
Abstract
Objectives
The objective of this study was to investigate the effect of location and number of anomalously connected pulmonary veins and any associated atrial septal defect (ASD) on the magnitude of left-to-right shunting in patients with partial anomalous pulmonary venous connection (PAPVC), and how that influences right ventricular volume loading.
Methods and results
The cardiac magnetic resonance (CMR) and echocardiography examinations of 26 paediatric patients (mean age, 11.2 ± 5.1 years) with unrepaired PAPVC were analysed. Fourteen patients had right-sided, 11 left-sided and 1 patient bilateral PAPVC. An ASD was present in 11 patients, of which none had a Qp/Qs < 1.5 and 8 had a Qp/Qs≥ 2.0. No patient with isolated left upper PAPVC experienced a Qp/Qs ≥ 2.0 compared to 9/12 patients with right upper PAPVC. Qp/Qs correlated with indexed right ventricle (RV) end-diastolic volume (RVEDVi, r = 0.59, p = 0.002) by CMR and with echocardiographic right ventricular end-diastolic dimension (RVED) z-score (r = 0.68, p = 0.003). A RVEDVi >124 ml/m2 by CMR and a RVED z-score >2.2 by echocardiography identified patients with a Qp/Qs ≥1.5 with good sensitivity and specificity.
Conclusions
An asymptomatic patient with a single anomalously connected left upper pulmonary vein and without an ASD is unlikely to have a significant left-to-right shunt. On the other hand, right-sided PAPVC is frequently associated with a significant left-to-right shunt, especially when an ASD is present.
Key Points
• Patients with PAPVC and ASD routinely have a significant left-to-right shunt.
• Patients with right PAPVC are likely to have a significant left-to-right shunt.
• Patients with left PAPVC are unlikely to have a significant left-to-right shunt.
• CMR is helpful in decision-making for patients with PAPVC.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In partial anomalous pulmonary venous connection (PAPVC), one or more, but not all, of the pulmonary veins connect to one of the systemic veins or to directly to the right atrium [1,2,3]. Patients with this condition exhibit varying degrees of right atrial and ventricular volume overload as a result of left-to-right shunting at the pulmonary venous and, in many cases, also the atrial level. Factors that influence the degree of left-to-right shunting include the number of anomalously connected pulmonary veins, the presence and size of any atrial septal defect (ASD), and the compliance of the right ventricle (RV) [3, 4]. The decision for surgical repair of PAPVC ± ASD depends on symptoms, shunt magnitude and degree of right ventricular dilatation. A pulmonary (Qp) to systemic flow (Qs) ratio (Qp/Qs) ≥1.5 is widely used as a criterion for the operative repair of simple left-to-right shunt lesions, including ASDs and PAPVC [5, 6].
Previous reports on the haemodynamics in patients with PAPVC were based on cardiac catheterisation and included assumptions about the relative contribution of each pulmonary vein to the total pulmonary venous blood flow. These techniques could not measure flow in the individual pulmonary veins or determine the relative contribution of multiple levels of left-to-right shunting to the total shunt. Knowing the amount of left-to-right shunting that anomalous pulmonary vein with or without an ASD produces impacts therapeutic decision-making. For example, a patient with a minor left-to-right shunt is treated conservatively, a patient with a secundum type ASD and single vein PAPVC may be best served with percutaneous closure of the ASD, while patients with significant left-to-right shunting from PAPVC require surgery [7, 8]. Today’s “gold standard” for flow quantification is phase contrast cardiac magnetic resonance imaging (PC CMR), allowing for flow assessments in each individual pulmonary vein as well as across the atrial septum [9,10,11,12].
The objective of this study was to investigate the effect of location and number of anomalously connected pulmonary veins and any associated ASD on the magnitude of left-to-right shunting in patients with PAPVC, and to determine the effect of left-to-right shunting on right ventricular volume loading.
Methods
Ethics, consent and permission: approval was granted by our institutional research ethics board (protocol number 1000016804) and the need for consent was waived for this retrospective study.
We performed a retrospective analysis of all CMR studies obtained on patients with unrepaired PAPVC between January 2003 and January 2010. Patients with Scimitar syndrome or congenital heart disease other than PAPVC or atrial communications were excluded. All CMR studies were obtained on one of two magnets: prior to 2007, a 1.5-T Signa CV/I system (GE Medical Systems, Little Chalfont, UK) was used. Thereafter, the examinations were performed on a 1.5-T Avanto magnet (Siemens Healthineers, Erlangen, Germany). The standard clinical CMR protocol at our hospital includes cine imaging in short axis for ventricular volumetry and phase-contrast velocity mapping of the ascending and descending aorta, superior and inferior caval veins, right (RPA) and left branch pulmonary arteries (LPA) and of the individual pulmonary veins, including the anomalously connected vein(s). Following the principle of flow conservation, net flows were measured throughout. The acquisition parameters of these standard imaging tools are reported elsewhere [12, 13]. Commercially available software (QFlow, version 5.1 and QMass version 7.1; MEDIS Medical Imaging Systems, Leiden, The Netherlands) was used for quantification of flow and ventricular volumes. The analysis was performed according to a standardised post processing algorithm, using uniform settings. When the anomalous pulmonary venous flow rate could not be directly measured because of complex pulmonary venous anatomy it was calculated by subtracting the flow volume in the normally draining pulmonary vein(s) on the same side from the ipsilateral arterial flow volume. In patients with an ASD, the left-to-right shunt across the ASD [Q(ASD)] [14] was calculated by subtracting the flow in the anomalously connecting pulmonary vein(s) from the total left-to-right shunt (Qp minus Qs, below). The pulmonary to systemic flow ratio (Qp/Qs) was calculated by dividing the total pulmonary arterial flow (Qp) by the systemic blood flow (Qs). The systemic blood flow was determined by measuring the flow in the ascending aorta.
In summary, the following equations were used:
In normal anatomy, but particularly in PAPVC, there is considerable variability in the anatomy of the connection of the pulmonary veins to the left atrium, particularly on the right side. In cases with right-sided PAPVC, the right upper (RUPV) and right middle pulmonary vein (RMPV) often connect in a complex fashion to the superior vena cava (SVC) or right atrium (RA) (Fig. 1). Consequently, it is often difficult to determine whether there is a separate RMPV [15, 16]. For the purpose of this study, flow in an anomalously draining RMPV (if present) was added to the RUPV flow. Right ventricular end-diastolic dimensions (RVEDd) were retrieved from the echocardiogram closest to CMR and converted to z-scores.

Anomalous connection of the left and right upper pulmonary veins. Volume-rendered reconstructions of contrast-enhanced three-dimensional magnetic resonance data sets in a an 8-year-old girl with anomalous connection of the left upper pulmonary vein to the innominate vein and b in a 9-year-old boy with anomalous connection of the right upper pulmonary vein to the right superior vena cava. The right lower and the left pulmonary veins drain normally (ao aorta, a.v. azygos vein, i.v. innominate vein, RPA right pulmonary artery, RUPV right upper pulmonary vein, SVC superior vena cava)
The echocardiogram performed closest to the date of the CMR, before surgical correction but within 12 months of the CMR, was reviewed. As per our institution’s clinical protocol, chamber diameters were measured according to established guidelines and were standardised to the body surface area as z-scores on the basis of published normative data [17,18,19,20].
Statistical analysis
Demographics and biological results are presented as mean ± SD. Parametric unpaired two-tailed Student t-tests using Microsoft Excel 2003 with SSC-Stat 2.12 add-on software package (Statistical Services Centre, University of Reading, Reading, UK) were used to compare results between different patient groups. Linear regression was performed to assess for associations between variables. Results with a p value <0.05 were considered significant.
Results
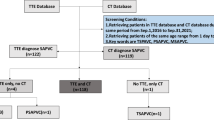
Twenty-eight patients with PAPVC had undergone a CMR during the reviewed time period. Two patients were excluded, one for significant additional congenital heart disease (Shone’s complex), and another due to Scimitar syndrome. In the remaining 26 patients, PAPVC was newly diagnosed or a suspected diagnosis confirmed by CMR in 9 patients (34.6%). The other 17 patients had a known diagnosis of PAPVC and were referred for assessment of Qp/Qs and right ventricular volumes. The demographic information is summarised in Table 1. The anomalous pulmonary blood flow volume had been measured directly in 11 patients (42.3%). It had been calculated in nine patients (branch pulmonary arterial flow minus ipsilateral regularly draining veins) and had not been obtained in five patients; in one patient with total anomalous right-sided pulmonary venous connection the right upper vein was stenotic, precluding accurate flow measurement. Eighteen patients (69.2%) had echocardiograms suitable for analysis, with a duration between echocardiography and the CMRI of 4.7 ± 3.0 months (0–10 months). The remaining eight did not have an echocardiogram within 12 months of the CMRI.
Fourteen patients (53.8%) had right-sided PAPVC and 11 (42.3%) had left-sided PAPVC. One patient had bilateral PAPVC with the RUPV, RMPV and the left upper pulmonary vein (LUPV) draining anomalously to the SVC. There were two (non-Scimitar) patients in whom all the right pulmonary veins drained anomalously, including the patient with bilateral PAPVC mentioned above. An ASD was found in 11 patients (42.3%), of which 9 (81.8%) had an anomalously connected RUPV (± RMPV), and 2 (18.2%) had an anomalously connected LUPV (connected to the innominate vein). The ASD in patients with right-sided PAPVC was of the sinus venosus type while the two patients with left-sided PAPVC had a secundum ASD.
Haemodynamic results are shown in Table 1, including a comparison between patients with and without an atrial communication. Out of 11 patients with an ASD none had a Qp/Qs < 1.8, and eight (72.7%) had a Qp/Qs ≥ 2.0. Of the 15 patients without an atrial communication, five (33.3%) had a Qp/Qs ≥ 1.5 and only 1 had a Qp/Qs ≥ 2.0 (2.9). There were no readily apparent features that explained the higher Qp/Qs in this patient. In patients with an atrial communication, the mean calculated left-to-right shunt due to the ASD alone (total shunt minus PAPVC shunt, Eq 4) was 2.34 ± 1.55 l/min/m2 (0.40–5.07), corresponding to 51.2 ± 19.8% (21.1–79.0) of the total shunt. In this subgroup without ASD, patients with PAPVC of the RUPV showed trends towards a higher Qp/Qs (1.90 ± 0.38 vs 1.47 ± 0.24) and larger RVEDVi (171 ± 65 ml/m2 vs 124 ± 32 ml/m2) compared towards PAPVC or the LUPV. The highest Qp/Qs in patients with isolated PAPVC of either the RUPV or the LUPV were 2.34 and 1.90, respectively. These differences were not significant, possibly because of the small group of only three patients with anomalous RUPV who did not have an atrial level shunt. Table 2 compares patients with PAPVC of the RUPV to those with PAPVC of the LUPV, irrespective of the presence of an ASD. Patients with PAPVC of the RUPV had a greater Qp/Qs (2.48 ± 0.73 vs 1.51 ± 0.23, p = 0.0004), larger RVEDVi (160 ± 37 ml/m2 vs 124 ± 28 ml/m2, p = 0.009) and smaller LVEDVi (68 ± 18 ml/m2 vs 88 ± 22 ml/m2, p = 0.008). However, they were also more likely to have an associated atrial communication (p = 0.01). No patient with PAPVC of the LUPV had a Qp/Qs ≥ 2.0, and 5 (45.5%) had a Qp/Qs ≥ 1.5. Of the patients with an anomalous RUPV (±RMPV), all had a Qp/Qs ≥ 1.5 and nine (75.0%) had a Qp/Qs ≥ 2.0.
Qp/Qs correlated with indexed right ventricular end-diastolic volume (RVEDVi, r = 0.59, p = 0.002, Fig. 2). A RVEDVi of 124 ml/m2 separated patients with a Qp/Qs ≥1.5 from those with a Qp/Qs <1.5 with an area under the receiver operating characteristic (ROC) curve of 0.84 (95% CI, 0.66-1.0; sensitivity, 88%; specificity, 67%; Fig. 3). RVEDd z-score by echocardiography correlated with RVEDVi by CMR (r = 0.72, p = 0.002, Fig. 4). Qp/Qs correlated with the RV end-diastolic dimension (RVED) z-score by echocardiography (r = 0.68, p = 0.003). Right ventricular ED z-score of 2.2 predicted a Qp/Qs ≥ 1.5 with an area under the ROC curve was of 0.96 (95% CI, 0.87-1.0; Fig. 3), a sensitivity of 100% and a specificity of 75%.

Right ventricular volume overload as a result of a left-to-right shunt. Right ventricular end-diastolic volume, indexed to body surface area (RVEDVi), versus pulmonary to systemic blood flow ratio (Qp/Qs)

Prediction of a significant left-to-right shunt (Qp/Qs of 1.5 or greater) by right ventricular volume and diameter. ROC curves for right ventricular end-diastolic volume by CMR, indexed to body surface area (RVEDVi) and right ventricular end-diastolic dimension z-scores (RVEDd z-score) by echocardiography

Agreement of right ventricular volume by CMR and diameter by echocardiography. Right ventricular end-diastolic volume by cardiac magnetic resonance, indexed to body surface area (RVEDVi) plotted against right ventricular end-diastolic dimension z-scores (RVEDd z-score) by echocardiography
Qp/Qs correlated inversely with indexed left ventricular end-diastolic volume (LVEDVi, r = -0.50, p = 0.01). Patients with a Qp/Qs ≥1.5 had a lower stroke volume index (42 ± 13 ml/m2 vs 51 ± 12 ml/m2, p = 0.06).
In patients with PAPVC of the RUPV (excluding the two patients with PAPVC or the RUPV and the RLPV), but without an atrial communication, the Qp/Qs and RVEDVi ranged from 1.64 to 2.34 and from 126 to 245 ml/m2, respectively. In LUPV PAPVC the Qp/Qs and RVEDVi ranges were 1.22-1.90 and 93-188 ml/m2, respectively.
In order to test whether an anomalous connection changed the amount of blood flow to the lung with the anomalous drainage, the perfusion of each lung was expressed as a percentage of the total pulmonary blood flow (TPBF) and compared to previously published data by our group in healthy adult volunteers [12]. In patients with anomalous connection of the LUPV (with or without an ASD), the relative blood flow to the left lung was 44.9 ± 3.6% (39.3–50.0%) of TPBF, compared to 46.6 ± 2.3% (42.4–49.5%) of TPBF in controls (p = 0.32). In patients with RUPV ± RMPV PAPVC, the measured right lung blood flow was 57.4 ± 5.1% (51.6–70.5%) of TPBF, versus 53.4 ± 2.3% (50.5–57.6%) in controls (p = 0.02).
Discussion
Although generally regarded as a relatively benign lesion, the natural history of PAPVC is not favourable in all cases. Anecdotal case reports of patients developing pulmonary vascular disease in the affected lung lobe in the presence of only one anomalously draining pulmonary vein document the potential risk of pulmonary hypertension in these patients [21, 22]. The goal of surgical correction of PAPVC is to alleviate complications associated with chronic right heart volume overload, including heart failure and atrial arrhythmias, and to prevent irreversible pulmonary vascular changes [3, 4, 23]. On the other hand, rerouting of the pulmonary veins carries the risk of postoperative pulmonary vein stenosis, sinus node dysfunction and atrial arrhythmias so that unnecessary surgery must be avoided [24,25,26,27,28].
In a symptomatic patient with PAPVC the decision to operate is usually straightforward, but difficulty arises when this lesion is diagnosed in asymptomatic patients. Current diagnostic tools like echocardiography and CMR, which are performed for reasons other than a possible atrial level shunt, occasionally identify patients with PAPVC which would previously have gone undiagnosed.
With this scenario of surgical decision-making in mind, the main findings of our paper are:
-
1.
An asymptomatic patient with isolated anomalous connection of the LUPV without an ASD is unlikely to have a significant left-to-right shunt, and typically does not require surgery on the basis of Qp/Qs and RV volume load.
-
2.
On the other hand, the combination of right-sided PAPVC with ASD is routinely associated with a significant left-to-right shunt.
-
3.
Even an isolated anomalously draining RUPV in the absence of an ASD can lead to a significant left-to-right shunt.
-
4.
RVED z-score by echocardiography is helpful in identifying patients with a significant Qp/Qs on the basis of RV enlargement.
Much of what is known about haemodynamics in PAPVC is based on a study by Alpert et al. [7] in a series of 21 patients with isolated PAPVC between 14 and 53 years of age. Using invasive oximetry as well as indicator dilution techniques and incorporating previously published estimates of flow distribution among the lung lobes by Bryan and co-workers [14], they postulated that the flow to the lung with the anomalously connected vein(s) is higher than in individuals with normally connected pulmonary veins. The present study, using CMR measurements, confirms Alpert et al.’s findings, at least on the right [7]. They hypothesised that the anomalously connecting veins carry more blood flow than normal because they drain into a lower pressure system: the mean right atrial pressure is lower than on the left, resulting in a greater pressure gradient across the anomalously draining lung segments and, presumably, preferential pulmonary blood flow to these segments.
Right-sided, but not left-sided, PAPVC led to an increase in flow to the ipsilateral lung, at least when an ASD was present [34, 35]. This is in keeping with a historical study by Dollery and colleagues [36], who found mildly, but significantly, increased right-sided pulmonary blood flow in patients with ASDs. The explanation that has been offered for this phenomenon is that in secundum type ASDs the RUPV streams across the atrial communication into the lower pressure right atrium, while the left-sided pulmonary veins stream to the left atrium, even in the presence of an ASD.
In patients with an ASD and / or PAPVC a significant left-to-right shunt often, although not without debate, defined as a Qp/Qs ≥ 1.5, and represents one of the criteria for intervention [6, 29]. Previously, cardiac catheterisation was required to determine the magnitude of a left-to-right shunt [30]. CMR-derived shunt quantification has been shown to correlate very closely with invasive oximetry in a number of shunt lesions [31]. Specifically, Festa et al. [32] compared the Qp/Qs obtained during cardiac catheterisation and CMR in patients with PAPVC and found excellent agreement, concluding that diagnostic cardiac catheterisation is not routinely required in this condition. We previously demonstrated that flow measurements in the pulmonary veins, using phase contrast velocity mapping CMR, are accurate and can be used to quantify complex extra-cardiac left-to-right shunts [11, 12, 33]. CMR, contrary to invasive oximetry, allows to differentiate between the left-to-right shunt via the anomalously connected pulmonary vein(s) and an ASD, if present. Clinically, we previously encountered a case of PAPVC of the LUPV and secundum type ASD. The differential shunt calculation led to a decision to close the ASD percutaneously and to not intervene on the anomalous vein. Our results indicate patients with isolated PAPVC of the LUPV are unlikely to have a significant left-to-right shunt: no patient with an anomalous LUPV had a Qp/Qs ≥ 2.0, so that surgery (and, likely, CMR) can often be avoided in this group, although larger studies are necessary to confirm this early finding. In contrast, patients with PAPVC of the RUPV may develop an important left-to-right shunt. The reason for the smaller left-to-right shunt in left-sided versus right-sided PAPVC is likely related to a larger volume of lung drained by the RUPV (± RMPV) than by the LUPV: the territory drained by the RUPV (and RMPV if present), grossly corresponding to the upper and middle lobes, is larger than that drained by the LUPV, i.e. approximately the left upper lobe including the lingula segment. This size discrepancy is mostly due to volume in the left hemithorax that is occupied by the heart. Another, probably less important explanation for lower Qp/Qs in left compared to right-sided PAPVC is that an anomalously draining left pulmonary vein typically drains into the on the innominate vein, remote from the RA. This may result in a slightly lower transpulmonary gradient in left-sided PAPVC, perhaps limiting flow through the anomalous vein. When an atrial communication is present, most often in the form of a sinus venosus ASD, associated with PAPVC of the RUPV, the shunt is nearly always significant.
Although RV dilatation is the result of a significant left-to-right shunt, the association between either RVEDVi by CMR or RVED z-score by echocardiography and Qp/Qs was loose. There must, therefore, be other factors precipitating RV dilatation in certain patients, including RV compliance and perhaps interactions between the RV and LV. Interestingly, Qp/Qs was inversely correlated with the LVEDVi, presumably due to compression by the volume loaded RV and, possibly, underfilling, similar to what is routinely observed in patients with total anomalous pulmonary venous connection. In 1975, Laurenceau et al. [38] found a strong correlation between indexed RV diameter and Qp/Qs. Prior to the widespread availability of CMR, echocardiographic measurements of RV and right atrial size predicted a Qp/Qs > 1.5 with 96% sensitivity and 94% specificity [37]. Interestingly, the ability of echocardiographic RVED z-score to predict a Qp/Qs ≥ 1.5 exceeded that of RVEDVi by CMR. This observation is counterintuitive and needs to be tested in larger studies. If confirmed it suggests that the RV diameter at the base is more reflective of the degree of volume loading through a supraventricular shunt than a three-dimensional assessment by CMR that also takes into account other regions of the RV which may not be affected to similar degrees by the volume-loading. Based on our findings, RVED z-scores may be a suitable screening tool for RV enlargement, despite an only modest correlation with RVEDVi by CMR, similar to previous reports [19, 39, 40].
Limitations
Some, but not all, patients had a separate RMPV. Typically, an RMPV, when present, connects close to the mouth of the RUPV: at the level of the SVC/right atrial junction if anomalous and to the high left atrium when if normally connected. Therefore, and to overcome the challenge during analysis from this anatomical variability, we regarded a separately connecting RMPV as a branch of the RUPV. A further limitation was the small sample size, which may have obscured additional associations or differences. There was likely a referral bias in this retrospectively studied cohort as it depended on the managing physician to decide if a CMR was indicated. However, since the objective of this study was not to determine prevalence and incidence, the impact of this referral bias is thought to be limited.
Conclusions
Patients with isolated PAPVC of the LUPV are unlikely to have a surgically important left-to-right shunt, especially in the presence of normal RV dimensions by echocardiography. These patients do not benefit from routine haemodynamic assessment by CMR. Patients with PAPVC of the RUPV and ASD usually have a significant left-to-right shunt and the surgical indication can typically be made on the basis of echocardiography and/or symptoms. These patients also benefit little from routine CMR, except for the delineation of anatomy. In borderline candidates for surgical repair of PAPVC, especially in cases with isolated PAPVC of the RUPV, the combination of an accurate assessment of the pulmonary venous anatomy, quantification of Qp/Qs and of right ventricular dilatation makes cardiac CMR a well-suited non-invasive tool to aid decision-making.
Abbreviations
- ASD:
-
Atrial septal defect
- CMR:
-
Cardiac magnetic resonance
- LPA:
-
Left branch pulmonary arteries
- LUPV:
-
Left upper pulmonary vein
- PAPVC:
-
Partial anomalous pulmonary venous connection
- PC CMR:
-
Phase contrast cardiac magnetic resonance imaging
- RMPV:
-
Right middle pulmonary vein
- RPA:
-
Right branch pulmonary arteries
- RUPV:
-
Right upper pulmonary vein
- RV:
-
Right ventricle
- RVED:
-
Right ventricular end-diastolic dimension
- SVC:
-
Superior vena cava
- TPBF:
-
Total pulmonary blood flow
References
Healey JE Jr (1952) An anatomic survey of anomalous pulmonary veins: their clinical significance. J Thorac Surg 23:433–444
Alsoufi B, Cai S, Van Arsdell GS, Williams WG, Caldarone CA, Coles JG (2007) Outcomes after surgical treatment of children with partial anomalous pulmonary venous connection. Ann Thorac Surg 84:2020–2026 discussion 2026
Brown DW, Geva T (2013) Anomalies of the pulmonary veins. In: Allen HD, Driscoll DJ, Shaddy RE, Feltes TF (eds) Moss and Adams heart disease in infants, children, and adolescents : including the fetus and young adult, 8th edn. Lippincott Williams & Wilkins, Philadelphia, pp 809–839
Rudolph A (2001) Atrial septal defect and partial anomalous drainage of pulmonary veins. In: Rudolph A (ed) Congenital diseases of the heart: clinical-physiological considerations, 2nd edn. Futura Publishing Company, Armonk, pp 245–282
Kouchoukos NT, Blackstone EH, Hanley FL, Kirlin JK (2013) Atrial septal defect and partial anomalous pulmonary venous connection. In: Kouchoukos NT, Blackstone EH, Hanley FL, Kirlin JK (eds) Kirklin/Barratt-Boyes Cardiac surgery, 4th edn. Saunders, Philadelphia, pp 1150–1182
Andersen M, Moller I, Lyngborg K, Wennevold A (1976) The natural history of small atrial septal defects; long-term follow-up with serial heart catheterizations. Am Heart J 192:302–307
Alpert JS, Dexter L, Vieweg WV, Haynes FW, Dalen JE (1977) Anomalous pulmonary venous return with intact atrial septum: diagnosis and pathophysiology. Circulation 156:870–875
Tajik AJ, Gau GT, Ritter DG, Schattenberg TT (1972) Echocardiographic pattern of right ventricular diastolic volume overload in children. Circulation 46:36–43
Goo HW, Al-Otay A, Grosse-Wortmann L, Wu S, Macgowan CK, Yoo SJ (2009) Phase-contrast magnetic resonance quantification of normal pulmonary venous return. J Magn Reson Imaging 29:588–594
Grosse-Wortmann L, Al-Otay A, Goo HW et al (2007) Anatomical and functional evaluation of pulmonary veins in children by magnetic resonance imaging. J Am Coll Cardiol 49:993–1002
Valsangiacomo ER, Barrea C, Macgowan CK, Smallhorn JF, Coles JG, Yoo SJ (2003) Phasecontrast MR assessment of pulmonary venous blood flow in children with surgically repaired pulmonary veins. Pediatr Radiol 33:607–613
Valsangiacomo ER, Levasseur S, McCrindle BW, MacDonald C, Smallhorn JF, Yoo SJ (2003) Contrast-enhanced MR angiography of pulmonary venous abnormalities in children. Pediatr Radiol 33:92–98
Kellenberger CJ, Yoo SJ, Buchel ER (2007) Cardiovascular MR imaging in neonates and infants with congenital heart disease. Radiographics 27:5–18
Bryan AC, Bentivoglio LG, Beerel F, Macleish H, Zidulka A, Bates DV (1964) Factors affecting regional distribitution of ventilation and perfusion of the lung. J Appl Physiol 19:395–402
Marom EM, Herndon JE, Kim YH, McAdams HP (2004) Variations in pulmonary venous drainage to the left atrium: implications for radiofrequency ablation. Radiology 230:824–829
Kato R, Lickfett L, Meininger G et al (2003) Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation 107:2004–2010
Lopez L, Colan SD, Frommelt PC et al (2010) Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr 23:465–495 quiz 576-7
Lai WW, Geva T, Shirali GS et al (2006) Guidelines and standards for performance of a pediatric echocardiogram: a report from the Task Force of the Pediatric Council of the American Society of Echocardiography. J Am Soc Echocardiogr 19:1413–1430
Lai WW, Gauvreau K, Rivera ES, Saleeb S, Powell AJ, Geva T (2008) Accuracy of guideline recommendations for two-dimensional quantification of the right ventricle by echocardiography. Int J Cardiovasc Imaging 24:691–698
Daubeney PE, Blackstone EH, Weintraub RG, Slavik Z, Scanlon J, Webber SA (1999) Relationship of the dimension of cardiac structures to body size: an echocardiographic study in normal infants and children. Cardiol Young 9:402–410
Saalouke MG, Shapiro SR, Perry LW, Scott LP 3rd (1977) Isolated partial anomalous pulmonary venous drainage associated with pulmonary vascular obstructive disease. Am J Cardiol 39:439–444
Babb JD, McGlynn TJ, Pierce WS, Kirkman PM (1981) Isolated partial anomalous venous connection: a congenital defect with late and serious complications. Ann Thorac Surg 31:540–541
Ward KE, Mullins CE (1998) Anomalous pulmonary venous connections, pulmonary vein stenosis, and atresia of the common pulmonary vein. In: Garson AJ, Bricker JT, Fischer DJ, Neish SR (eds) The science and practice of pediatric cardiology, 2nd edn. Williams & Wilkins, Baltimore, pp 1431–1461
Hancock Friesen CL, Zurakowski D, Thiagarajan RR et al (2005) Total anomalous pulmonary venous connection: an analysis of current management strategies in a single institution. Ann Thorac Surg 79:596–606 discussion 596-606
Caldarone CA, Najm HK, Kadletz M et al (1998) Relentless pulmonary vein stenosis after repair of total anomalous pulmonary venous drainage. Ann Thorac Surg 66:1514–1520
Greenway SC, Yoo SJ, Baliulis G, Caldarone C, Coles J, Grosse-Wortmann L (2011) Assessment of pulmonary veins after atrio-pericardial anastomosis by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 13:72
Said SM, Burkhart HM, Schaff HV et al (2012) Single-patch, 2-patch, and caval division techniques for repair of partial anomalous pulmonary venous connections: does it matter? J Thorac Cardiovasc Surg 143:896–903
Buz S, Alexi-Meskishvili V, Villavicencio-Lorini F et al (2009) Analysis of arrhythmias after correction of partial anomalous pulmonary venous connection. Ann Thorac Surg 87:580–583
Feltes TF, Bacha E, Beekman RH 3rd et al (2011) Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Circulation 123:2607–2652
Boehrer JD, Lange RA, Willard JE, Grayburn PA, Hillis LD (1992) Advantages and limitations of methods to detect, localize, and quantitate intracardiac left-to-right shunting. Am Heart J 124:448–455
Beerbaum P, Korperich H, Barth P, Esdorn H, Gieseke J, Meyer H (2001) Noninvasive quantification of left-to-right shunt in pediatric patients: phase-contrast cine magnetic resonance imaging compared with invasive oximetry. Circulation 103:2476–2482
Festa P, Ait-Ali L, Cerillo AG, De Marchi D, Murzi B (2006) Magnetic resonance imaging is the diagnostic tool of choice in the preoperative evaluation of patients with partial anomalous pulmonary venous return. Int J Cardiovasc Imaging 22:685–693
Roman KS, Kellenberger CJ, Macgowan CK et al (2005) How is pulmonary arterial blood flow affected by pulmonary venous obstruction in children? A phasecontrast magnetic resonance study. Pediatr Radiol 35:580–586
Henk CB, Schlechta B, Grampp S, Gomischek G, Klepetko W, Mostbeck GH (1998) Pulmonary and aortic blood flow measurements in normal subjects and patients after single lung transplantation at 0.5 T using velocity encoded cine MRI. Chest 114:771–779
Ley S, Fink C, Puderbach M et al (2006) MRI Measurement of the hemodynamics of the pulmonary and systemic arterial circulation: influence of breathing maneuvers. AJR Am J Roentgenol 187:439–444
Dollery CT, West JB, Wilcken DE, Hugh-Jones P (1961) A comparison of the pulmonary blood flow between left and right lungs in normal subjects and patients with congenital heart disease. Circulation 24:617–625
Johnson MC, Sekarski TJ, Balzer DT (2000) Echocardiographic prediction of left-to-right shunt with atrial septal defects. J Am Soc Echocardiogr 13:1038–1042
Laurenceau JL, Dumesnil JG, Gagne S (1975) Echocardiographic evaluation of the significance of shunt in secondary communications and in partial abnormal pulmonary venous returns. Arch Mal Coeur Vaiss 68:619–624
Greutmann M, Tobler D, Biaggi P et al (2012) Echocardiography for assessment of regional and global right ventricular systolic function in adults with repaired tetralogy of Fallot. Int J Cardiol 157:53–58
Mertens LL, Friedberg MK (2010) Imaging the right ventricle—current state of the art. Nat Rev Cardiol 7:551–563
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Shi-Joon Yoo.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise.
No complex statistical methods were necessary for this paper.
Ethical approval
Institutional Review Board approval was obtained.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Methodology
• retrospective
• cross-sectional study, diagnostic or prognostic study, observational
• performed at one institution
Rights and permissions
About this article

Cite this article
Seller, N., Yoo, SJ., Grant, B. et al. How many versus how much: comprehensive haemodynamic evaluation of partial anomalous pulmonary venous connection by cardiac MRI. Eur Radiol 28, 4598–4606 (2018). https://doi.org/10.1007/s00330-018-5428-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5428-9