
Abstract
Purpose
The effect of overactive bladder (OAB) on sexual health has been evaluated extensively for women but much less for men. Therefore, the aim of this study was to evaluate the relationship between OAB and men’s sexual activity and the effect of OAB on erectile dysfunction (ED) and premature ejaculation (PE) in a large representative cohort of men at the population level.
Methods
This study was based on computer-assisted web interviews that used validated questionnaires. The most recent census and the sample size estimation calculations were employed to produce a population-representative pool.
Results
The study included 3001 men, representative of the population in terms of age and place of residence. The frequency of sexual intercourse was higher for respondents without OAB symptoms compared with persons who had OAB (p = 0.001), but there was no association between OAB symptoms and number of sexual partners (p = 0.754). Regression models did not confirm the effect of OAB on sexual activity (odds ratio 0.993, CI 0.974–1.013, p = 0.511). Both ED and PE were more prevalent in respondents with OAB symptoms compared with persons who lacked those symptoms (p < 0.001). Importantly, the effect of OAB on ED or PE was independent of age, comorbidities, and lifestyle habits (regression coefficients of 0.13 and 0.158 for ED and PE, respectively).
Conclusion
Overactive bladder did not significantly affect men’s sexual activity, but it significantly correlated with ED and PE. Our results suggest a need in daily clinical practice to screen for OAB symptoms for persons who report ED or PE.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Overactive bladder (OAB) is a highly bothersome condition that negatively affects the quality of life by impairing physical and social functioning, mental health, and work productivity [1].
The effect of OAB on sexuality has also been documented, and many studies have shown that OAB negatively affects women’s sexual health [2]. Balzarro et al., in their systematic review with meta-analysis, further confirmed that OAB was a risk for women’s sexual dysfunction [3]. However, the effect of OAB on men’s sexual health has received comparably less empirical attention. Only a few studies have shown that, because of urinary symptoms, OAB was significantly associated with reduced sexual activity and sexual enjoyment [4]. Even less is known about associations between OAB and erectile dysfunction (ED) and premature ejaculation (PE). Although many investigations demonstrated that ED and lower urinary tract symptoms (LUTS) often coexist, with odds ratio of ED among men who have LUTS ranging from 1.52 to 28.7 [5], there is a paucity of data on the effect of the subset of storage LUTS that define OAB. Whereas the close association between LUTS and men’s sexual dysfunctions is independent of age, comorbidities, and lifestyle factors [6], the effect of OAB on men’s sexual function has not been analysed to the same extent as that for LUTS.
Considering all the aforesaid factors, our understanding of the effect of OAB on sexual behaviour of men is limited [7]. Therefore, the aim of this study was to evaluate the relationship between OAB and men’s sexual activity and the effect of OAB on ED and PE in a large representative cohort of men at the population level. In addition, we analysed the sex-specific and overall quality of life of men who had ED with OAB or PE with OAB.
Methods
This study is an extension of ED POLAND, a population-based, representative, and cross-sectional investigation proposed to ascertain overall sexual health of Polish men [8]. The presented extension was designed and the data were analysed by members of the European Association of Urology Young Academic Urologists Working Group on Functional Urology. We followed standardized guidelines and well-established recommendations for reporting observational studies [9]. Our investigation was approved by the research ethics committee of Jagiellonian University Medical College, Krakow, Poland (1072.6120.331.2021); in addition, this study was registered with ClinicalTrials.gov (NCT05462171). All participants provided informed consent before entering this study.
Overall design
This inquiry was based on a computer-assisted web interview. The quota controls included age and place of residence. We used the most recent Polish population census (2021) to adequately assess the distribution of quota controls and to build a population-level sample of participants that represented the entire Polish population [10]. Our analysis included men aged at least 18 years and living in all geographical regions of Poland.
Data collection
Institut Public de Sondage d'Opinion Secteur (IPSOS), a research agency with relevant quality certificates (ESOMAR, PKJPA, PKJBI, OFBOR), distributed the survey.
Measures
For each respondent, we collected demographic data, including age, level of education, employment status, and marital status.
To assess sexual activity, we asked questions about frequency of sexual activity and number of sexual partners. These two questions were adapted from a nationally representative US survey, the General Social Survey [11]. The five-item International Index of Erectile Function (IIEF-5) [7, 12], the Premature Ejaculation Diagnostic Tool (PEDT) [7, 13], and the Overactive Bladder-Validated 8-question Screener (OAB-V8) [14, 15] were used to assess ED, PE, and OAB. These three questionnaires were rigorously translated and adapted into Polish [14, 16, 17], and they are discussed in the relevant guidelines of the European Association of Urology [7, 15].
Finally, we included questions on sex-specific and overall quality of life and relevant comorbidities and lifestyle habits. All questions and questionnaires with the scale-point thresholds for each questionnaire are presented in Online Resource 1.
Statistics
We used Kruskal–Wallis test for quantitative variables and chi-square test for qualitative variables. To analyse the effect of OAB on sexual activity, we used logistic regression models and presented results as odds ratios (ORs) with a 95% CI. To analyse the effect of OAB on ED and PE, we used linear regression models and presented results as regression coefficients with a 95% CI.
The sample size was calculated based on the population age distribution, available from the recent census [10], with the methodology that was used in other population-based studies of men’s sexual health [18]. We set the national sample size to 3000 respondents, which provided a 95% certainty that the survey results would be ± 1–2% of what they would have been had we polled the entire adult male Polish population.
A p-value less than 0.05 was considered to be statistically significant. R (The R Project for Statistical Computing, version 4.3.0, Austria) was used to conduct data analysis.
Results
Overall, 3001 men were surveyed, representative for age and place of residence. The response rate of our survey was 51.7%.
Effect of OAB on sexual activity
We found a significant correlation between OAB and frequency of sexual activity. Respondents without OAB had significantly higher frequency of sexual intercourse in the prior 12 months compared with individuals who had OAB (p = 0.001). Conversely, there was no association between OAB symptoms and number of sexual partners (p = 0.754). In addition, multivariate logistic regression did not demonstrate an effect of OAB on men’s sexual activity (OR 0.993, CI 0.974–1.013, p = 0.511).
Overall effect of OAB on ED and PE
Overactive bladder correlated well with ED. Erectile dysfunction was more prevalent for respondents with OAB symptoms compared with persons who lacked these symptoms (Spearman's Rank correlation coefficient R = − 0.37, p < 0.001, Online Resource 2). Using different cut-offs of IIEF-5, we also found positive correlations between ED and OAB (Spearman's Rank correlation coefficient R = − 0.35, p < 0.001, Online Resource 2).
Similarly, OAB correlated well with PE. Premature ejaculation was more prevalent for respondents with OAB compared with respondents without OAB (Spearman's Rank correlation coefficient R = 0.36, p < 0.001, Online Resource 2). Positive associations between PE and OAB were further found when we used different cut-offs of PEDT (Spearman's Rank correlation coefficient R = 0.27, p < 0.001, Online Resource 2).
Effect of OAB on ED and PE in age groups
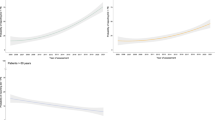
Univariate linear regression was used to measure the effect of OAB on ED and PE across age groups. When all age groups were combined, the relation between OAB and ED was statistically significant with a regression coefficient of -0.176 (Online Resource 3). The regression coefficients for all age groups were also statistically significant (Online Resource 3).
The same relation for OAB and PE was noticed, with a regression coefficient of 0.158 when participants from all age groups were combined (Online Resource 3). The regression coefficients for all different age groups were statistically significant (Online Resource 3).
Effect of OAB on ED and PE adjusted for age, comorbidities, and lifestyle habits
With multivariate linear regression, we found that the effect of OAB on ED and PE was independent of age, comorbidities, and lifestyle habits (Table 1). For ED, the regression coefficient was -0.13, i.e., an increase in the OAB-V8 score by 1 point entailed a decrease in the IIEF-5 score by an average of 0.13 points. For PE, the regression coefficient was 0.158, i.e., an increase in the OAB-V8 score by 1 point entailed an increase in the PEDT score by an average of 0.158 points.
Item analysis
We analysed which items of OAB-V8 had a negative effect on IIEF-5 and PEDT scores, and the results of this analysis are presented in Online Resource 4.
Effect on quality of life
Coexistence of OAB and ED or PE had negative effects on sex-specific quality of life. We found that respondents with OAB and ED or OAB and PE had worse sex-specific quality of life compared with the remaining participants (Online Resource 5).
We found similar results for OAB, ED, PE, and overall quality of life. Participants with OAB and ED or OAB and PE had worse overall quality of life compared with the other respondents (Online Resource 5).
Discussion
To the best of our knowledge, our study is the first complex population-representative analysis of effects of OAB on men’s sexual health that used widely accepted survey instruments for assessment of OAB, ED, and PE.
In our study, OAB did not significantly affect men’s sexual activity in terms of frequency of sexual intercourse and number of sexual partners. Conversely, OAB correlated well with ED and PE. Importantly, the relations between OAB and ED or OAB and PE were independent of age, comorbidities, and lifestyle habits. Finally, respondents with OAB and ED or OAB and PE had worse sex-specific and overall quality of life compared with the other respondents.
Many analyses showed that the prevalence of ED was greater for men with LUTS than for men without LUTS [5, 6]; however, only a limited number of studies have focused on connections between OAB and ED. In 2008, Irwin et al. presented a secondary investigation of the EPIC study that analysed the prevalence of self-reported ED (of note, ED was assessed with a single question) in men with OAB (n = 502) vs. controls (n = 502) [4]. The authors showed that respondents with OAB were significantly more likely than controls to report ED (prevalence OR 1.5; 95% CI 1.1–2.2). In 2011, Coyne et al. further analysed the data from the EpiLUTS study and demonstrated that OAB was a significant predictor of ED (of note, ED was assessed with the Erectile Function domain of the IIEF) with OR of 2.00 or 2.24 depending on the OAB definition [19]. The effect of OAB on ED was also analysed in some patient populations. For instance, the presence of severe ED was significantly associated with OAB for patients with diabetes (correlation coefficient 0.275) [20]. Therefore, our results further support the concept that OAB and ED are closely correlated. In addition, we confirmed that the OAB–ED relation was independent of multiple covariates.
The correlations between OAB and PE have been analysed to an even smaller degree compared with OAB and ED. Until now, only one study was conducted to assess the connection between OAB and PE, i.e., a secondary analysis of EpiLUTS performed by Coyne et al. [19]. Although rates of PE in the EpiLUTS study were higher for participants with OAB compared with persons who lacked this syndrome, regression models failed to demonstrate OAB as a significant predictor of PE [19]. Notably, to assess PE, the investigators used only a single-item self-reported question about control of ejaculation. Here, we need to underline that there is lack of a universally accepted and clear definition of PE; therefore, current diagnostic criteria are variable and are largely based on subjective measurements [7]. Because a person’s perception of PE is often subjective and highly individual, validated screening instruments that include relevant symptom burden of the disease are the optimal method to use in population-based analyses [7]. Therefore, we decided to use the PEDT, an instrument with high specificity and sensitivity in identifying PE [7]. In addition, its validity has been widely accepted in estimating PE prevalence in other large population-based analyses [7, 21]. Therefore, in our study that was based on reliable instruments for OAB and PE assessment, we found that OAB correlated significantly with PE, and the effect of OAB on PE was independent of age, comorbidities, and lifestyle habits.
We confirmed the negative effect of coexisting OAB and ED or OAB and PE on sex-specific and overall quality of life. Respondents with coexisting conditions had worse sex-specific and overall quality of life compared with unaffected respondents. Many studies demonstrated that men with independent OAB, ED, and PE experience a deterioration in psychological, social, physical, and economic well-being compared with men who do not have these conditions [7]. Therefore, the results of our study may suggest the need for screening for OAB symptoms with persons who report ED or PE. Because we showed that OAB had negative effects on both ED and PE, it may be justified to simply ask patients with ED and PE about bothersome storage LUTS. However, it is not known whether treatment specific for OAB will have an effect on management of ED and PE. Nevertheless, some recent interesting pilot data (n = 20) suggest that pharmacological treatment of OAB with beta-3 agonists may improve erectile function of men with concurrent/concomitant OAB and ED [22]. In a small (n = 54) longitudinal study, Lombardi et al. reported similar positive effects of OAB treatment with sacral neuromodulation on erectile function [23]. Clearly more research is warranted to evaluate the effects of treatments for OAB on various domains of men’s sexual health, for ED and PE in particular.
Our regression models did not confirm the negative effect of OAB on men’s sexual activity. This finding might be in contrast to other studies that showed OAB as a negative factor for the frequency of men’s sexual intercourse. In their population-level analysis, Irwin et al. showed that a significantly greater percentage of persons with OAB reported that urinary symptoms caused them to decrease or cease sexual activity [4]. However, the authors did not use regression models to confirm the finding. Heidler et al. and Yoo et al. presented similar results, also without validation with regression models [24, 25]. In contrast, Coyne et al. confirmed with both univariate and multivariate analyses that OAB was predictive of decreased sexual activity of men [19]. Therefore, we can hypothesize that the association between men’s sexual activity and OAB is more complex than one would expect, and the underlying mechanisms are not completely understood.
Our study was limited mainly by the use of self-reports to measure OAB. Even reliance on the validated OAB screening tool (OAB-V8) does not enable exclusion of storage symptoms secondary to other conditions unrelated to OAB. However, recent epidemiological analyses on OAB have been based mostly on validated OAB screening instruments [26, 27] and these instruments are considered as optimal for population-based analyses [28]. We could not also confirm by clinical diagnosis any of the other outcomes including sexual dysfunctions, an acknowledged information bias of population-based self-reporting.
Conclusions
This investigation was the first population-representative study of the effect of OAB on men’s sexual health, including the effect of OAB on sexual activity, ED, and PE, that used reliable instruments. OAB did not significantly affect men’s sexual activity, but OAB correlated well with ED or PE. In addition, the relations between OAB and ED or OAB and PE were independent of age, comorbidities, and lifestyle habits. Finally, respondents with OAB and ED or OAB and PE had worse sex-specific and overall quality of life compared with the other respondents. Because OAB, ED, and PE significantly affect overall well-being, we suggest that screening for OAB symptoms of patients who report ED or PE should be considered in daily clinical practice.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- ED:
-
Erectile dysfunction
- IIEF-5:
-
The 5-item International Index of Erectile Function
- LUTS:
-
Lower urinary tract symptoms
- OAB:
-
Overactive bladder
- OAB-V8:
-
Overactive Bladder-Validated 8-question Screener
- OR:
-
Odds ratio
- PE:
-
Premature ejaculation
- PEDT:
-
Premature Ejaculation Diagnostic Tool
References
Coyne KS, Sexton CC, Kopp ZS et al (2011) The impact of overactive bladder on mental health, work productivity and health-related quality of life in the UK and Sweden: results from EpiLUTS. BJU Int 108:1459–1471
Coyne KS, Margolis MK, Jumadilova Z et al (2007) Overactive bladder and women’s sexual health: what is the impact? J Sex Med 4:656–666
Balzarro M, Rubilotta E, Mancini V et al (2019) Impact of overactive bladder-wet syndrome on female sexual function: a systematic review and meta-analysis. Sex Med Rev 7:565–574
Irwin DE, Milsom I, Reilly K et al (2008) Overactive bladder is associated with erectile dysfunction and reduced sexual quality of life in men. J Sex Med 5:2904–2910
Seftel AD, de la Rosette J, Birt J et al (2013) Coexisting lower urinary tract symptoms and erectile dysfunction: a systematic review of epidemiological data. Int J Clin Pract 67:32–45
Rosen R, Altwein J, Boyle P et al (2003) Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol 44:637–649
European Association of Urology (EAU), Non-Oncology Guidelines [Internet]; Sexual and Reproductive Health, Publicated: 2023 https://uroweb.org/guidelines/sexual-and-reproductive-health. Accessed Jun 2023.
Przydacz M, Chlosta M, Rajwa P, Chlosta P (2023) Population-level prevalence, effect on quality of life, and treatment behavior for erectile dysfunction and premature ejaculation in Poland. Sci Rep 13:13168
von Elm E, Altman DG, Egger M et al (2014) The strengthening the reporting of observational studies in epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg 12:1495–1499
Glowny Urzad Statystyczny (GUS), Narodowe Spisy Powszechne [Internet]; Publicated: 2021 [Cited: 2023 June]. https://stat.gov.pl/spisy-powszechne/. Accessed Jun 2023.
Ueda P, Mercer CH, Ghaznavi C, Herbenick D (2020) Trends in frequency of sexual activity and number of sexual partners among adults aged 18 to 44 years in the US, 2000–2018. JAMA Netw Open 3:e203833
Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM (1999) Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res 11:319–326
Symonds T, Perelman MA, Althof S et al (2007) Development and validation of a premature ejaculation diagnostic tool. Eur Urol 52:565–573
Coyne KS, Zyczynski T, Margolis MK, Elinoff V, Roberts RG (2005) Validation of an overactive bladder awareness tool for use in primary care settings. Adv Ther 22:381–394
European Association of Urology (EAU), Non-Oncology Guidelines [Internet]; Non-neurogenic Female LUTS, Publicated: 2023. https://uroweb.org/guidelines/non-neurogenic-female-luts. Accessed Jun 2023.
Przydacz M, Chlosta M, Zembrzuski M, Wiatr T, Chlosta P (2022) Polish translation and cross-cultural adaptation of the five-item International Index of Erectile Function. Cent European J Urol 75:216–219
Symonds T, Perelman M, Althof S et al (2007) Further evidence of the reliability and validity of the premature ejaculation diagnostic tool. Int J Impot Res 19:521–525
Chen KK, Chiang HS, Jiann BP et al (2004) Prevalence of erectile dysfunction and impacts on sexual activity and self-reported intercourse satisfaction in men older than 40 years in Taiwan. Int J Impot Res 16:249–255
Coyne KS, Sexton CC, Thompson C et al (2011) The impact of OAB on sexual health in men and women: results from EpiLUTS. J Sex Med 8:1603–1615
Liu RT, Chung MS, Chuang YC et al (2012) The presence of overactive bladder wet increased the risk and severity of erectile dysfunction in men with type 2 diabetes. J Sex Med 9:1913–1922
Shaeer O (2013) The global online sexuality survey (GOSS): The United States of America in 2011 Chapter III–Premature ejaculation among English-speaking male Internet users. J Sex Med 10:1882–1888
Karakus S, Musicki B, Burnett AL (2022) Mirabegron improves erectile function in men with overactive bladder and erectile dysfunction: a 12-week pilot study. Int J Impot Res 34:588–592
Lombardi G, Mondaini N, Giubilei G et al (2008) Sacral neuromodulation for lower urinary tract dysfunction and impact on erectile function. J Sex Med 5:2135–2140
Heidler S, Mert C, Wehrberger C et al (2010) Impact of overactive bladder symptoms on sexuality in both sexes. Urol Int 85:443–446
Yoo ES, Kim BS, Kim DY, Oh SJ, Kim JC (2011) The impact of overactive bladder on health-related quality of life, sexual life and psychological health in Korea. Int Neurourol J 15:143–151
Przydacz M, Golabek T, Dudek P, Lipinski M, Chlosta P (2020) Prevalence and bother of lower urinary tract symptoms and overactive bladder in Poland, an Eastern European Study. Sci Rep 10:19819
Soler R, Gomes CM, Averbeck MA, Koyama M (2018) The prevalence of lower urinary tract symptoms (LUTS) in Brazil: Results from the epidemiology of LUTS (Brazil LUTS) study. Neurourol Urodyn 37:1356–1364
Llorente C (2010) New concepts in epidemiology of lower urinary tract symptoms in men. Eur Urol Suppl 9:477–481
Acknowledgements
The authors thank study participants for their time.
Funding
This study was supported by unrestricted grants from the Jagiellonian University Medical College and Polpharma Pharmaceuticals. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors’ work was independent of the funders.
Author information
Authors and Affiliations
Contributions
MP, NO, SDC, CGT, FH, TH, EI, ATF, MT, LV, MC, FC, SD, PG, NR, HBG, PC, and VP were involved in conceptualization, investigation, methodology, and writing—review & editing. MP performed formal analysis, project administration, supervision, validation, visualization, and writing—original draft. MP and PC did funding acquisition and provided resources.
Corresponding author
Ethics declarations
Conflicts of interest
The authors have nothing to disclose.
Ethical approval
This study was performed in compliance with Good Clinical Practice and in accordance with the Declaration of Helsinki. The research ethics committee of Jagiellonian University Medical College, Krakow, Poland approved this study (1072.6120.331.2021); in addition, this study was registered with ClinicalTrials.gov (NCT05462171). Informed consent was provided by all participants.
Informed consent
All participants provided informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Przydacz, M., Osman, N., De Cillis, S. et al. Overactive bladder negatively affects erectile function and promotes premature ejaculation: findings from large representative population-level study. World J Urol 42, 139 (2024). https://doi.org/10.1007/s00345-024-04841-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00345-024-04841-5