
Abstract
Purpose
To undertake a meta-analysis of comparative data of laparoscopic versus open inguinal herniotomy in infants and children.
Methods
We searched MEDLINE, EMBASE, and The Cochrane Central Controlled Trials Registry for relevant randomized controlled trials and observational studies comparing laparoscopic with open inguinal hernia repair in children aged less than 19 years.
Results
Data on 2,699 children were identified from 10 comparative studies. Laparoscopic techniques were associated with a trend towards higher recurrence rate (OR = 1.81; 95% CI 0.89–3.67; p = 0.10), longer operative time for unilateral repairs (WMD = 10.23; 95% CI 8.82–11.64; p < 0.00001), and may be shorter operative time for bilateral repairs (WMD = −4.54; 95% CI −11.63 to 2.55; p = 0.21). There was a significant reduction in developing a contralateral metachronous inguinal hernia in the laparoscopic group (OR = 0.37; 95% CI 0.20–0.67; p = 0.001).
Conclusions
Laparoscopic inguinal herniotomy is significantly associated with longer operative time for unilateral cases and a reduction in metachronous hernia development. There was a trend towards higher recurrence rate for laparoscopic repairs and shorter operative time for bilateral cases. A well conducted randomized controlled trial is warranted to compare both approaches.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia repair is one of the most frequently performed pediatric surgical operations [1]. Open repair of an inguinal hernia has been accepted as the method of choice since it was first described more than 50 years ago due to its lower morbidity, good cosmesis, and lower rates of recurrence [2–4]. Several pediatric laparoscopic inguinal hernia repair techniques have been introduced over the last few years [5–15]. Some centers use laparoscopes routinely for inguinal hernia repair in children because of the belief that the laparoscopic repair is less painful to the patients, results in earlier recovery and better cosmesis [16, 17]. In addition, laparoscopic repair also allows contralateral patent process vaginalis (PPV)/hernias to be defined and repaired in the same operation [9]. Unresolved debate still exists regarding the benefit of using laparoscopy over conventional open inguinal hernia repair even among laparoscopic surgeons due to the concern about its higher recurrence rate [9]. The aim of this study was to assess any differences in complication rates and outcome following surgery for indirect inguinal hernia between infants and children treated using the open and laparoscopic techniques. We performed a systematic review and meta-analysis of the existing evidence.
Methods
Search strategy
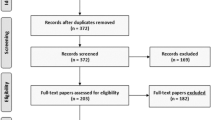
The search strategy is summarized in Fig. 1. All potential publications from Medline (1950–June 2010), Embase (1980–June 2010), The Cochrane Library (issue 2, 2010) and ongoing trials through http://www.clinicaltrials.gov website were identified. The following subject headings (MeSH) and text word terms were utilized: inguinal hernia, laparoscopy, minimal access surgery, infant(s), neonate(s), newborn(s), child, paediatric, pediatric. No language restriction was applied. Additional citations were sought using references in articles retrieved from searches. Content experts were contacted to identify unpublished and ongoing studies.

Schematic summary of search strategy
Inclusion criteria
All comparative studies of the laparoscopic and open approaches for indirect inguinal hernia in children aged less than 19 years were selected. The primary outcome measure was the recurrence rate. Other clinically important outcomes such as rate of contralateral PPV, operative time, postoperative pain and recovery, cosmesis, postoperative testicular atrophy, postoperative hydrocele and stitch granuloma/abscess were also sought. Other case series were considered for descriptive analysis.
Data extraction
Retrieved articles were assessed for eligibility and data on patients, intervention, control, outcomes and methodological quality were abstracted independently by two authors. Discrepancies were resolved by discussion and consensus.
Methodological quality of the studies
The quality of the included comparative studies was assessed independently by two authors. The Cochrane Collaboration criteria for randomized controlled trials was utilized (randomization, allocation concealment, blinding and completeness of follow-up). Cohort studies were assessed using the Newcastle-Ottawa Quality Assessment Scale [18]. The methodological details of the included studies were extracted from the published data.
Statistical analysis
For dichotomous outcomes, odds ratio (OR) and its associated confidence interval were calculated. For continuous outcomes, treatment effect was expressed as mean difference and its calculated standard deviation. If appropriate, meta-analysis of pooled data of the comparative studies was performed using a fixed effect model. Review Manager 5.0.24 software was used for statistical analysis. Heterogeneity was defined as a significant test of heterogeneity (p < 0.1) and/or differences in the treatment effects across studies. Tests for between study heterogeneity (including the I 2 test) were performed. When statistical heterogeneity existed, a random effect model was utilized.
Results
Description of studies
Initial electronic search yielded 290 Medline, 216 Embase, 5 Cochrane Library (issue 2, 2010) and 7 ClinicalTrials.gov potentially relevant citations. After screening the abstracts, 48 articles were reviewed in full texts. Thirty-four articles have met the predefined inclusion criteria (Fig. 1). Ten published studies were identified (Niyogi [19]; Tsai [20]; Koivusalo [21]; Endo [22]; Bharathi [23]; Hassan [24]; Koivusalo [25]; Chan [17]; Oue [26]; Antao [27]) in which the laparoscopic and open approaches for repair of pediatric inguinal hernias were directly compared (Table 1) [17, 19–27].
Quality of included studies
Two randomized controlled trial (Koivusalo [21]; Chan [17]), one nonrandomized clinical trial (Tsai [20]) and seven observational comparative studies (Niyogi [19]; Endo [22]; Bharathi [23, 28]; Hassan [24]; Koivusalo [25]; Oue [26]; Antao [27]) were assessed.
Koivusalo 2009 [21]
This was a single center study. Infants and children between 4 months and 16 years of age were randomized for laparoscopic and open repair. The randomization procedure using closed envelopes was utilized but was not adequately described. Allocation concealment was apparently adequate. Outcome assessment was masked. It was not clear that the analysis was done on an intention to treat basis. Not all enrolled infants and children were accounted for in the final results for various reasons.
Chan 2005 [17]
This was a single center study. Infants and children between 3 months and 18 years of age were randomized for laparoscopic and open repair. The randomization procedure was not adequately described. Allocation concealment was apparently adequate. Outcome assessment was masked. Analysis was done on an intention to treat basis. All infants and children were accounted for in the final results.
Tsai 2010 [20]
This was nonrandomized clinical trial. Children with a mean age of 4.9 years underwent either open or minilaparoscopic herniorrhaphy. The choice between the two approaches was made according to the wish of child and/or parent. The selection process was adequate. The groups were comparable with regard to important baseline factors. Outcomes were obtained from medical record. The follow-up period was adequate and those lost to follow-up were excluded from the analysis. The study scored 8/9 on Newcastle-Ottawa Quality Assessment Scale.
Endo 2009 [22]
This was a large prospective cohort study. Children between 1 month and 24 years of age were included. The selection process was adequate. Groups were comparable except for gender and presence of umbilical hernia. Outcomes were obtained from medical records. Description for follow-up was not adequate and the period was not long enough (7 months). The study scored 6/9 on Newcastle-Ottawa Quality Assessment Scale.
Niyogi 2010 [19]
This was a retrospective cohort study. Children between 1 day and 15 years of age were included. The selection process was adequate. Comparability between groups cannot be assessed. Outcomes were obtained from medical records. Follow-up period was not long enough. The study scored 6/9 on Newcastle-Ottawa Quality Assessment Scale.
Bharathi 2008 [23, 28]
This was a cohort study. Children between 1½ year and 14 years of age were included. The selection process was adequate. Groups were comparable except for age. Outcomes were obtained from medical records. Follow-up was not adequately described. The study scored 6/9 on Newcastle-Ottawa Quality Assessment Scale.
Hassan 2007 [24]
This was a retrospective cohort study. Infants and children between 4 months and 7 years of age were included. The selection process was adequately described. The group was comparable with regard to important baseline factors. However, only males were included. A clear exclusion criteria was not presented. Outcome of patients was done through medical record reference; however, the follow-up period was not long enough to assess recurrence rate adequately (3 months only). The study scored 5/9 on Newcastle-Ottawa Quality Assessment Scale.
Koivusalo 2007 [25]
This was a retrospective cohort study. Infants and children between 1 and 81 months of age who had incarcerated hernias were included. The selection process was adequately described. Data were collected from surgical records. Included patients were controlled for age, gender, site, and weight. Only 72% of patients were seen in the outpatient clinics postoperatively. However, a telephone survey was conducted to ascertain outcomes up to 97% of included cohort. The median follow-up period was 26 months. The study scored 6/9 on Newcastle-Ottawa Quality Assessment Scale.
Oue 2005 [26]
This was a retrospective cohort study. Infants and children between 4 months and 13 years of age were included. The selection process was adequately described. The groups were comparable with regard to important baseline factors; however, only girls were included. Outcome of patients was done through medical record reference. The follow-up was complete and long enough to assess for recurrence (12–48 months). The study scored 8/9 on Newcastle-Ottawa Quality Assessment Scale.
Antao 2004 [27]
This was a retrospective cohort study. Only infants were included. The selection process was adequately described. Data were collected from surgical records. Comparability between groups was not described adequately. Outcome of patients was done through medical record reference. However, the follow-up period was not long enough to assess recurrence rate adequately (7 months only). The study scored 6/9 on Newcastle-Ottawa Quality Assessment Scale.
Recurrence
The two randomized controlled trials (Koivusalo [21] and Chan [17]) on 172 infants and children between age of 3 months and 18 years have reported a recurrence rate of 0–4% for laparoscopic approach compared with 0–2% for the open approach. In a meta-analysis of 10 comparative studies, there was a trend towards higher recurrence rate for the laparoscopic inguinal hernia repair [OR = 1.81; 95% CI 0.89–3.67; p = 0.10] (Fig. 2a). A sensitivity analysis was conducted where studies limited to girls, and/or with a median follow-up less than 6 months, and/or addressing a complicated hernia, and/or limited to infants were excluded and the meta-analysis of the remaining 6 comparative studies had shown a comparable recurrence rate among the groups [OR = 0.87; 95% CI 0.34–2.23; p = 0.76] (Fig. 2b).

a Forest plot comparing recurrence rate for children treated with laparoscopic versus open inguinal herniotomy. b Sensitivity analysis of recurrence rate among children treated by laparoscopic versus open inguinal herniotomy
Operative time
Nine comparative studies reported on operative time for unilateral hernia repair. The operative time was significantly longer in the laparoscopic group compared to open group for unilateral hernia [weighted mean difference (WMD) 10.23; 95% CI 8.82–11.64; p < 0.00001] (Fig. 3a). Four comparative studies reported on operative time for bilateral hernia and there was a trend towards shorter operative time in favor of laparoscopic group [WMD −4.54; 95% CI −11.63 to 2.55; p = 0.21] (Fig. 3b).

a Forest plot comparing operative time for children treated with unilateral laparoscopic versus open inguinal herniotomy. b Forest plot comparing operative time for children treated with bilateral laparoscopic versus open inguinal herniotomy
Contralateral patent processus vaginalis (PPV)/contralateral metachronous inguinal hernia
Eight comparative studies reported on contralateral patency (Table 1). The prevalence of contralateral PPV was ranging from 21 to 47% in the laparoscopic group. In a meta-analysis of seven comparative studies that reported on development of metachronous hernia, there was a significant reduction in metachronous hernia development in the laparoscopic group [OR = 0.37; 95% CI 0.20–0.67; p = 0.001] (Fig. 4).

Forest plot comparing contralateral metachronous inguinal hernia development for children treated with laparoscopic versus open inguinal herniotomy
There was insufficient data with regard to cosmesis, composite morbidity, conversion rate, and postoperative pain to be pooled up and meta-analyze. However, the two randomized controlled trials have revealed a conflicting data with regard to postoperative pain, recovery and cosmesis. Chan et al. [17] concluded their trail stating that children who underwent laparoscopic repair suffered less pain, and their recovery and wound cosmesis are more satisfactory. While Koivusalo et al. [21] concluded that recovery and cosmetic outcome were similar between the groups; however, the laparoscopic hernia repair was associated with increased postoperative pain.
Discussion
Our review examined the safety and efficacy of the laparoscopic approach in the management of inguinal hernias in infants and children. Ten comparative studies were reviewed. Although the data is limited, the laparoscopic approach was associated with a trend towards higher recurrence rate. A sensitivity analysis had shown a comparable recurrence rate among groups, where studies limited to infants, or girls, or addressing incarcerated hernia, or having a short follow-up period were excluded. This could be explained partially by refinements in techniques and by achieving the required learning curve in the recent included studies. A narrative review by Bharathi et al. [28] of 22 studies (3 comparative studies) have shown a recurrence rate ranging from 0 to 5% for the laparoscopic inguinal herniotomy, which is comparable with that for open repair. A recent case series by Parelkar et al. [29] have demonstrated technical modifications where they were able to bring down the recurrence rate from 2.9 to 0%.
The operative time for unilateral cases was significantly longer for those who underwent minimal access surgery for inguinal hernia in children. The direction of this effect was consistent; however, the included studies were heterogeneous due to various reasons including technical, surgeon, patient, and institutional factors. In those who underwent bilateral repairs, there was a trend towards shorter operative time in favor of laparoscopic approach. The direction of this effect was consistent and homogenous among studies’ reported operative time for bilateral repairs [17, 19, 20, 22]. This temporal efficacy that has been observed for bilateral cases could be explained partially by avoiding additional access for the opposite side [23, 28].
Although the fate of a contralateral PPV remains unclear, the laparoscopic approach was advantageous in detecting a contralateral PPV which could be dealt with in the same operation and potentially decrease the rate of metachronous hernias development. Our review has demonstrated a significant reduction in the development of contralateral metachronous hernia from 6.3% (72/1144) for open repairs to 0.9% (14/1,571) for laparoscopic approach. The 14 patients, who developed metachronous hernia in the laparoscopic group, did so, because the contralateral PPVs were not closed at the initial repairs. A systematic review by Ron et al. [30] on 22,846 children revealed an overall incidence of 7.2% for contralateral metachronous inguinal hernia.
Despite numerous case series spanning over a decade of surgical practice, only two randomized controlled trials were identified, studying 172 infants and children. The conflicting data revealed by the two randomized controlled trials could be explained partially by the possibility of selection bias and by the presence of potential confounding factors including different operative techniques and lack of standardization of other received treatments [17, 21].
Although our review utilized a very comprehensive search strategy to minimize the effect of publication bias, only two randomized clinical trial was included. Therefore, our review is a summary of the existing evidence with limitation to the conclusions drawn from these data due to the quality of the included studies. To minimize the reviewer bias, all steps of this review were conducted independently by two review authors. Our review’s conclusions are hampered by the quality and the small sample size of the most included studies. The studies included were heterogeneous in study design, age and gender of enrolled infants, primary or recurrent hernia, simple or complicated hernias. However, due to the limited number of studies and enrolled children, a subgroup analysis was not feasible.
Recurrent groin hernias can be due to various defects and minimal access surgery is the best method for their detection and simultaneous repair [31]. Laparoscopic repair seems to be the preferred method for recurrent hernia after open repair, with less chance of damage to vas or testicular vessels by going through a virgin territory, and scattered case series have shown its comparability to an initial laparoscopic repair [32, 33].
Minimal access surgery may be advantageous for incarcerated inguinal hernia. The creation of pneumoperitoneum dilates the deep ring, which would help in the reduction process, along with manual external compression. Moreover, Laparoscopy will allow to inspect the bowel for any evidence of ischemia and to do the simultaneous repair at a non-edematous tissue [34, 35].
We were unable to identify any clear benefit of laparoscopic inguinal herniotomy over the open approach. This review brings to light the paucity of existing good-quality evidence in this area. A large-scale randomized well-powered clinical trial comparing the two approaches should be conducted to guide our practice. We have justified the completion of this review, as it is our opinion that there is currently inadequate information on which to base a treatment decision.
References
Kapur P, Caty MG, Glick PL (1998) Pediatric hernias and hydroceles. Pediatr Clin North Am 45:773–789
Levitt MA, Ferraraccio D, Arbesman MC, Brisseau GF, Caty MG, Glick PL (2002) Variability of inguinal hernia surgical technique: a survey of North American pediatric surgeons. J Pediatr Surg 37:745–751
Antonoff MB, Kreykes NS, Saltzman DA, Acton RD (2005) American academy of pediatrics section on surgery hernia survey revisited. J Pediatr Surg 40:1009–1014
Ein SH, Njere I, Ein A (2006) Six thousand three hundred sixty one pediatric inguinal hernias; a 35-year review. J Pediatr Surg 41:980–986
Schier F (1998) Laparoscopic herniorraphy in girls. J Pediatr Surg 33:1495–1497
Montupet P, Esposito C (1999) Laparoscopic treatment of congenital inguinal hernia in children. J Pediatr Surg 34:420–423
Haddad M, Kamal A (2000) Is ligation of the hernia sac necessary? J Pediatr Endosurg Innov Tech 4:77
Schier F (2000) Laparoscopic surgery of inguinal hernia in children—initial experience. J Pediatr Surg 35:1331–1338
Schier F, Montupet P, Esposito C (2002) Laparoscopic inguinal herniorraphy in children: a three-center experience with 933 repairs. J Pediatr Surg 37:395–397
Prasad R, Lovvorn HN III, Wadle GM, Lobe TE (2003) Early experience with needlescopic inguinal herniorraphy in children. J Pediatr Surg 38:1055–1058
Chan KL, Tam PKH (2003) A safe laparoscopic technique for the repair of inguinal hernias in boys. J Am Coll Surg 196:987–989
Chan KL, Tam PKH (2004) Technical refinements in laparoscopic repair of childhood inguinal hernia. Surg Endosc 18:957–960
Yip KF, Tam PK, Li MK (2004) Laparoscopic flip-flap hernioplasty: an innovative technique for pediatric hernia surgery. Surg Endosc 18:1126–1129
Jialin L, Hanxin Z, Xiaofang Y, Shiyun B (2007) Laparoscopic herniorraphy combined ligation of the hernial sac and suturation of the internal ring in children with indirect inguinal hernias. Surg Laparosc Endosc Percutan Tech 17:95–98
Chan KL, Chan HY, Tam PKH (2007) Towards a near-zero recurrence rate in laparoscopic inguinal hernia repair for pediatric patients of all ages. J Pediatr Surg 42:1993–1997
Laberge JM (2002) What’s new in pediatric surgery? J Am Coll Surg 195:208–218
Chan KL, Hui WC, Tam PKH (2005) Prospective, randomized, single-center, single-blind comparison of laparoscopic vs open repair of pediatric inguinal hernia. Surg Endosc 19:927–932
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P (2005) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.lri.ca/programs/ceu/oxford.htm
Niyogi A, Tahim AS, Sherwood WJ, De Caluwe D, Madden NP, Abel RM, Haddad MJ, Clarke S (2010) A comparative study examining open inguinal herniotomy with or without hernioscopy to laparoscopic inguinal hernia repair in a pediatric population. Pediatr Surg Int 26:387–392
Tsai YC, Wu CC, Yang SSD (2010) Open versus minilaparoscopic herniorrhaphy for children: a prospective comparative trial with midterm follow-up evaluation. Surg Endosc 24:21–24
Koivusalo AI, Korpela R, Wirtavuori K, Piiparinen S, Rintala RJ (2009) A single-blinded, randomized comparison of laparoscopic versus open hernia repair in children. Pediatrics 123:332–337
Endo M, Watanabe T, Nakano M, Yoshida F, Ukiyama E (2009) Laparoscopic completely extraperitoneal repair of inguinal hernia in children: a single-institute experience with 1,257 repairs compared with cut-down herniorrhaphy. Surg Endosc 23:1706–1712
Bharathi RS, Arora M, Baskaran V (2008) Congenital inguinal hernia: lap vs open surgery: how great is the difference? JSLS 12:277–281
Hassan ME, Mustafawi AR (2007) Laparoscopic flip-flap technique versus conventional inguinal hernia repair in children. JSLS 11:90–93
Koivusalo A, Pakarinen MP, Rintala RJ (2007) Laparoscopic herniorrhaphy after manual reduction of incarcerated inguinal hernia. Surg Endosc 21:2147–2149
Oue T, Kubota A, Okuyama H, Kawahara H (2005) Laparoscopic percutaneous extraperitoneal closure (LPEC) method for the exploration and treatment of inguinal hernia in girls. Pediatr Surg Int 21:964–968
Antao B, Samuel M, Curry J, Kiely E, Drake D (2004) Comparative evaluation of laparoscopic vs. open inguinal herniotomy in infants. Pediatr Endosurg Innov Tech 8:302–309
Bharathi RS, Arora M, Baskaran V (2008) Minimal access surgery of pediatric inguinal hernias: a review. Surg Endosc 22:1751–1762
Parelkar SV, Oak S, Gupta R, Sanghvi B, Shimoga PH, Kaltari D, Prakash A, Shekhar R, Gupta A, Bachani M (2010) Laparoscopic inguinal hernia repair in the pediatric age group- experience with 437 children. J Pediatr Surg 45:789–792
Ron O, Eaton S, Pierro A (2007) Systematic review of the risk of developing a metachronous contralateral inguinal hernia in children. BJS 94:804–811
Perlstein J, Du Bois J (2000) The role of laparoscopy in the management of suspected recurrent pediatric hernias. J Pediatr Surg 35:1205–1208
Esposito C, Montupet P (1998) Laparoscopic treatment of recurrent inguinal hernia in children. Pediatr Surg Int 14:182–184
Chan KL (2007) Laparoscopic repair of recurrent childhood inguinal hernias after open herniotomy. Hernia 11:37–40
Kaya M, Huckstadt T, Schier F (2006) Laparoscopic approach to incarcerated inguinal hernia in children. J Pediatr Surg 41:567–569
Shalaby R, Shams AM, Mohamed S, El-Leathy M, Ibrahem M, Alsaed G (2007) Two-trocar needlescopic approach to incarcerated inguinal hernia in children. J Pediatr Surg 42:1259–1262
Acknowledgments
I would like to thank Dr Khalid Alfaleh for his advice regarding some of the aspects of the methodology of this systematic review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alzahem, A. Laparoscopic versus open inguinal herniotomy in infants and children: a meta-analysis. Pediatr Surg Int 27, 605–612 (2011). https://doi.org/10.1007/s00383-010-2840-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-010-2840-x