
Abstract
The aim was to compare X-ray and ultrasound (US) in diagnosing gout. In a prospective study, 105 consecutive patients with clinical suspicion of gout underwent conventional X-ray und high-resolution US in order to help in arriving at a definite diagnosis. X-ray findings suggestive of gout included soft-tissue opacifications with densities between soft tissue and bone, articular and periarticular bone erosions, and osteophytes at the margins of opacifications or erosions. US findings suggestive of gout included bright stippled foci and hyperechoic soft-tissue areas. Fifty-five patients had a definite diagnosis of gout (102 involved sites), 31 patients were diagnosed as having another disease (59 involved sites), and 19 patients were excluded from the study because a definite diagnosis could not be established. X-ray suggested gout with a sensitivity of 31% (32/102) and a specificity of 93% (55/59), whereas US suggested gout with a sensitivity of 96% (98/102) and a specificity of 73% (43/59). US was much more sensitive than conventional X-ray but less specific. Our data show that US often provided additional diagnostic information in patients with clinical suspicion of gout when laboratory findings and X-ray results were negative or inconclusive and should therefore be used in these cases.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Gout is a disorder of purine metabolism with a raised but variable blood uric acid level and deposition of monosodium urate crystals preferentially in the joints and soft tissues of the extremities [1]. It occurs especially in men and affects about 1% of the population in Western countries [2]. Gout often has a characteristic clinical presentation with an acute, exquisitely painful monarthritis of the first metatarsophalangeal joint (MTP-I) or the knee, in combination with local redness and tumefaction. Laboratory investigations show elevated levels of blood uric acid. In these typical cases, diagnostic imaging is not necessary [3]. Frequently, however, the clinical presentation is atypical, involving another site, for instance, or showing prolonged and less severe clinical symptoms, or exhibiting normal levels of blood uric acid at the time of presentation [2, 4, 5]. In these cases, imaging of the involved site would be of importance to help reach a definite diagnosis of gout. X-ray is the established method and usually the first and the only imaging test performed [3, 6]. High-resolution ultrasound (US) is frequently employed for differential diagnosis of a variety of inflammatory joint diseases in our clinic; we found that US often demonstrates characteristic signs of gout, even in patients with normal X-rays. There are several investigations, primarily case studies, that report detection of monosodium urate deposits and gouty tophi with US [7–19]. However, there is no study which assessed the value of US for diagnosing gout in clinically suspicious cases in a substantial population. The aim of our study was to prospectively compare the diagnostic success of US and X-ray in patients with clinical suspicion of gout that either had gouty inflammation or another musculoskeletal disorder.
Materials and methods
A total of 105 consecutive adult patients (13 women, 92 men; age range: 31–89 years; mean age: 59 years) with clinical suspicion of gout were referred to us by the Rheumatological Outpatient Department of our university hospital for further evaluation by appropriate diagnostic imaging. The patient cohort included those with a high, intermediate, or a low clinical probability of having gout. All patients underwent both conventional X-ray examination and high-resolution US scanning in order to help establish a definite diagnosis.
X-ray examinations of each clinically involved site were performed in two planes, using modern systems (digital luminescence radiography, Agfa). US examinations were performed using high-quality broadband linear transducers with a frequency range of 8–14 MHz (Sonoline Elegra, Sonoline Antares, Acuson Sequoia 512; Siemens Medical Systems). Color Doppler US was done as sensitively as possible for slow blood flow (frequency: 7–10 MHz; PRF: 800–1200) at a still usable ratio of signal-to-background noise. X-rays and US images were digitally stored in a PACS and viewed on high-quality screens (5K, Magic View, Siemens Medical Systems).
Imaging signs
X-ray findings suggestive of gout—which we have taken into consideration in this study—included soft-tissue opacifications with densities between soft tissue and bone (Fig. 1), articular and periarticular bone erosions (Fig. 2), and osteophytes at margins of opacifications or erosions (Fig. 2).

A 56-year-old man with gouty arthritis of the left MTP-I joint. a Longitudinal US image at the region of the MTP-I joint reveals a hyperechoic cloudy area representing monosodium urate deposits within the thickened synovia (arrows). Osteophytes at the joint margins indicate arthrosis (arrowheads). b Various color Doppler signals within the synovia are due to inflammation. X-rays in PA (c) and oblique projection (d) demonstrate signs of arthrosis (arrows), as well as cloudy soft-tissue opacifications (arrowheads) representing monosodium urate deposits

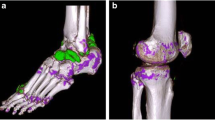
A 67-year-old woman with gouty monarthritis of the proximal interphalangeal (PIP) joint of the right index finger. a Longitudinal US image at the region of the PIP-II joint reveals bright stippled foci (arrows) and hyperechoic aggregates (arrowheads) representing monosodium urate deposits within the thickened hypoechoic synovia and the joint space. Osseous erosion is also visible (thick arrow). b Multiple color Doppler signals within the synovia indicate considerable inflammation. X-rays in PA (c) and oblique projection (d) demonstrate osseous erosion (arrowhead) with a tiny calcification and an osteophyte at the margin of the erosion (arrow) suggesting gout. Soft-tissue opacifications were not detectable
US findings suggestive of gout analyzed in this study, included bright stippled foci (Figs. 2, 3, 4, 5, and 6), hyperechoic soft-tissue areas (Figs. 1, 2, 4, 5, and 6), hypoechoic streaks between and around hyperechoic areas (Fig. 4), hypervascularisation at color Doppler US (Figs. 1, 2, 3, and 5), and articular and periarticular bone erosions (Fig. 2).

A 54-year-old man with gouty arthritis of the right MTP-I joint. a Longitudinal US image at the region of the MTP-I joint reveals bright stippled foci (arrows) representing monosodium urate deposits within the thickened hypoechoic synovia. b Multiple color Doppler signals within the synovia and surrounding tissue indicate considerable inflammation. X-rays in PA (c) and oblique projection (d) demonstrate signs of mild arthrosis at the MTP-I joint but no specific sign of gout

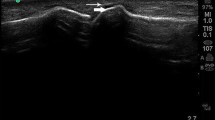
A 65-year-old man with tophaceous gout of the left MTP-I joint. Longitudinal US image at the region of the MTP-I joint reveals bright stippled foci (arrows) and hyperechoic areas (arrowheads) representing monosodium urate deposits. Hyperechoic urate deposits are surrounded by hypoechoic bands (triangles)

A 52-year-old man with gouty arthritis of the left knee. a Transverse US image laterally to the patella shows moderate echo-free joint effusion with slightly thickened (1 mm) synovia (arrows) indicating arthritis. b Longitudinal US image medial at the knee reveals cloudy hyperechoic areas (arrowheads) and stippled bright foci (arrows) representing monosodium urate deposits close to the meniscus (triangle). X-ray in PA projection (c) shows medial reduction of cartilage (arrow), and in lateral projection (d) joint effusion in the recessus suprapatellaris (arrow). The X-rays do not show signs suggestive of gout

A 41-year-old man with gouty inflammation of Achilles tendon. a-b Longitudinal US images of the right Achilles tendon show cloudy hyperechoic areas (arrowheads) and stippled bright foci (arrows) representing monosodium urate deposits at the Achilles tendon (triangles). b Color Doppler US reveals inflammatory hypervascularisation in and around the tendon. c X-ray of the right calcaneus in lateral projection shows spindle-shaped thickening of the Achilles tendon (arrowheads), usually observed in patients with tendinosis, but does not reveal signs suggestive of gout
Imaging evaluation
All images from each method applied were independently reviewed by two experienced radiologists and thereafter a consensus opinion on each imaging sign was obtained.
Reference standard
Definite diagnoses were established by microscopy of aspirates or by characteristic clinical and laboratory findings.
Statistical analysis
We calculated the estimates for sensitivity and specificity for each single imaging sign, as well as for the positive predictive value, the negative predictive value, and the accuracy for US and X-ray as imaging methods (Table 3). For all measures, 95% confidence intervals were determined (Table 3).
Data analyses were performed by using the Stata statistical software package (version 9.0, StataCorp, College Station, Tex.) for Windows (Microsoft, Redmond, Wash.).
Results
Fifty-five patients had a definite diagnosis of gout, 31 were diagnosed as having another disease, and 19 were excluded from the study since a definite diagnosis could not be established. Of the 55 patients with gout 51 were male. The other diagnoses in the above-mentioned 31 study patients are shown in Table 1.
Among the 55 patients with gout, 26 patients had each one clinically involved site, 17 had two each, ten had three each, and three patients had four each involved sites. One hundred and two clinically involved sites in the 55 patients with gout (Table 2) and 59 clinically involved sites in the 31 patients without gout were examined and evaluated with X-ray and US.
Definite diagnoses were established by microscopy of aspirates in 30 patients and by characteristic clinical and laboratory findings in 56 patients.
Plain radiography revealed soft-tissue opacifications in 27 of 102 sites with gout (26%) and in two of 59 sites without gout (3%). Articular and periarticular bone erosions suggestive of gout were shown in 20 of 102 sites with gout (20%) and in three of 59 sites without gout (5%). Osteophytes at the margins of bone erosions or tophi were present in five of 102 sites with gout (5%) and in none of the 59 sites without gout (0%).
US revealed bright stippled foci in 82 of 102 sites with gout (80%) and in 15 of 59 sites without gout (25%). Hyperechoic areas were seen in 81 of 102 sites with gout (79%) and in three of 59 sites without gout (5%). Bone erosions were detectable in 24 of 102 sites with gout (24%) and in 18 of 59 sites without gout (31%). Hypoechoic streaks were detected in 82 of 102 sites with gout (80%) and in 30 of 59 sites without gout (51%). Color Doppler US showed hypervascularisation in 96 of 102 sites with gout (94%) and in 28 of 59 sites without gout (47%).
In 66 of 102 sites (65%), US demonstrated characteristic findings of gout (bright stippled foci and/or hyperechoic areas) whereas X-rays did not show signs of gout (Figs. 3, 5, and 6). We had no patients with gout in whom X-rays were suggestive of gout but US was negative. Only in four of 102 sites with gout (4%) did US fail to reveal signs of urate deposits (bright stippled foci or hyperechoic areas). These sites were three knees and one carpus in four different patients. US revealed increased echo-free fluid within the three knees, thickened synovia in two knees and the carpus, hypervascularisation at color Doppler in the synovia of one knee and the carpus, but no US signs of urate deposits.
Sensitivities, specificities, positive predictive values (PPVs), negative predictive values (NPVs), and accuracies, as well as 95% confidence intervals are shown in Table 3.
Discussion
X-ray is a quick and effective standard imaging method for the musculoskeletal system and is therefore usually the first imaging procedure in the investigation of disorders of this system [1, 20, 21]. X-ray is also the established imaging method in patients with gout since it can reveal characteristic signs of gout [6, 10, 22–27]. At our institution, additionally to X-ray, we perform high-resolution US investigation in gout patients. US frequently shows distinctive signs of gout even in patients with negative X-ray results and has therefore become a standard procedure for several years at our hospital. In the present study, we evaluated high-resolution US in diagnosing gout and compared it with X-ray, the established standard method.
X-ray has been known for a long time to reveal characteristic signs of gout, including soft-tissue opacifications with densities between soft tissue and bone representing urate deposits (Fig. 1), as well as articular and periarticular well-marginated bone erosions (Fig. 2), osteophytes at the margins of tophi or erosions (“overhanging edges”) (Fig. 2), and signs of arthrosis (Fig. 1) [1, 6, 10, 22–27]. We prospectively evaluated these signs in our patient cohort with the exception of arthrosis. Signs of arthrosis, while often present in patients with gout, are too unspecific and were therefore not investigated further in the present study. A distribution and appearance of articular and periarticular bone erosions consistent with gout but different from that typical for rheumatoid arthritis or psoriatic osteoarthropathy was taken as an important X-ray sign (Fig. 2) [10].
Our study shows that X-rays revealed signs of gout in advanced cases but failed to do so in the majority of patients (negative in 69%, 70 of 102 involved sites) (Figs. 3, 5, and 6). Several authors frequently found X-rays in patients with gout to be negative for a long time [3, 6, 10, 16, 28]. In a radiographic study with a large cohort, Bloch et al. [6] reported that X-rays did not show signs of gout in 45% (210 of 466 patients). They pointed out that there is usually a latent period of about 5–10 years between the first clinical symptoms and the appearance of specific radiologic signs [6]. Gout primarily involves soft tissues in and around the joints [6]. It could, therefore, be expected that signs of gout are detected by US at an earlier stage of disease than on plain radiography since the specific advantage of US is its ability to detect soft-tissue changes [29–32]. Due to the high acoustic impedance difference between soft tissues and urate deposits and the considerable spatial resolution of high-frequency US, punctiform urate deposits (visible as bright stippled foci) can be detected (Fig. 3) [15]. There has to be substantial amounts of urate deposits, however, before they can be detected on X-ray as elevated soft-tissue densities (Fig. 1) [15]. An additional advantage is that gout primarily affects the peripheral regions of the human body, which can be quite well examined by high-frequency US.
Consistent with our observations, there are several reports in the literature, mostly case reports, that describe bright spots and hyperechoic areas on US scans lying within areas of gouty tophi [9, 12–19]. However, descriptions of US appearances of gouty tophi in the literature vary substantially as follows: heterogeneous masses, composed of hypoechoic and hyperechoic areas with generally more of the tophus being hyperechoic, occasionally showing posterior acoustic shadow [12]; markedly increased echogenicity and heterogeneity and posterior to the increased echogenicity loss of detail and shadowing [18]; hyperechoic area [13]; heterogeneously echogenic nodules with internal hyperechoic spots [17]; in homogeneously echoic “echotexture” and/or hyperechoic bands generating a posterior acoustic shadow and/or hyperechoic spots [16]; hypoechogenic with bright spots in the periphery and some shadowing [9]; bulky hypoechoic heterogeneous material [11]. In our experience gouty tophi often present as heterogeneous masses containing hypoechoic and hyperechoic areas (Figs. 2, 4, 5, and 6). Furthermore, US images are usually assessed by subjective optical impressions and therefore descriptions used can vary. Hyperechoic areas with bright spots represent urate deposits or calcifications if additionally present in some cases, whereas hypoechoic areas seem to represent zones of fibrous and inflammatory tissue or are caused by acoustic absorption and shadowing (Fig. 4). We found hyperechoic areas and bright stippled foci as being characteristic for gout; so we focused only on these signs in our study irrespective of whether the major part of a lesion appeared hypoechoic, hyperechoic or inhomogeneous and also irrespective of its localization within soft tissues, tophi, synovia, or synovial fluid.
In the literature we found four studies which were not just case reports dealing with US signs of gout.
One of these studies by Nalbant et al. [12] describes the sonographic appearances of subcutaneous nodules (20 tophi, 20 rheumatoid nodules, two sarcoid nodules, two lipomas, and four synovial cysts). In contrast to rheumatoid nodules, 80% of the gouty nodules appeared as heterogeneous masses with generally more of the nodule being hyperechoic on a portable US equipment (SonoSiteTM 180, 10–5 MHz linear array transducer) [12]. We also used this type of portable US device in several patients with gout at our intensive care units. These patients were not included in the present study since tiny bright stippled foci (an important criterion in our study) were often not detected by using this equipment compared with the high-end transducers which were used for our study patients. This observation is in accordance with Grassi et al. [15], who used high-quality equipment and emphasized that the findings in patients with gout may not be as easily detectable by lower quality US systems.
The other three articles are published by or in cooperation with W. Grassi from the University of Ancona, Italy [15, 16, 19]. Two of them are pictorial essays by Grassi et al. [15] and Farina et al. [19] in which several US signs of gout are described, such as the hyperechoic surface of hyaline cartilage, hyperechoic bands and spots within soft tissues, and the “snowstorm” appearance of synovial fluid without giving statistical parameters to assess the value of the signs. The third article is a recently published prospective study by Wright et al. [16], who compared US and X-ray in detecting bone erosions and characteristic sonographic features in the first metatarsophalangeal joints. They investigated the MTP-I joints of both feet in 39 patients with gout and in 22 control subjects. In the patients with gout, only 12 of 78 joints (15%) had clinical signs of inflammation at the time of investigation. X-ray revealed bone erosions in 22 (28%) and tophi in three (4%) of the 78 MTP-I joints investigated, whereas high-resolution US detected bone erosions in 52 (66%) and tophi in 38 (49%) joints [16]. Hyperechoic spots were found in nine joints (12%) [16]. In our study, only patients with symptoms (clinical signs of inflammation) were included and all clinically involved sites were prospectively investigated (Table 2) in order to evaluate the usefulness of US in diagnosing gout in patients with clinical suspicion.
In our study the presence of bright stippled foci and/or hyperechoic areas at US indicated gout with great sensitivity (96%), whereas the specificity was limited (73%) (Table 3). The low specificity was due to the presence of bright stippled foci also in several cases of arthrosis (n = 4), rheumatoid arthritis (n = 3), pseudogout (n = 3), and chondrocalcinosis (n = 1) representing punctiform calcifications (Figs. 7 and 8). If only hyperechoic (cloudy) areas representing larger aggregates of urate deposits are taken as the criterion, specificity improved to 95% at a sensitivity of 79% (Table 3). Only two cases of chondrocalcinosis and one case of pseudogout in our study gave false positive results with respect to hyperechoic areas. The high specificity of hyperechoic areas as an US sign was comparable with the high specificity of X-ray (93%) in our series. However, X-ray had very low sensitivity (31%) (Table 3). In our patient cohort with gout, there was not a single site which was suggestive of gout on X-ray but negative on US. Among the 32 sites showing gout on X-ray, there was only one in which bright stippled foci were present and hyperechoic areas (the more specific US sign) absent. In all the other 31 X-ray-positive sites, there were hyperechoic areas at US detectable.

A 78-year-old man with rheumatoid arthritis. a-b Longitudinal US images at the region of the right metacarpophalangeal joints II (a) and III (b) reveal several bright stippled foci (arrows) within the synovia and joint fluid representing tiny calcifications at microscopy of the aspirate. Multiple osseous erosions are also visible (arrowheads)

A 52-year-old man with pseudogout. Six years after renal transplantation he developed a painful swelling at the dorsal aspect of the left elbow. US image shows various bright stippled foci (arrows) within the bursa olecrani representing tiny calcifications at microscopy of the aspirate
Bright stippled foci and/or hyperechoic areas enabled a negative predictive value of 91%, signifying that a negative US investigation for these two US signs excluded gout with a probability of 91%.
In patients with gouty inflammation, hypoechoic streaks within and around urate deposits and/or hypoechoic synovial thickening were often detected (80%) (Figs. 2, 3, 4, and 5) (Table 3). These hypoechoic areas were usually seen to be hypervascularized at color Doppler US (Figs. 2 and 3) (Table 3). This observation is in accordance with reports in the literature [9, 11, 17] and we suppose that they represent inflammatory changes. While hypoechoic hypervascularized streaks indicate inflammation, they give no indication of its cause as it is an unspecific feature. Only in combination with bright stippled foci and hyperechoic areas (representing urate deposits) are they relatively specific for the presence of gout. In our study we assessed percentages of occurrence (Table 3); however, we did not consider them for statistical analysis. We could omit them without losing sensitivity significantly since we encountered only two out of 102 sites with gouty inflammation in which inflamed tissue was observed without at least one of our two US signs of urate deposits. On the other hand, detection of inflammatory changes (hypoechoic hypervascularized streaks at gray-scale and color Doppler US) leads to the site of pathology and is therefore an essential aspect of the US diagnosis of (gouty) inflammation. Bone erosions were detected more often by US than by X-ray in our study, which is in agreement with the report of Wright et al. [16]. However, we could not define reliable US criteria to differentiate between erosions due to gout and erosions due to rheumatoid or psoriatic arthritis, and therefore we excluded them from further analysis as being unspecific (Table 3). Since we did not encounter cases in which US was positive for the presence of erosions and simultaneously negative for the presence of important signs for gout (bright stippled foci and hyperechoic areas), our exclusion of bone erosions made no difference.
In the present study we had a high percentage of patients with atypical clinical presentation, since the patients were referred from the Rheumatological Outpatient Department of our hospital. Typical cases of gout are usually treated by their general practitioners and are not referred to our radiology department.
We also encountered several cases of tophi without surrounding inflammatory changes at US which represent clinically silent urate deposits. These patients were not part of the study, since we evaluated only individuals with clinical symptoms.
In summary, we found bright stippled foci and hyperechoic (cloudy) areas representing monosodium urate deposits of different sizes seen on US to be reliable features in the diagnosis of gout. US is much more sensitive than conventional X-ray but less specific. Our data show that US often provides decisive additional diagnostic information in patients with clinical suspicion of gout when laboratory findings and X-ray results are negative or inconclusive and should therefore be used in these cases.
References
Watt I (1997) Basic differential diagnosis of arthritis. Eur Radiol 7:344–351
Terkeltaub RA (2003) Gout. N Engl J Med 349:1647–1655
Gentili A (2006) The advanced imaging of gouty tophi. Curr Rheumatol Rep 8:231–235
Feydy A, Liote F, Carlier R, Chevrot A, Drape JL (2006) Cervical spine and crystal-associated diseases: imaging findings. Eur Radiol 16:459–468
Monu JU, Pope TL Jr (2004) Gout: a clinical and radiologic review. Radiol Clin North Am 42:169–184
Bloch C, Hermann G, Yu TF (1980) A radiologic reevaluation of gout: a study of 2,000 patients. AJR Am J Roentgenol 134:781–787
Grassi W, Filippucci E, Farina A, Cervini C (2000) Sonographic imaging of the distal phalanx. Semin Arthritis Rheum 29:379–384
Lyburn ID, Torreggiani WC, Harris AC, Zwirewich CV, Munk PL (2002) Tophaceous podagra: ultrasound diagnosis. Hosp Med 63:48–49
Gerster JC, Landry M, Dufresne L, Meuwly JY (2002) Imaging of tophaceous gout: computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 61:52–54
Falasca GF (2006) Metabolic diseases: gout. Clinics? Dermatol 24:498–508
Balbir-Gurman A, Nahir AM, Braun-Moscovici Y, Soudack M (2005) Sonographic features of a tophaceous nodule. Isr Med Assoc J 7:746–747
Nalbant S, Corominas H, Hsu B, Chen LX, Schumacher RH, Kitumnuaypong T (2003) Ultrasonography for assessment of subcutaneous nodules. J Rheumatol 30:1191–1195
O’Leary ST, Goldberg JA, Walsh WR (2003) Tophaceous gout of the rotator cuff: a case report. J Shoulder Elbow Surg 12:200–201
Wakefield RJ, Emery P, Pease C (2003) Gout related upper limb cellulitis: an ultrasound study. J Rheumatol 30:417–419
Grassi W, Meenagh G, Pascual E, Filippucci E (2006) “Crystal clear”—Sonographic assessment of gout and calcium pyrophosphate deposition disease. Semin Arthritis Rheum 36:197–202
Wright SA, Filippucci E, McVeigh C, Grey A, McCarron M, Grassi W, Wright GD, Taggart AJ (2007) High-resolution ultrasonography of the 1st metatarsal phalangeal joint in gout: a controlled study. Ann Rheum Dis 66:859–864
Ho CF, Chiou HJ, Chou YH, Chang CY (2003) Peritendinous lesions: the role of high-resolution ultrasonography. J Clin Imag 27:239–250
Coombs PR, Houseman N, White R (2006) Chronic tophaceous gout of the third flexor digitorum profundus tendon in the hand: An unusual sonography diagnosis. AJR Am J Roentgenol 187:313–315
Farina A, Filippucci E, Grassi W (2002) Sonographic findings of the synovial fluid. Reumatismo 54:261–265
van der Jagt EJ, Hofman S, Kraft BM, van Leeuwen MA (2000) Can we see enough? A comparative study of film-screen vs digital radiographs in small lesions in rheumatoid arthritis. Eur Radiol 10:304–307
Sammak B, Abd El Bagi M, Al Shahed M, Hamilton D, Al Nabulsi J, Youssef B, Al Thagafi M (1999) Osteomyelitis: a review of currently used imaging techniques. Eur Radiol 9:894–900
Watt I, Middlemiss H (1975) The radiology of gout. Clin Radiol 26:27–36
Brailsford JF (1959) The radiology of gout. Br J Radiol 32:472–478
Berens DL (1978) Roentgenographic changes in gout. Postgrad Med 63:154–161
Resnick D (1977) The radiologic manifestations of gouty arthritis. Clin Rev Diagn Imaging 9:265–335
Huber N (1896) Zur Verwerthung der Roentgen-Strahlen im Gebiete der inneren Medicin [The use of X-rays in internal medicine]. Dtsch Med Wochenschr 22:182–184
Martel W (1968) The overhanging margin of bone: a roentgenologic manifestation of gout. Radiology 91:755–756
Gerster JC, Landry M, Rappoport G, Rivier G, Duvoisin B, Schnyder P (1996) Enthesopathy and tendinopathy in gout: computed tomographic assessment. Ann Rheum Dis 55:921–923
Lin J, Jacobson JA, Fessel DP, Weadock WJ (2000) An illustrated tutorial of musculoskeletal sonography. AJR Am J Roentgenol 175:1711–1719
Kane D, Grassi W, Sturrock R (2004) Musculoskeletal ultrasound—a state of the art review in rheumatology. Part 2: Clinical indications for musculoskeletal ultrasound in rheumatology. Rheumatology (Oxford) 43:829–838
Horcajadas AB, Lafuente JL, de la Cruz Burgos R, Muniz SH, Roca SA, Ortega SG, Franjo PD, Cruz EO (2003) Ultrasound and MR findings in tumor and tumor-like lesions of the fingers. Eur Radiol 13:672–685
Magarelli N, Guglielmi G, Di Matteo L, Tartaro A, Mattei PA, Bonomo L (2001) Diagnostic utility of an echo-contrast agent in patients with synovitis using power Doppler ultrasound: a preliminary study with comparison to contrast-enhanced MRI. Eur Radiol 11:1039–1046
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rettenbacher, T., Ennemoser, S., Weirich, H. et al. Diagnostic imaging of gout: comparison of high-resolution US versus conventional X-ray. Eur Radiol 18, 621–630 (2008). https://doi.org/10.1007/s00330-007-0802-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-007-0802-z