
Abstract
Background
Radiofrequency (RF) catheter ablation guided by electroanatomic mapping systems is an effective therapy for atrial fibrillation. However, it may be affected by respiration movements. The aim of this study was to determine the impact of respiratory gating on procedural parameters in patients undergoing catheter ablation of atrial fibrillation (AF).
Methods and results
One-hundred forty consecutive patients undergoing pulmonary vein isolation were admitted to study. Respiratory gating module (AccuResp algorithm, Carto3, Biosense Webster) was enabled in 70 patients and disabled in 70 patients during procedures. Successful pulmonary vein isolation and sinus rhythm were obtained in all patients. A significant reduction in total procedure times [median 77, interquartile range (IQR 66–95) min vs median 82 (IQR 72–104) min, p < 0.05] and fluoroscopy times [median 14 (IQR 9–17) min vs median 16 (IQR 12–22) min, p < 0.05] were observed in the respiratory gated group. Although ablation times (duration between the first and last ablation) were significantly shorter in respiratory gated group [median 37 (IQR 32–53) min vs median 48 (IQR 39–65) min, p < 0.05], total RF application durations were not different between two groups [median 1,554 (IQR 1,213–2,196) s vs median 1,802 (IQR 1,344–2,448) s, p = 0.11]. Difference in electroanatomical map reconstruction times was not significant [median 14 (IQR 12–16) min in gated group vs median 13 (IQR 10–18) min in nongated group, p = 0.19].
Conclusion
Respiratory gating significantly improves fluoroscopy and ablation times during electroanatomic mapping guided AF ablation. Respiratory gated maps may provide uninterrupted continuous ablation applications. Furthermore, using automatic respiratory gating module does not prolong mapping times.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Radiofrequency (RF) catheter ablation is an effective therapy for atrial fibrillation (AF) and electroanatomic mapping (EAM) systems play important role on ablation procedures [1–5]. Unfortunately, benefits of these tools are limited by biological factors. Significant changes in left atrium (LA) and pulmonary vein (PV) anatomy due to respiration have been reported [6, 7]. Beinart et al. [8] recently demonstrated favorable effects of respiratory gating on electroanatomical map accuracy. Respiratory compensated electroanatomical maps showed better correlation with pre-acquired computed tomography (CT) and magnetic resonance (MR) images. However, better correlation does not always mean better ablation results and impact of respiratory gating on AF ablation has not been studied yet.
AccuResp algorithm (Biosense Webster, Diamond Bar, Ca) automatically detects out-of-gate acquisition and exclude them from the reconstructed anatomy, thus it may provide accurate maps at the expense of longer mapping times. More reliable maps may shorten procedure times and may increase success rates. On the other hand, integration of reconstructed electroanatomical maps and pre-acquired static 3D images might compensate negative effects of nongated maps. Relative changes in left atrial anatomy are most pronounced in the distal pulmonary veins and in the left atrium body near the mitral valve [9]. Therefore, avoiding from these regions during image integration might have similar effects as respiratory gating.
The aim of this study was to assess the impact of respiratory gating on electroanatomic mapping and image integration guided AF ablation procedures.
Methods
Study population
One-hundred-forty consecutive patients, who underwent catheter ablation of AF for the first time admitted to the study. Three experienced physicians, who perform totally more than 400 AF ablations per year participated the study. All procedures were done by the same physicians in both groups under conscious sedation and spontaneous respiration. All patients had symptomatic, drug refractory AF. The demographics of the patients are summarized in Table 1.
Electroanatomical map construction and respiratory gating
Left atrial geometry was constructed using fast anatomical mapping (FAM) feature of EAM system Carto 3 (Biosense Webster, Diamond Bar, Ca). Navistar 7F open irrigated-tip catheter (Biosense Webster, Diamond Bar, Ca) was used for mapping and ablation. In respiratory gated group, AccuResp module (Biosense Webster, Diamond Bar, Ca) was enabled and respiration training was done. During the training phase, mapping catheter was placed in the left inferior pulmonary vein with a good contact. Gated threshold was set at 30 % of the respiratory cycle and FAM of the LA was constructed. Mapping was started immediately in nongated group. The time from the connection of mapping catheter to the first RF application was defined as electroanatomical map reconstruction time. Resolution thresholds were set at the same levels in both groups during FAM construction.
CT/MRI image acquisition and integration
After completion of FAMs, they were integrated with pre-acquired CT or MRI images (125 patients CT, 15 patients MRI). CT was performed using 64 slice CT scanner (Philips Brilliance iCT 256) and MR angiography was performed using 1.5-T MR scanner (Philips Achieva 1.5-T Dual Nova HP R2.6.3p7). Carto Merge System (Biosense Webster, Diamond Bar, Ca) was used for segmentation and integration of LA model into electroanatomic maps. Because the respiratory changes are most prominent in distal PVs and anterior areas near the mitral valve, these regions were not used during landmark registration [9].
Catheter ablation
Circumferential left atrial ablation lines were performed around the antrum of ipsilateral pulmonary veins with power limited to 30 W and temperature to 43 °C. PVs were continuously assessed for electrical isolation using the circular mapping catheter. After completion of the lines, bidirectional block was verified with pacing maneuvers. When needed additional lines were added in patients with persistent AF. Ablation of complex fractionated electrograms was not performed. If AF persisted following the linear ablation, DC cardioversion was performed. Ablation time was determined from the beginning of first ablation to the end of last ablation. Each application duration was automatically calculated by electrophysiology recording system, and total value was defined as total RF application duration.
Statistical analysis
All variables are represented as a mean ± standard deviation or median and interquartile range as appropriate. Normality was evaluated using Kolmogorov–Smirnov test. Comparisons between groups were performed with either an unpaired Student’s t test or Mann–Whitney U test, where a normal distribution could not be assumed. A p < 0.05 was considered to be statistically significant.
Results
We enrolled 140 patients, who underwent AF ablation for the first time. In respiratory gated group (70 patients, mean age 59 ± 10 years, 21 female) underwent procedures after enabling AccuResp module. In nongated group (70 patients, mean age 56 ± 10 years, 25 females), procedures were performed using the same EAM system without enabling the AccuResp module. Baseline clinical factors did not differ between the two groups (Table 1).
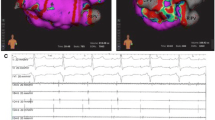
Durations from the beginning of the procedure to beginning of the EAM reconstruction were similar in both groups [median 22 min, (IQR 17–27) vs median 21 min (IQR 16–25), p = 0.40, Table 2; Fig. 1].

Comparison of different time intervals during AF ablation. Note that the intervals from the beginning of the procedure to the start of ablation are similar in both groups, but the ablation time is significantly shorter in respiratory gated group
In gated group, electroanatomical maps reconstructed within median 14 (IQR 12–16) min vs median 13 (IQR 10–18) min in nongated group (p = 0.19) (Table 2; Fig. 1).
Significantly shorter ablation times were observed in respiratory gated group [median 37 (IQR 32–53) min vs median 48 (IQR 39–65) min, p < 0.05]. However, total RF application durations were not different between two groups [median 1,554 (IQR 1,213–2,196) s vs median 1,802 (IQR 1,344–2,448) s, p = 0.11, Table 2; Fig. 1].
A significant reduction in total procedure times [median 77 (IQR 66–95) min vs median 82 (IQR 72–104) min, p < 0.05] and fluoroscopy times [median 14 (IQR 9–17) min vs median 16 (IQR 12–22) min, p < 0.05] were observed in the respiratory gated group.
One patient from each group had significant pericardial effusion and developed cardiac tamponade 24 h after procedures. Pericardiocentesis was performed for both patients and surgery was not needed. Vascular access complications rates were similar among two groups. Two hematoma developed in nongated group and one hematoma developed in gated group (p = 0.56). None of them required intervention.
In nongated group, roof lines were performed in three patients and roof plus mitral isthmus lines were performed in five patients. In gated group, roof plus mitral isthmus lines were performed in six patients and box isolation was performed in one patient. Successful pulmonary vein isolation and sinus rhythm were obtained in all patients. DC cardioversion was performed in 46 patients (24 in nongated and 22 in gated group, p = 0.71).
Discussion
Principal findings of our study demonstrated that respiratory gating allows faster AF ablation procedures and reduces X-ray screening. However, the use of this technology was not able to reduce the total RF application durations.
During the past decade, EAM systems achieved remarkable advances and became the cornerstone of AF ablations [1, 10, 11]. Despite these advances, an accuracy of maps is still affected by biological factors, such as respiration [9, 12]. During EAM reconstruction, catheter movements are affected by respiration and significant changes occur in LA–PV geometry. Moreover, deep inspiration during reconstruction could deform maps. PV ostiums are crucial landmarks of AF ablation and important changes in their positions, predominantly in inferior direction, were reported during respiration [9].
Respiratory gating based on the end expiration might provide accurate maps and compensate negative effects of respiration. Previous work by Beinart et al. [8] has confirmed that more accurate electroanatomical maps can be obtained by respiratory gating. The only study investigated the impact of respiratory gating on RF ablation was about cavotricuspid isthmus (CTI) ablation procedures [13]. In this study, respiratory gated acquisition resulted in a better visualization of CTI and a significant reduction in fluoroscopy and RF times. However, LA anatomy is more complex, then CTI and ablation lines in multiple dimensions are needed during PV isolations. To the best of our knowledge, this is the first study investigated the impact of respiration gating on atrial fibrillation ablation and our results support its favorable effects.
EAM reconstruction times
AccuResp module automatically detects out-of-gate acquisition and excludes them from the created anatomy, thus it does not slows down the mapping procedure. Although reconstruction times were slightly longer in respiratory gated group, difference was not significant. However, all procedures in our study were performed with image integration and only crucial parts for landmark registration were mapped instead for detailed reconstruction of all LA. Therefore, our results may not be generalized for ablation procedures without image integration.
Potential advantage of respiratory gating
Significant reduction in procedural times is the result of shorter ablation times in respiratory gated group. Durations from the beginning of the procedure to the start of ablation were similar in both groups, but the ablation times were significantly shorter in respiratory gated group (Fig. 1). On the other hand, total RF energy applied to isolate PVs was not influenced by respiratory gating. These data seem to be the result of uninterrupted ablation applications in respiratory gated group. Although this study was not designed to evaluate the accuracy of electroanatomical maps and compare them with pre-acquired CT or MRI images, reduction in ablation and fluoroscopy times supports superiority of gated maps.
Catheter-tissue contact force is also critically influenced by respiration [14, 15]. However, it seems to be directly related to the respiratory movement itself and it is hard to suggest that the respiratory gating had positive effects on contact force. Catheter positions are visualized real-time during ablation and respiratory gating does not have effect of catheter view, it only excludes out-of-gate ablation points and may affect shape of ablation lines. For these reasons, main advantage of respiratory gating is attributable to the realistic LA geometry construction.
In addition, merging electroanatomical maps and pre-acquired static 3D images did not compensate negative effects of respiration. Although the prominently mobile points were avoided during landmark registration, there were significant differences between two groups.
Safety
We observed no difference in cardiovascular complication rates among two groups. However, extensive use of fluoroscopy during long ablation procedures increases the radiation risk for patients and medical staff [16–19]. Moreover, radiation exposure during AF ablation is longer than simpler catheter ablation procedure [20, 21]. EAM systems have been demonstrated to reduce fluoroscopy times during RF ablations [22–24]. Our results imply that the respiratory gating provides further reduction in fluoroscopy time.
Limitations
It should be remembered that all procedures in our study were performed with Carto3 system under guidance of image integration. Therefore, validation of our results is limited for this ablation technique. All patients ablated under conscious sedation and spontaneous respiration. Our results cannot be generalized for procedures performed under general anesthesia, where respiratory rate and tidal volumes are predictable. In addition, this study was not designed to assess long-term clinical outcome after AF ablation, but was focused on procedural outcomes. Studies evaluate the long-term effects of this technique are needed.
Conclusion
Respiratory gated electroanatomic mapping significantly improves ablation and fluoroscopy times during AF ablation. Beside these advantages, using automatic respiratory gating module does not prolong mapping times.
References
Calkins H, Kuck KH, Cappato R et al (2012) 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace 14:528–606
Camm AJ, Lip GY, De Caterina R et al (2012) 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 33:2719–2747
Said SM, Braun-Dullaeus RC (2011) Comment on the European guidelines for the management of atrial fibrillation. Clin Res Cardiol 100:543–544
Chun KR, Schmidt B, Kuck KH et al (2013) Catheter ablation of atrial fibrillation in the young: insights from the German Ablation Registry. Clin Res Cardiol 102:459–468
Richter B, Gwechenberger M, Socas A et al (2012) Markers of oxidative stress after ablation of atrial fibrillation are associated with inflammation, delivered radiofrequency energy and early recurrence of atrial fibrillation. Clin Res Cardiol 101:217–225
Noseworthy PA, Malchano ZJ, Ahmed J, Holmvang G, Ruskin JN, Reddy VY (2005) The impact of respiration on left atrial and pulmonary venous anatomy: implications for image-guided intervention. Heart Rhythm 2:1173–1178
Klemm HU, Steven D, Johnsen C et al (2007) Catheter motion during atrial ablation due to the beating heart and respiration: impact on accuracy and spatial referencing in three-dimensional mapping. Heart Rhythm 4:587–592
Beinart R, Kabra R, Heist KE et al (2011) Respiratory compensation improves the accuracy of electroanatomic mapping of the left atrium and pulmonary veins during atrial fibrillation ablation. J Interv Card Electrophysiol 32:105–110
Ector J, De Buck S, Loeckx D et al (2008) Changes in left atrial anatomy due to respiration: impact on three-dimensional image integration during atrial fibrillation ablation. J Cardiovasc Electrophysiol 19:828–834
Rotter M, Takahashi Y, Sanders P et al (2005) Reduction of fluoroscopy exposure and procedure duration during ablation of atrial fibrillation using a novel anatomical navigation system. Eur Heart J 26:1415–1421
Bertaglia E, Bella PD, Tondo C et al (2009) Image integration increases efficacy of paroxysmal atrial fibrillation catheter ablation: results from the CartoMerge Italian Registry. Europace 11:1004–1010
Sra J, Ratnakumar S (2008) Cardiac image registration of the left atrium and pulmonary veins. Heart Rhythm 5:609–617
de Ruvo E, Dottori S, Sciarra L et al (2013) Impact of respiration on electroanatomical mapping of the right atrium: implication for cavotricuspid isthmus ablation. J Interv Card Electrophysiol 36:33–40
Kumar S, Morton JB, Halloran K et al (2012) Effect of respiration on catheter-tissue contact force during ablation of atrial arrhythmias. Heart Rhythm 9:1041–1047
Wakili R, Clauss S, Schmidt V et al (2014) Impact of real-time contact force and impedance measurement in pulmonary vein isolation procedures for treatment of atrial fibrillation. Clin Res Cardiol 103:97–106
Efstathopoulos EP, Katritsis DG, Kottou S et al (2006) Patient and staff radiation dosimetry during cardiac electrophysiology studies and catheter ablation procedures: a comprehensive analysis. Europace 8:443–448
McFadden SL, Mooney RB, Shepherd PH (2002) X-ray dose and associated risks from radiofrequency catheter ablation procedures. Br J Radiol 75:253–265
Pantos I, Koukorava C, Nirgianaki E et al (2012) Radiation exposure of the operator during cardiac catheter ablation procedures. Radiat Prot Dosimetry 150:306–311
Lindsay BD, Eichling JO, Ambos HD, Cain ME (1992) Radiation exposure to patients and medical personnel during radiofrequency catheter ablation for supraventricular tachycardia. Am J Cardiol 70(2):218–223
Lickfett L, Mahesh M, Vasamreddy C et al (2004) Radiation exposure during catheter ablation of atrial fibrillation. Circulation 110:3003–3010
Macle L, Weerasooriya R, Jais P et al (2003) Radiation exposure during radiofrequency catheter ablation for atrial fibrillation. Pacing Clin Electrophysiol 26:288–291
Estner HL, Deisenhofer I, Luik A et al (2006) Electrical isolation of pulmonary veins in patients with atrial fibrillation: reduction of fluoroscopy exposure and procedure duration by the use of a non-fluoroscopic navigation system (NavX). Europace 8:583–587
Sporton SC, Earley MJ, Nathan AW, Schilling RJ (2004) Electroanatomic versus fluoroscopic mapping for catheter ablation procedures: a prospective randomized study. J Cardiovasc Electrophysiol 15:310–315
Stabile G, Scaglione M, del Greco M et al (2012) Reduced fluoroscopy exposure during ablation of atrial fibrillation using a novel electroanatomical navigation system: a multicentre experience. Europace 14:60–65
Acknowledgments
The authors acknowledge the János Bolyai Research Scholarship of the Hungarian Academy of Sciences and Hungarian Scientific Research Found (OTKA 105555 LG, GSZ).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Özcan, E.E., Szeplaki, G., Tahin, T. et al. Impact of respiration gating on image integration guided atrial fibrillation ablation. Clin Res Cardiol 103, 727–731 (2014). https://doi.org/10.1007/s00392-014-0707-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-014-0707-1