Stender H, Coull J, Hyldig-Nielsen JJ (2001) Identification of indicator microorganisms using a standardized PNA FISH method. J Microbiol Methods 47:281–292
Oliveira K, Procop GW, Wilson D, Coull J, Stender H (2002) Rapid identification of Staphylococcus aureus directly from blood cultures by fluorescence in situ hybridization with peptide nucleic acid probes. J Clin Microbiol 40:247–251
Bjarnsholt T, Alhede M, Alhede M, Eickhardt-Sorensen SR, Moser C, Kuhl M, Jensen PO, Hoiby N (2013) The in vivo biofilm. Trends Microbiol 21:466–474
Høiby N, Frederiksen B (2000) Microbiology of Cystic fibrosis. In: Hodson Margaret E, Geddes Duncan M (eds) Cystic fibrosis. Hodder Arnold, London, pp 83–107
Römling U, Balsalobre C (2012) Biofilm infections, their resilience to therapy and innovative treatment strategies. J Intern Med 272:541–561
Vlassova N, Han A, Zenilman JM, James G, Lazarus GS (2011) New horizons for cutaneous microbiology: the role of biofilms in dermatological disease. Br J Dermatol 165:751–759
Verhoeff M, van DV, Rovers MM, Sanders EA, Schilder AG (2006) Chronic suppurative otitis media: a review. Int J Pediatr Otorhinolaryngol 70:1–12
Bonez PC, Dos Santos Alves CF, Dalmolin TV, Agertt VA, Mizdal CR, Flores VD, Marques JB, Santos RC, nraku de Campos MM (2013) Chlorhexidine activity against bacterial biofilms. Am J Infect Control
Guzel A, Ozekinci T, Ozkan U, Celik Y, Ceviz A, Belen D (2009) Evaluation of the skin flora after chlorhexidine and povidone—iodine preparation in neurosurgical practice. Surg Neurol 71:207–210
Cabenda SI, Peerbooms PG, van Asselt GJ, Feenstra L, van der BS (1988) Serous otitis media (SOM). A bacteriological study of the ear canal and the middle ear. Int J Pediatr Otorhinolaryngol 16:119–124
Nistico L, Kreft R, Gieseke A, Coticchia JM, Burrows A, Khampang P, Liu Y, Kerschner JE, Post JC, Lonergan S, Sampath R, Hu FZ, Ehrlich GD, Stoodley P, Hall-Stoodley L (2011) Adenoid reservoir for pathogenic biofilm bacteria. J Clin Microbiol 49:1411–1420
Ehrlich GD, Veeh R, Wang X, Costerton JW, Hayes JD, Hu FZ, Daigle BJ, Ehrlich MD, Post JC (2002) Mucosal biofilm formation on middle-ear mucosa in the chinchilla model of otitis media. JAMA 287:1710–1715
Kirketerp-Møller K, Jensen PO, Fazli M, Madsen KG, Pedersen J, Moser C, Tolker-Nielsen T, Hoiby N, Givskov M, Bjarnsholt T (2008) Distribution, organization, and ecology of bacteria in chronic wounds. J Clin Microbiol 46:2717–2722
Acknowledgments
Helle Krogh Johansen was supported by a clinical research stipend from the Novo Nordisk Foundation.
Conflict of interest
No conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wessman, M., Bjarnsholt, T., Eickhardt-Sørensen, S.R. et al. Mucosal biofilm detection in chronic otitis media: a study of middle ear biopsies from Greenlandic patients. Eur Arch Otorhinolaryngol 272, 1079–1085 (2015). https://doi.org/10.1007/s00405-014-2886-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-014-2886-9