
Abstract
Purpose
Surface electromyography (sEMG) using intravaginal probes is of widespread use for assessing pelvic floor muscles (PFM) activity in women. Although considered as a reliable method, its validity has been called into question due to the presence of a phenomenon called crosstalk. Crosstalk is described as the recording of sEMG activity originating from neighboring muscles rather than coming exclusively from the muscles being investigated. The purpose of this review was to provide an overview of existing literature about crosstalk during intravaginal surface electromyographic recordings.
Methods
A scoping review was performed according to the Arksey and O’Malley framework. An electronic search was conducted on six relevant databases. Additionally, authors were directly contacted to identify grey literature. Data extraction consisted of descriptive numeric analysis as well as thematic analysis, which were conducted by two independent reviewers.
Results
Forty-nine references written by 34 authors coming from 13 different countries constitute the body of evidence of the present review. Eight main themes have been identified through the thematic analysis. The included material varies greatly in terms of methodology, approach to the crosstalk problem and depth of analysis.
Conclusions
A gap in knowledge affecting the validity of the current sEMG investigation methods was identified. Literature addressing the crosstalk problem is scarce and often flawed. Definitive conclusions are regularly drawn from an insufficient basis of evidence. Further research is, therefore, deeply necessary, although it remains unclear whether this issue can be solved at all with current technology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surface electromyography (sEMG) using intravaginal probes is widely used and considered a reliable method of assessing pelvic floor muscles (PFM) activity in healthy women [1]. However, some authors have questioned its validity, suspecting the presence of crosstalk [2, 3].
The crosstalk phenomenon is described as the detection by the EMG of a signal originating from a neighboring muscle rather than exclusively from the muscle under investigation [4]. It is mostly due to volume conduction of electrical activity [5]. Such a contamination is problematic since it may lead to erroneous interpretation of the signal information [6]. Crosstalk has been extensively investigated in some muscle groups including the quadriceps [7] and the gastrocnemii [8]. Byrne et al. [7] concluded that crosstalk from the vastii did indeed contaminate sEMG recordings of the rectus femoris, while Solomonow et al. [8] were able to estimate that crosstalk accounts for 4–5% of the recorded signal of the gastrocnemii.
In the PFM research field, crosstalk has become a topic of growing interest in the discussion sections of recently published studies [9, 10], with great variability in the manner and the depth in which this matter is treated. Very few authors have attempted to evaluate PFM crosstalk as the main focus of their study [4, 11]. Possible explanations for this limited interest include the particular challenges posed by the local anatomical characteristics, as well as the related technical and methodological difficulties in designing an appropriate experiment [4]. Another barrier is the relative taboo still surrounding this intimate body part. As a consequence, there appears to be no consensus between researchers concerning the extent of this problem or on its impact on research findings. Some authors consider crosstalk to be negligible [12, 13], while others view it as a real concern [4, 11] because high levels of crosstalk cast doubt on the validity of experimental studies investigating the effectiveness of PFM interventions.
Based on these observations and to provide an overview of the current state of knowledge, it was decided to undertake a scoping review. According to Levac et al. [14], scoping reviews are powerful tools for synthesizing health research evidence. As an exploratory project, a scoping review allows systematic mapping of the available literature, identifying key concepts and gaps in the research, thus pointing out where further primary research is necessary. Moreover, it is particularly indicated when literature is scarce or diverse [14], as in the present project.
The purpose of this review was to provide an overview of existing literature about crosstalk in sEMG PFM measurements. More specifically, the objectives were to (1) conduct a systematic search of the published and grey literature on the topic, (2) map the characteristics of the material retrieved, (3) summarize evidence regarding the aspects of crosstalk discussed in the literature, and (4) determine whether and (if so) how further research should be conducted.
Methods
Methodology
The research team included two reviewers trained as physical therapists and acquainted with PFM research, as well as a supervisor with expertise in sport science.
The methodology for this scoping review was based on the framework outlined by Arksey and O’Malley [15], also considering subsequent recommendations formulated by Levac et al. [14]. This framework involves five successive key phases, which were strictly followed.
As advocated by Levac et al. [14], the fifth step, the “results presentation”, consists of both descriptive numeric and qualitative analyses. A thematic analysis approach was used for qualitative assessment of the body of evidence. Braun and Clarke [16] defined thematic analysis as a method allowing identification, analysis and reporting of patterns (themes) within data. To this end, the six recommended steps were completed successively. According to Caelli et al. [17], this qualitative study, as a thematic analysis, falls into the category of “generic approaches”. As such, it does not follow the guiding set of philosophical assumptions characteristic of traditional qualitative approaches. Primary physical therapy research, and, therefore, the articles included in the present review, typically follows a realistic ontology and a positivist epistemology, defined by Bourgeault et al. [18] as the clear assumption that “there is a single reality which can be observed directly”. The present qualitative study touches upon pragmatic epistemology, however, since we acknowledge that “phenomena do operate independently of our ideas, but [that] we must apprehend these phenomena through our [own] ideas” [18]. It was conducted with an inductive, descriptive methodology. Furthermore, because this inductive approach was chosen, data extraction and analysis were not based on a set of a priori defined themes; instead, important and recurrent themes were identified in the body of evidence [19].
Research question
This review was driven by the question: “How is crosstalk taken into consideration in published and unpublished studies evaluating pelvic floor muscles (PFM) using surface electromyography (sEMG) in women?”.
Data sources and search strategy
Searches were performed to query six relevant electronic databases: MEDLINE/Pubmed, EMBASE, CINAHL, PEDro, Cochrane and Google Scholar. These searches took place from week 42 of 2015 until week 46 of 2015. To ensure comprehensiveness, no limits were initially set in terms of date, language or type of material.
At the outset, very specific keywords were combined: (PFM) OR (pelvic floor muscle*) AND (crosstalk/cross-talk/cross talk). Thereafter, search terms were broadened to (EMG) OR (electromyography) AND (PFM/pelvic floor muscle*). This procedure generated very comprehensive results, therefore limiting the probability of missing relevant publications. Each search was adapted to the specific requirements of each database. Subsequently, the reference lists of included articles were screened for further potentially relevant articles. The International Continence Society (ICS) and the International Urogynecological Association (IUGA) were identified as relevant organizations. The meeting abstracts from the years 1999 through 2015 for the ICS conferences and 2003/2005–2015 for the IUGA conferences were carefully checked.
As a last step in finalizing the literature search, personal contact with 18 authors active in the field was established via email, with the aim of identifying further unpublished work on the topic (such as bachelor’s, master’s, doctoral or postdoctoral theses). A friendly reminder was sent 2 weeks later in cases of non-response. Six researchers answered, and one additional conference proceeding was retrieved, thanks to these suggestions.
Eligibility criteria
Article inclusion was based on inclusion of the word “crosstalk”, or any of its abovementioned spelling variations, in the full-text versions of all articles with titles that suggested the use of sEMG for PFM activity evaluation in women. When electronic search could not be performed, articles were read in their entirety. Every effort was made to retrieve the full texts of all articles that could not be clearly excluded based upon their title. For articles which could not be obtained through the reviewers’ institutional library, authors or journals were directly contacted.
In accordance with the inclusion criteria, articles in which authors did not use sEMG as a method of investigation and justified this choice by emphasizing its susceptibility to crosstalk were excluded as well.
Data characterization
Descriptive numeric analysis
A spreadsheet was created using Microsoft Excel 2008 to display the relevant characteristics of the studies included in the review. To ensure consistency, a standardized framework was used to extract information.
Thematic analysis
The two reviewers (NF and IK) conducted the thematic analysis independently. All citations about crosstalk (including references) were collected into a table using Microsoft Word 2008. Simultaneously, codes were assigned to each excerpt. When different codes were possible for a given citation, the reviewer made her decision based on the aspect that she perceived as dominant.
After an initial test including the first five articles of the review, both reviewers met to exchange experiences, check the preliminary findings and ensure that the procedure led to satisfactory results. After this meeting, data from the totality of the articles were extracted following the same procedure. Another meeting took place to compare the final results, find consensus on the codes, identify themes and finally define them. Themes were then re-organized, to allow a logical flow to emerge between them. As for the other steps, this stage happened through consensus between the two primary researchers.
Data extraction was systematically conducted from the first to the last reference. Hence, the concept of saturation was not considered. This procedure ensured comprehensiveness but as a consequence, similar information was collected repeatedly.
Results
Search and selection of studies
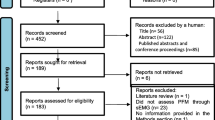
The selection process is displayed in a flowchart adapted from the PRISMA guidelines in Fig. 1 [20]. One article was excluded on the grounds that an ambiguous online translation was obtained from the original Icelandic-language text. Only one conference abstract was found through screening meeting abstracts; however, it was already a part of the included references. This is not surprising since the search strategy was designed to generate exhaustive results. The 49 remaining articles were further analyzed and constitute the body of evidence of this scoping review.

Flowchart of the literature search methodology [20]
Descriptive numeric analysis: general characteristics of the included material
The oldest included article was published in 2001, whereas the most recent dated from 2015. In the majority of cases (61%: 30/49), the mention of crosstalk was only incidental, i.e., limited to one or two sentences on the topic.
Overall, 34 different first authors contributed to the topic of interest, with 8 of them writing more than one included reference. However, additionally taking into consideration the last authors, it is noteworthy to point out that many references are the result of the work produced by only a few research teams that have been extremely active in this field. This is highlighted in Table 1.
Details about types of documents, study designs, localization of the statements regarding crosstalk and types of intravaginal probes are shown in Table 2.
Themes identified through thematic analysis
Results of the thematic analysis are presented in a complementary fashion in the text and in Table 3, which presents the different themes and subthemes identified, providing direct citations as illustrative examples from the body of evidence.
-
1.
Definition of the concept
-
1a. Description
-
1b. Contamination (muscles involved)
-
1c. Rationale for recording crosstalk
-
Regarding the reasons underlying crosstalk recording, current PFM literature is somewhat scarce [2].
-
-
-
2.
Current research and evidence
-
3.
Influencing factors
-
3a. Intravaginal probes
-
3b. Electrode configuration
-
3c. Electrode size and location
-
3d. Other factors
-
Additional relevant aspects to consider include temperature and humidity [2]. However, these factors are quite difficult to control.
-
-
-
4.
Investigation/identification
-
4a. Crosstalk present: quantification/assessment
-
Only two researchers (Madill [11, 27] and Keshwani [4, 10]) explicitly attempted to bring to light the presence of crosstalk in their recordings. A few others conducted separate sub-studies including very few subjects (Hodges et al. [13], Sapsford and Hodges [28], Smith et al. [29], Sjödahl et al. [30]). Madill [11, 27] compared increasing PFM EMG activity amplitude with increasing vaginal pressure amplitude during isolated and non-isolated PFM contractions. Besides the PFM, she examined the transversus abdominis, the rectus abdominis, the gluteal and hip adductor muscles. When intravaginal pressure did not increase simultaneously with rises in EMG amplitude, crosstalk was deemed present. Madill [11, 27] found this to happen in two of eight subjects, being the first researcher to introduce the possibility of individual variability in crosstalk recordings. Keshwani and McLean [10] additionally draw attention to the influence of contraction intensities of the hip muscles, as the risk for crosstalk has been shown to increase concomitantly with higher intensity levels. In a further publication [4], Keshwani and McLean analyzed PFM EMG activation amplitude using Root Mean Square (RMS) during hip adductor and hip external rotator ipsilateral muscle contractions. They compared a newly developed suction head intravaginal probe with the commercially available Femiscan, concluding that both intravaginal probes were susceptible to recording crosstalk at higher levels of contraction intensities, i.e., during contractions exceeding 50% of maximal voluntary contraction (MVC). However, they were not able to firmly determine if both probes were recording crosstalk, or if this increase in activity was due to co-activation (see also point 5).
-
-
4b. Reasons for crosstalk exclusion
-
Sjödahl et al. (unpublished; in Sjödahl et al. [30]) have conducted a separate pilot study to investigate PFM crosstalk from the abdominal and hip adductor musculatures. They concluded that the risk for crosstalk is minimal. Unfortunately, despite our best efforts, we could not access this publication.
-
Hodges et al. [13] examined crosstalk by simultaneously recording vaginal PFM activity levels using a Periform probe and activity of the gluteus maximus, hip adductors, medial hamstrings, obliquus internus abdominis and rectus femoris muscles using surface EMG electrodes. The study protocol involved one subject during the performance of one low-intensity arm movement task. Under these circumstances, no crosstalk from the hip or abdominal musculature has been observed. Smith et al. [29] reported about a very similar protocol performed on one continent woman, coming to the same conclusion.
-
Keshwani [26], in her Master’s thesis investigating the re-test reliability and validity of a novel suction electrode in comparison to the Femiscan, was able to conclude that crosstalk from the deep abdominal muscles could be excluded.
-
Sapsford and Hodges [28] used a Periform vaginal probe and sEMG electrodes over the hip adductors and the gluteus maximus. They visually compared the onset times of muscular activity and concluded that crosstalk was unlikely, since they identified distinct activity patterns.
-
-
-
5.
Synergistic activation
-
A major issue in current research is being able to make a distinction between crosstalk and synergistic activation (or co-activation) of neighboring muscles. As a matter of fact, the PFM might be activated to assist in pelvic stabilization during resisted tasks, and probably work in synergy with other muscles of the pelvic girdle [2]. However, as of today, researchers have not been able to develop a methodology to differentiate between them.
-
-
6.
Limitations of sEMG (with regards to crosstalk)
-
6a. General
-
6b. Psychometric properties (validity and reliability)
-
-
7.
Measures taken to avoid crosstalk
-
Some authors decided to make adjustments or take additional precautionary measures in order to minimize the potential for crosstalk. These preventive actions included: visual inspection to identify simultaneous hip adductor or gluteus muscle contraction instead of isolated PFM contraction [34–36]; use of a strap in the lithotomic position to support legs and prevent contraction of the hip internal rotators or adductors [24]; completion of additional pilot studies to assess the problem [13, 28–30] and teaching of a correct isolated PFM contraction and screening for the ability to perform it before study enrollment [35].
-
-
8.
Suggestions for future work
-
Many aspects of the problem have been overlooked or could not be taken into consideration so far in the literature. Future work should especially focus on the following points:
-
Use electrodes large enough to record a reasonable amount of activity, but small enough to minimize crosstalk [37].
-
Use a bipolar configuration combined with a differential amplifier, and provide extensive details about signal processing methods [2].
-
Minimize inter-electrode spacing [24].
-
Favor probes providing double differential electrode configuration [26].
-
Treat results from the right and the left sides of the PFM separately, differentiate between contraction intensity levels (% of MVC) and consider hip external rotators in the evaluation protocol [26].
-
Teach correct isolated PFM contraction beforehand, and check for accessory muscle contraction or movement at the hip joint [21].
-
-
Discussion
Although the first report of using EMG to describe female PFM activity goes back to 1968 [38] (cited in [27]), it must be recognized that this method still has potential for improvement with respect to crosstalk considerations. The inconsistency in spelling, with different variants (“crosstalk”/“cross-talk”/“cross talk”) sometimes encountered in a single article, is a prime example of the vagueness surrounding the topic. Another worrisome characteristic of the current literature is that it mainly relies on subjective, qualitative inspection of raw data [13, 30], whereas scientific rigor would call for objective methods including statistical analysis. The present scoping review sheds light on the contrasting opinions held by researchers. It is interesting to notice that often, authors who state their confidence in the ability of intravaginal probes to record PFM activity without capturing crosstalk [22, 30, 39–42] make reference to only two studies from the same research group [13, 29], which present the major drawback of being underpowered. They both included only one healthy subject for the crosstalk investigation. Moreover, on at least one occasion, a researcher arguing that the intravaginal probe used in his study had been previously tested and was not prone to crosstalk based his statement on three references [22]. Interestingly, a brief verification into the source articles revealed that none of the three publications in fact investigated this particular type of intravaginal probe. Such a basis is insufficient to draw definitive conclusions on this complex matter. On the other hand, authors arguing that current intravaginal probes are subject to crosstalk deserve credit for basing their opinions on more comprehensive research, describing issues and actively looking for alternatives (Keshwani [4, 26], Madill [11, 27], McLean [43]). Since they could not be satisfied with the commercially available probes, some authors decided to create their own prototypes [43–45]. To date, those prototypes have not been commercialized.
Limitations
Overall, the high proportion of references making incidental mentions of the crosstalk phenomenon is regrettable: many authors did not look thoroughly into the problem, instead repeatedly using similar warning statements.
One author, who claimed to have conducted a pilot study with the express purpose of investigating the crosstalk problem, never responded to our request for the text of this study. This unpublished article might have brought additional insights into the topic being discussed.
Scoping reviews by definition are to be conducted without performing any kind of quality assessment of the included material. This guarantees breadth of coverage, but a lack of methodological rigor in the primary material suggests that readers ought to exercise caution in the interpretation and generalization of the present findings.
Suggestions for future research
The challenges faced in designing the perfect intravaginal probe while considering crosstalk issues, among others, are numerous and diverse. Not only do the deep PFM lie in an intimate and sensitive area hidden within the pelvic cavity, but also the moist environment of the vaginal canal precludes the use of traditional adhesive electrodes [2, 26]. Hormonal changes influencing vaginal humidity and varying temperature may also be sources of signal alteration [10]. Individual components, with the presence of crosstalk being identified in some subjects but not in others, cannot be excluded [27]. The ability to volitionally contract the PFM is far from straightforward to many healthy individuals [2]. Furthermore, obtaining a true maximal voluntary contraction is crucial in any sEMG activity recording, but for the PFM any potential pain or fear of pain, discomfort, anxiety or feeling that the probe may slip out further complicates this requirement [2]. Moreover, the very presence of the vaginal probe may alter PFM performance by modifying their contractile properties, although Auchincloss and McLean showed that it probably does not have such a significant influence [46]. The adaptability of the intravaginal probe to each subject’s particular anatomical characteristics and gynecological/obstetrical history may play a key role, though an underappreciated one. Indeed, the two most commonly used, commercially available intravaginal probes (the Periform and the Femiscan) surprisingly only come in one standard size despite the fact that Voorham-Van der Zalm et al. [47], back in 2006, were able to show using ultrasound that probe positioning varied considerably among multiparous women. This positioning problem is further complicated by the observation that the PFM move cranially and ventrally while they contract [26]. Additionally, the fact that most probes were originally designed for biofeedback therapy purposes in lithotomic position makes them susceptible to motion artifacts and therefore inadequate for use while standing, during functional tasks such as coughing, or during whole-body movements accompanied by reflexive activity of the PFM, such as running and jumping. Another important consideration is the sometimes forgotten characteristic that both sides of the PFM are different muscles with distinctive innervations, and as such, an adequate intravaginal probe should be able to distinguish between right and left sides [2]. Ignoring this would provide an erroneous, nonspecific representation of the general muscle activity around the vagina [26]. Double differential configuration, as advocated by the SENIAM group (Surface Electromyography for the non-invasive assessment of muscles), as well as small electrode surfaces located close together, are additional requirements to be fulfilled to minimize crosstalk [48]. Other issues such as the distinction between synergistic activations or substitutions and crosstalk imply a high degree of methodological complexity in the elaboration of an adequate research protocol. This will require interdisciplinary collaboration among the engineering sciences, mathematics, and so on.
Alternatives to intravaginal probes include the use of adhesive electrodes over the peri-neal area or the insertion of fine wire electrodes. Adhesive electrodes have been shown to account for technical problems related to any possible shift, and also have low subject acceptability [31]. Fine wire electrodes have been chosen for crosstalk investigation in other skeletal muscles: Byrne et al. [7] chose to compare fine wire and sEMG recordings of the rectus femoris and vastus lateralis during isometric contractions consisting of knee extensions and hip flexions. They concluded that crosstalk contamination occurred from the vastus lateralis and suggested utilizing fine wire electrodes to ensure accurate EMG recordings [7]. However, fine wire EMG is particularly invasive, which presages difficulties in participant recruitment. Additionally, it appears not to provide valid results for PFM evaluation since it records only from a very small, localized region (limited to one or two motor units), therefore failing to reflect the global muscle activity [10]. For these reasons, neither adhesive nor fine wire electrodes can be considered valid options. Therefore, further research should focus on testing and establishing a valid reference intravaginal probe. In addition, improvements regarding the electrodes, the measuring amplifiers and the development of adequate mathematical methodologies, such as Wavelet Transforms or Empirical Mode Decomposition [49] to purify the signal from crosstalk contaminations are appropriate leads to pursue in the future. The gain of a non-stationary wavelet approach is to provide simultaneous information in the domains of time, frequency and magnitude. Therefore, areas where the muscles co-contract can be distinguished. The areas where the activity of inividual muscles predominates indicate the maximal expected amount of crosstalk [50]. The Empirical Mode Decomposition (EMD) is a method for breaking down signals into various components and comparable with Fourier transform and Wavelet transform. Without leaving the time domain, EMD is adaptive and can be applied to non-linear and non-stationary time series, i.e., derived from ECG or EMG. Together with subsequent independent component analysis [51] it can be used to purify EMG from ECG artifacts [51], electrical muscle stimulation signals [52] or crosstalk [53]. However, from a global perspective, an essential and somewhat daunting question remains open: even if a perfectly optimized intravaginal probe was available, since some highly crosstalk-susceptible muscles—such as the hip external rotators—are not accessible to direct sEMG measurements, it might be impossible to detect and remove their influence using current technology.
Conclusions
This scoping review identified a gap in scientific knowledge regarding the validity of the diverse intravaginal probes currently used in research. Literature addressing the crosstalk problem is scarce and oftentimes flawed: studies in this area suffer from having a small number of subjects involved in the evaluation procedure. Further deficiencies include lack of details regarding the protocol, making subsequent independent interpretation difficult, paucity of “reference publications” on the matter and failure to acknowledge and determine the influence of crosstalk from hip external rotators. Considering all these shortcomings, further research is deeply necessary to improve the validity of applied research assessing and comparing the effects of different physical therapy regimens and to deepen the understanding of PFM activation patterns under physiological and pathological conditions. To achieve this goal, the processing of a valid intravaginal probe is required and the method to eliminate crosstalk has to be improved. Nevertheless, it remains unclear to what extent technological tools are sufficient to detect and eliminate crosstalk signal contaminations in future. However, the leading question persists whether this issue can be solved at all with current technology.
References
Luginbuehl H, Greter C, Gruenenfelder D, Baeyens JP, Kuhn A, Radlinger L (2013) Intra-session test-retest reliability of pelvic floor muscle electromyography during running. Int Urogynecol J 24(9):1515–1522. doi:10.1007/s00192-012-2034-2
Brown CC (2007) Reliability of electromyography detection systems for the pelvic floor muscles. Master’s thesis. Queen’s University, Kingston
Grape HH, Dedering A, Jonasson AF (2009) Retest reliability of surface electromyography on the pelvic floor muscles. Neurourol Urodyn 28(5):395–399. doi:10.1002/nau.20648
Keshwani N, McLean L (2013) A differential suction electrode for recording electromyographic activity from the pelvic floor muscles: crosstalk evaluation. J Electromyogr Kinesiol 23(2):311–318. doi:10.1016/j.jelekin.2012.10.016
Turker KS (1993) Electromyography: some methodological problems and issues. Phys Ther 73(10):698–710
De Luca CJ (1997) The use of surface electromyography in biomechanics. J Appl Biomech 13:135–163
Byrne CA, Lyons GM, Donnelly AE, O’Keeffe DT, Hermens H, Nene A (2005) Rectus femoris surface myoelectric signal cross-talk during static contractions. J Electromyogr Kinesiol 15(6):564–575. doi:10.1016/j.jelekin.2005.03.002
Solomonow M, Baratta R, Bernardi M, Zhou B, Lu Y, Zhu M, Acierno S (1994) Surface and wire EMG crosstalk in neighbouring muscles. J Electromyogr Kinesiol 4(3):131–142. doi:10.1016/1050-6411(94)90014-0
Luginbuehl H, Naeff R, Zahnd A, Baeyens JP, Kuhn A, Radlinger L (2016) Pelvic floor muscle electromyography during different running speeds: an exploratory and reliability study. Arch Gynecol Obstet 293(1):117–124. doi:10.1007/s00404-015-3816-9
Keshwani N, McLean L (2015) State of the art review: Intravaginal probes for recording electromyography from the pelvic floor muscles. Neurourol Urodyn 34(2):104–112. doi:10.1002/nau.22529
Madill S, McLean L (2004) Electromyographic crosstalk and muscle substitutions in the measurement of pelvic floor muscle activation. In: Biannual conference of the international society for electrophysiology and kinesiology, Boston, 2004
Halski T, Ptaszkowski K, Slupska L, Dymarek R (2013) The evaluation of bioelectrical activity of pelvic floor muscles depending on probe location: a pilot study. BioMed Res Int 2013:238312. doi:10.1155/2013/238312
Hodges PW, Sapsford R, Pengel LH (2007) Postural and respiratory functions of the pelvic floor muscles. Neurourol Urodyn 26(3):362–371. doi:10.1002/nau.20232
Levac D, Colquhoun H, O’Brien KK (2010) Scoping studies: advancing the methodology. IS 5:69. doi:10.1186/1748-5908-5-69
Arksey H, O’Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8(1):19–32. doi:10.1080/1364557032000119616
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101. doi:10.1191/1478088706qp063oa
Caelli K, Ray L, Mill J (2003) “Clear as mud”: toward greater clarity in generic qualitative research. Int J Qual Methods 2(2):1–24
Bourgeault I, Dingwall R, de Vries R (2010) The SAGE Handbook of qualitative methods in health research. SAGE Publications, London
Pope C, Popay J (2007) Synthesizing qualitative and quantitative health evidence: a guide to methods. Open University Press, McGraw Hill Education, Berkshire
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. doi:10.1371/journal.pmed.1000097
Madill SJ (2009) Differences in pelvic floor muscle activation and functional output between women with and without stress urinary incontinence. PhD Thesis. Queen’s University, Kingston
Halski T, Slupska L, Dymarek R, Bartnicki J, Halska U, Krol A, Paprocka-Borowicz M, Dembowski J, Zdrojowy R, Ptaszkowski K (2014) Evaluation of bioelectrical activity of pelvic floor muscles and synergistic muscles depending on orientation of pelvis in menopausal women with symptoms of stress urinary incontinence: a preliminary observational study. BioMed Res Int 2014:274938. doi:10.1155/2014/274938
Auchincloss CC, McLean L (2009) The reliability of surface EMG recorded from the pelvic floor muscles. J Neurosci Methods 182(1):85–96. doi:10.1016/j.jneumeth.2009.05.027
Gentilcore-Saulnier E (2008) Deep and superficial pelvic floor muscle responses to a pain stimulus in vestibulodynia. Master’s Thesis. Queen’s University, Kingston
Keshwani N, McLean L (2011) Surface Electromyography of the Pelvic Floor Musculature: Reliability and Validity of a Novel Electrode Design. In: World Physical Therapy 2011, Amsterdam, Netherlands
Keshwani N (2011) Surface electromyography of the pelvic floor musculature: reliability and validity of a novel electrode design. Master’s Thesis. Queen’s University, Kingston
Madill SJ (2004) Synergistic pelvic floor and abdominal muscles contributions to rises in intravaginal pressure in urinary continent women. Queen’s University, Kingston
Sapsford RR, Hodges PW (2001) Contraction of the pelvic floor muscles during abdominal maneuvers. Arch Phys Med Rehabil 82(8):1081–1088. doi:10.1053/apmr.2001.24297
Smith MD, Coppieters MW, Hodges PW (2007) Postural response of the pelvic floor and abdominal muscles in women with and without incontinence. Neurourol Urodyn 26(3):377–385. doi:10.1002/nau.20336
Sjödahl J, Kvist J, Gutke A, Oberg B (2009) The postural response of the pelvic floor muscles during limb movements: a methodological electromyography study in parous women without lumbopelvic pain. Clin Biomech 24(2):183–189. doi:10.1016/j.clinbiomech.2008.11.004
Crotty K, Bartram CI, Pitkin J, Cairns MC, Taylor PC, Dorey G, Chatoor D (2011) Investigation of optimal cues to instruction for pelvic floor muscle contraction: a pilot study using 2D ultrasound imaging in pre-menopausal, nulliparous, continent women. Neurourol Urodyn 30(8):1620–1626. doi:10.1002/nau.21083
Bo K (2004) Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct 15(2):76–84. doi:10.1007/s00192-004-1125-0
Naess I, Bo K (2015) Pelvic floor muscle function in women with provoked vestibulodynia and asymptomatic controls. Int Urogynecol J 26(10):1467–1473. doi:10.1007/s00192-015-2660-6
Batista RL, Franco MM, Naldoni LM, Duarte G, Oliveira AS, Ferreira CH (2011) Biofeedback and the electromyographic activity of pelvic floor muscles in pregnant women. Revista Brasileira de Fisioterapia 15(5):386–392
Madill SJ, Harvey MA, McLean L (2009) Women with SUI demonstrate motor control differences during voluntary pelvic floor muscle contractions. Int Urogynecol J Pelvic Floor Dysfunct 20(4):447–459. doi:10.1007/s00192-008-0800-y
Vassimon FI, Ferreira CH, Martins WP, Ferriani RA, de Andrade Batista RL, Bo K (2016) Surface electromyography and ultrasound evaluation of pelvic floor muscles in hyperandrogenic women. Int Urogynecol J 27(4):587–591. doi:10.1007/s00192-015-2865-8
Botelho S, Pereira LC, Marques J, Lanza AH, Amorim CF, Palma P, Riccetto C (2013) Is there correlation between electromyography and digital palpation as means of measuring pelvic floor muscle contractility in nulliparous, pregnant, and postpartum women? Neurourol Urodyn 32(5):420–423. doi:10.1002/nau.22321
Hutch JA, Elliott HW (1968) Electromyographic study of electrical activity in the paraurethral muscles prior to and during voiding. J Urol 99(6):759–765
Capson AC, Nashed J, McLean L (2011) The role of lumbopelvic posture in pelvic floor muscle activation in continent women. J Electromyogr Kinesiol 21(1):166–177. doi:10.1016/j.jelekin.2010.07.017
Smith MD, Coppieters MW, Hodges PW (2007) Postural activity of the pelvic floor muscles is delayed during rapid arm movements in women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 18(8):901–911. doi:10.1007/s00192-006-0259-7
Junginger B, Baessler K, Sapsford R, Hodges PW (2010) Effect of abdominal and pelvic floor tasks on muscle activity, abdominal pressure and bladder neck. Int Urogynecol J 21(1):69–77. doi:10.1007/s00192-009-0981-z
Sapsford RR, Richardson CA, Maher CF, Hodges PW (2008) Pelvic floor muscle activity in different sitting postures in continent and incontinent women. Arch Phys Med Rehabil 89(9):1741–1747. doi:10.1016/j.apmr.2008.01.029
McLean L, Keshwani N (2011) Development and testing of a novel electrode for recording electromyography data from the pelvic floor muscles. In: 41st Annual Meeting of the International Continence Society, ICS, Glasgow, United Kingdom, pp 918–919
Voorham-van der Zalm PJ, Voorham JC, van den Bos TW, Ouwerkerk TJ, Putter H, Wasser MN, Webb A, DeRuiter MC, Pelger RC (2013) Reliability and differentiation of pelvic floor muscle electromyography measurements in healthy volunteers using a new device: the Multiple Array Probe Leiden (MAPLe). Neurourol Urodyn 32(4):341–348. doi:10.1002/nau.22311
Keshwani N, McLean L (2012) Development of a differential suction electrode for improved intravaginal recordings of pelvic floor muscle activity: reliability and motion artifact assessment. Neurourol Urodyn 31(8):1272–1278. doi:10.1002/nau.22253
Auchincloss C, McLean L (2012) Does the presence of a vaginal probe alter pelvic floor muscle activation in young, continent women? J Electromyogr Kinesiol 22(6):1003–1009. doi:10.1016/j.jelekin.2012.06.006
Voorham-van der Zalm PJ, Pelger RC, van Heeswijk-Faase IC, Elzevier HW, Ouwerkerk TJ, Verhoef J, Nijeholt GA (2006) Placement of probes in electrostimulation and biofeedback training in pelvic floor dysfunction. Acta Obstet Gynecol Scand 85(7):850–855. doi:10.1080/00016340500442456
Recommendations for sEMG (2016) http://www.seniam.org. Accessed March 2016
Chowdhury RH, Reaz MB, Ali MA, Bakar AA, Chellappan K, Chang TG (2013) Surface electromyography signal processing and classification techniques. Sensors 13(9):12431–12466. doi:10.3390/s130912431
von Tscharner V, Valderrabano V (2010) Classification of multi muscle activation patterns of osteoarthritis patients during level walking. J Electromyogr Kinesiol 20(4):676–683
Abbaspour S, Lindén M, Gholamhosseini H (2015) ECG Artifact removal from surface EMG signal using an automated method based on wavelet-ICA. Stud Health Technol Inform 211:91–97
Stratton K, Faghri PD (2016) Electrically and hybrid-induced muscle activations: effects of muscle size and fiber type. Eur J Transl Myol 26(3):6163
Hyvarinen A, Oja E (2000) Independent component analysis: algorithms and applications. Neural Netw 13(4–5):411–430
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This aricle does not contain any studies with human participants performed by any of the authors. Therefore, for this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Flury, N., Koenig, I. & Radlinger, L. Crosstalk considerations in studies evaluating pelvic floor muscles using surface electromyography in women: a scoping review. Arch Gynecol Obstet 295, 799–809 (2017). https://doi.org/10.1007/s00404-017-4300-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-017-4300-5