
Abstract
To elucidate left ventricular function in pulmonary hypertension, we measured parameters of left ventricular as well as right ventricular function by echocardiography in 11 patients with pulmonary hypertension (idiopathic pulmonary artery hypertension in 4, chronic thromboembolic pulmonary hypertension in 5, and other pulmonary hypertension in 2). The percent change in these parameters 6 months after treatment with pulmonary artery vasodilators (beraprost in 8 and sildenafil in 3) was assessed. There was a correlation between the relative change in right ventricular systolic pressure (RVSP) and the relative changes in left ventricular outflow tract velocity–time integral (r = −0.730, P = 0.011) and mitral valve velocity–time integral (r = −0.621, P = 0.041). However, there was no correlation between the relative change in RVSP and the relative changes in left ventricular ejection fraction, left ventricular diastolic dimension, and systolic blood pressure. The relative change in RVSP was also correlated with the relative change in early diastolic myocardial velocity at the medial mitral annulus (r = −0.675, P = 0.023). Reduction of RVSP by pulmonary artery vasodilators might increase left ventricular preload, leading to an increase in stroke volume. Right ventricular load reduction might improve left ventricular diastolic function in patients with pulmonary hypertension, possibly through altered interventricular septal performance.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pulmonary hypertension of any etiology is a rapidly progressive disease and is associated with a high mortality despite medical interventions [1]. Since pulmonary artery hypertension leads to right heart failure via right cardiac pressure overload, right ventricular function including pulmonary artery pressure, right ventricular or atrial pressures, right ventricular or atrial enlargement, and tricuspid regurgitation are often evaluated in the clinical setting [2]. By contrast, left ventricular function in pulmonary artery hypertension is not well understood. Several studies using Doppler echocardiographic measurement have suggested impaired left ventricular filling in pulmonary hypertension [3, 4]. In these studies, left ventricular isovolumic relaxation time was prolonged in patients with pulmonary hypertension in comparison with normal individuals, possibly being associated with right ventricular pressure overload. However, there are only limited data in these studies with which to discuss clinical significance.
In this study, we applied recent novel echocardiographic techniques, including tissue Doppler imaging, in patients with pulmonary hypertension to acquire more detailed information about left ventricular systolic and diastolic function.
Patients and methods
Patients
The study enrolled 11 patients with untreated pulmonary hypertension (4 men and 7 women; age, 61.5 ± 19.0 years) including idiopathic pulmonary artery hypertension in 4, chronic thromboembolic pulmonary hypertension in 5, pulmonary hypertension associated with collagen disease in 1, and pulmonary hypertension associated with chronic obstructive pulmonary disease in 1. Patients with pulmonary hypertension secondary to left heart failure or congenital heart disease were excluded. The diagnosis in each patient was based on symptoms, electrocardiogram, chest X-ray, echocardiogram, arterial blood gas analysis, X-ray computed tomography, magnetic resonance imaging, ventilation/perfusion scintigraphy, right cardiac catheterization, and/or pulmonary angiography, according to the American College of Chest Physicians (ACCP) evidence-based clinical practice guidelines [5]. All patients were treated with pulmonary artery vasodilators (beraprost 180 mg/day in 7 patients, sildenafil 60 mg/day in 4 patients). Right and left heart function were assessed before and 6 months after vasodilator treatment using transthoracic echocardiography.
Transthoracic echocardiography
Transthoracic echocardiography was performed and the images analyzed by two experienced echocardiographers using commercially available equipment (Vivid 7; GE Medical Systems, Horton, Norway). The measurements were performed according to the American Society of Echocardiography guidelines [6]. Left ventricular diastolic (LVDd) and systolic (LVDs) dimensions were measured using M-mode echocardiography. From the apical two- and four-chamber view, left ventricular end-diastolic (LVEDV) and end-systolic (LVESV) volumes were measured using a modified Simpson method and computer-assisted planimetry [7]. Left ventricular ejection fraction (LVEF) was calculated as (LVEDV − LVESV) × 100/LVEDV. Transmitral peak early diastolic filling (E) and peak atrial contraction (A) wave velocities were measured by means of continuous pulsed-wave Doppler from the apical windows aligning the ultrasound beam with the transvalvular mitral flow and sample between the tip of the valves, and E/A was calculated. Tricuspid regurgitation velocity (TRV) was measured from the highest peak velocity obtained with pulsed Doppler through the tricuspid valve using multiple views. Right ventricular systolic pressure (RVSP) was calculated from TRV and right atrial pressure (estimated by inspection of the inferior vena cava) using the modified Bernoulli equation [8]. Left ventricular outflow tract (LVOT) flow velocity and mitral valve (MV) inflow velocity were measured, and a velocity–time integral (VTI) was calculated for both LVOT outflow and MV inflow. Finally, early diastolic myocardial velocity at the medial mitral annulus (E′) was measured, using pulsed-wave tissue Doppler imaging [9].
Statistical analysis
Data are expressed as the mean ± SD. Since the data were normally distributed, the changes in parameters before and after treatment were assessed using a paired t test. The correlation between two parameters was assessed using simple linear regression. A P value of less than 0.05 was considered statistically significant.
Results
After 6 months of treatment with pulmonary artery vasodilators, RVSP decreased in 7 of the 11 patients enrolled, whereas it increased in the remaining 4. Overall, RVSP did not change significantly (69.3 ± 25.6 to 70.0 ± 30.3 mmHg) (Fig. 1). In addition, there were no significant changes in left ventricular functional parameters, including LVDd (43.6 ± 6.2 to 44.1 ± 5.5 mm), LVDs (26.4 ± 5.0 to 27.3 ± 5.0 mm), LVEF (68.9 ± 9.6 to 70.2 ± 7.8 %), LVOT-VTI (17.8 ± 3.8 to 19.3 ± 5.3 cm), MV-VTI (18.0 ± 6.3 to 18.0 ± 5.7 cm), E/A (0.78 ± 0.32 to 0.85 ± 0.23), and E′ (4.3 ± 1.5 to 4.9 ± 1.6 cm/s). There were also no significant changes in systolic (111.8 ± 16.9 to 106.6 ± 20.0 mmHg) and diastolic (69.6 ± 11.0 to 64.6 ± 12.3 mmHg) blood pressure (Table 1). In the assessment, where the patients were divided into two medication groups with beraprost (n = 7) and sildenafil (n = 4), there were no significant changes in RVSP (61.0 ± 23.1 to 59.4 ± 25.6, 83.8 ± 26.1 to 88.5 ± 32.2 mmHg in the beraprost and sildenafil groups, respectively), LVOT-VTI (18.6 ± 4.6 to 19.2 ± 6.1, 16.5 ± 1.7 to 19.5 ± 4.1 cm), MV-VTI (16.5 ± 6.1 to 17.4 ± 6.3, 20.6 ± 6.7 to 19.1 ± 5.1 cm), E/A (0.74 ± 0.31 to 0.87 ± 0.27, 0.84 ± 0.38 to 0.81 ± 0.17), and E′ (4.1 ± 1.0 to 4.7 ± 1.9, 4.7 ± 2.3 to 5.1 ± 0.7 cm/s) in both groups.

Change in right ventricular systolic pressure (RVSP) 6 months after pulmonary vasodilator treatment. The RVSP decreased in 7 of 11 patients (solid line), but increased in the remaining 4 (dotted line). Overall, the RVSP did not change significantly
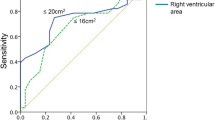
In patients overall, the percent change in LVOT-VTI correlated with the percent change in RVSP (r = −0.730, P = 0.011) (Fig. 2a). Furthermore, the percent change in MV-VTI also correlated with the percent change in RVSP (r = −0.621, P = 0.041) (Fig. 2b). However, there was no correlation between the percent change in RVSP and the percent changes in LVEF (r = −0.425, P = 0.192), LVDd (r = −0.052, P = 0.878), E/A (r = −0.352, P = 0.288), and systolic blood pressure (r = 0.263, P = 0.435). In addition, the percent change in E′ correlated with the percent change in RVSP (r = −0.675, P = 0.023) (Fig. 3).

a Relationship between the percent change in left ventricular outflow velocity–time integral (LVOT-VTI) and that in right ventricular systolic pressure (RVSP). b Relationship between the percent change in mitral valve inflow velocity–time integral (MV-VTI) and that in RVSP

Relationship between the percent change in early diastolic myocardial velocity at the medial mitral annulus (E′) and that in right ventricular systolic pressure (RVSP)
Discussion
In this study, we assessed left ventricular function in patients with pulmonary hypertension who received pulmonary artery vasodilator therapy. The major findings were that the relative changes in LVOT-VTI and MV-VTI after vasodilator treatment correlated with the relative change in RVSP. The relative change in E′ also correlated with the change in RVSP.
Stroke volume is expressed as a product of LVOT-VTI and left ventricular outflow area [10]. Since left ventricular outflow area was unchanged after vasodilator treatment, our finding of a correlation between the relative change in RVSP and that in LVOT-VTI suggests that right ventricular pressure load reduction by vasodilator treatment might increase stroke volume. In addition, stroke volume is determined by left ventricular systolic function, left ventricular afterload, and left ventricular preload [11]. Our results showed that the changes in LVEF, LVDd, and systolic blood pressure were not correlated with the change in RVSP. Nevertheless, the change in MV-VTI was correlated with the change in RVSP. Since the MV-VTI represents left ventricular filling volume [12], these findings suggest that right ventricular pressure load reduction by vasodilator treatment does not alter left ventricular systolic function and afterload, but rather increases left ventricular preload, resulting in an increase in stroke volume. In addition, the significant correlation between the change in RVSP and that in E′ strongly suggests that right ventricular pressure load reduction by vasodilator treatment might improve left ventricular diastolic function.
From our results, we can envision that pulmonary hypertension in the absence of left heart failure or congenital heart disease may affect left ventricular function, especially left ventricular diastolic function. Several possible mechanisms may be responsible for the effect of pulmonary hypertension on left ventricular diastolic function. Hypoxia, which often accompanies pulmonary hypertension, possibly induces left ventricular myocardial damage. Since hypoxia-induced left ventricular myocardial damage affects left ventricular diastolic function earlier than left ventricular systolic function [13], this interpretation is consistent with our results. However, we could not evaluate the relationship between changes in left ventricular functional parameters and the change in arterial oxygenation after pulmonary artery vasodilator treatment. Another possible mechanism is interaction between the right and left ventricles and biventricular adaptation to right ventricular pressure overload [14]. Right ventricular pressure overload produces right ventricular enlargement, which leads to left ventricular chamber distortion, as demonstrated by decreased LVEDV and abnormal left ventricular eccentricity [15]. These processes may impair left ventricular diastolic filling. Recently, Olson et al. [16] observed left ventricular strain and strain rate using two-dimensional speckle tracking in chronic thromboembolic pulmonary hypertension before and after pulmonary thromboendarterectomy. They reported that left ventricular circumferential and posterior wall radial strain improved after relief of pulmonary arterial obstruction, and suggested that the improved left ventricular strain might reflect improved left ventricular diastolic filling. Our results strongly suggest that the change in RVSP after pulmonary artery vasodilator treatment might produce a change in left ventricular diastolic function, as demonstrated by the change in E′. This may lead to a change in left ventricular filling as demonstrated by the change in MV-VTI, resulting in a change in stroke volume as demonstrated by the change in LVOT-VTI.
Potential limitations
The present study has several possible limitations. First, the study population was too small to evaluate pathophysiology. The etiology of pulmonary hypertension varied among patients and included idiopathic pulmonary artery hypertension, chronic thromboembolic pulmonary hypertension, pulmonary hypertension associated with collagen disease, and pulmonary hypertension associated with chronic obstructive pulmonary disease. However, this study included pulmonary hypertension caused only by pulmonary artery or pulmonary disease, and excluded cardiogenic pulmonary hypertension due to left heart failure or congenital heart disease. Therefore, we believe that we can comprehensively discuss the pathophysiology of pulmonary hypertension from the present results in this population. Second, we should assess local left ventricular performance during the diastolic phase to evaluate the mechanisms more precisely. In this study we assessed E′ as a parameter of left ventricular diastolic function, but medial E′ alone was used. Because medial E′ may be more influenced by right ventricular volume and pressure, simultaneous assessment of lateral E′ would be needed. Finally, despite pulmonary artery vasodilator treatment, RVSP increased in 4 of 11 patients and did not change significantly overall. These results indicate that the study population included patients with pulmonary hypertension refractory to treatment.
Conclusions
Our results suggest that left ventricular function, especially left ventricular diastolic function, may be affected by right ventricular pressure overload in patients with pulmonary hypertension. Future studies are necessary to determine whether left ventricular diastolic function could provide important prognostic information in pulmonary hypertension.
References
Natarajan R (2011) Recent trends in pulmonary arterial hypertension. Lung India 28:39–48
Sciomer S, Badagliacca R, Fedele F (2005) Pulmonary hypertension: echocardiographic assessment. Ital Heart J 10:840–845
Louie EK, Rich S, Brundage BH (1986) Doppler echocardiographic assessment of impairment left ventricular pressure overload due to primary pulmonary hypertension. J Am Coll Cardiol 8:1298–1306
Louie EK, Rich S, Vevitsky S, Brundage BH (1992) Doppler echocardiographic demonstration of the different effects of right ventricular pressure and volume overload on left ventricular geometry and filling. J Am Coll Cardiol 8:1298–1306
McGoon M, Gutterman D, Steen V, Barst R, McCrory DC, Fortin TA, Loyd JE (2004) Screening, early detection, and diagnosis of pulmonary arterial hypertension. ACCP evidence-based clinical practice guidelines. Chest 126:14S–34S
Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA (2002) Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr 15:167–184
Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I (1989) Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 2:358–367
Kircher BJ, Himelman RB, Schiller NB (1990) Non invasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol 66:493–496
Nagueh SF, Mikati I, Kopelen HA, Middleton KJ, Quiñones MA, Zoghbi WA (1998) Doppler estimation of left ventricular filling pressure in sinus tachycardia. A new application of tissue Doppler echocardiography in patients with pulmonary arterial hypertension. Circulation 98:1644–1650
Shahgaldi K, Manouras A, Brodin LA, Winter R (2010) Direct measurement of left ventricular outflow tract area using three dimensional echocardiography in biplane mode improves accuracy of stroke volume assessment. Echocardiography 9:1078–1085
Suga H, Igarashi Y, Yamada O, Goto Y (1985) Mechanical efficiency of the left ventricle as a function of preload, afterload, and contractility. Heart Vessels 1:3–8
Waggoner AD, De Las Fuentes MN, Gleva MJ, Spence KE, Davila-Roman VG (2008) Left ventricular diastolic filling prior to cardiac resynchronization therapy: implication for atrioventricular delay programming. Pacing Clin Electrophysiol 31:838–844
Ito A, Tomita H, Sano S (2009) Doppler echocardiographic assessment of left ventricular diastolic function in chronic hypoxic rats. Acta Med Okayama 63:87–96
Daniels LB, Krummen DE, Blanchard DG (2004) Echocardiography in pulmonary vascular disease. Cardiol Clin 22:383–399
Gurudevan SV, Malouf PJ, Auger WR, Waltmann TJ, Madani M, Raisinghani AB, DeMaria AN, Blanchard DG (2007) Abnormal left ventricular diastolic filling in chronic thromboembolic pulmonary hypertension: true diastolic dysfunction or left ventricular underfilling? J Am Coll Cardiol 49:1334–1339
Olson N, Brown JP, Kahn AM, Auger WR, Madani MM, Waltman TJ, Blanchard DG (2010) Left ventricular strain and strain rate by 2D speckle tracking in chronic thromboembolic pulmonary hypertension before and after pulmonary thromboendarterectomy. Cardiovasc Ultrasound 8:43
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amano, H., Toyoda, S., Arikawa, T. et al. Left ventricular function in pulmonary hypertension. Heart Vessels 28, 505–509 (2013). https://doi.org/10.1007/s00380-012-0272-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-012-0272-3