
Abstract
Purpose
GTI-2040 is a novel antisense oligonucleotide to the R2 subunit of ribonucleotide reductase. This phase II trial was conducted to determine the efficacy and tolerability of GTI-2040 when combined with docetaxel and prednisone for the treatment of patients with castration-resistant prostate cancer (CRPC).
Methods
Chemo-naïve CRPC patients with adequate performance status and organ function were treated with docetaxel 75 mg/m2 IV on day 1 plus GTI-2040 5 mg/kg/day by continuous intravenous infusion day 1–14 on a 21 day cycle, with prednisone 5 mg orally twice daily. The primary endpoint was PSA response rate. Pharmacokinetic studies of GTI-2040 and pharmacodynamic studies on peripheral blood mononuclear cells (PBMC) were also performed.
Results
Twenty-two patients in total (19 from this study and 3 from a prior phase I/II study at this institution) were treated at the recommended phase II dose. A confirmed PSA response was seen in 9/22 patients (41%). Of 16 patients with measurable disease, there was 1 partial response (PR) and 12 stable disease (SD) lasting 3.6 months (median), as best response. The most common toxicities were anemia, fatigue, lymphopenia, leucopenia and neutropenia. Grade 3+ toxicities included neutropenia, lymphopenia, leucopenia, fatigue, febrile neutropenia and hypophosphatemia.
Conclusions
The PSA response rate of GTI-2040 in combination with docetaxel and prednisone just met the minimum phase II criteria for further enrollment. However, after evaluation of all the clinical data, further study of this dose and schedule of GTI-2040 in CRPC was not recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most commonly diagnosed and second leading cause of cancer-related death in North America. Although androgen deprivation therapy is initially effective in treating recurrent or metastatic disease, all patients will eventually develop castration-resistant prostate cancer (CRPC). The current standard of care for CRPC are docetaxel-based regimens; however, long-term remissions are infrequent and not all patients respond, underscoring the need for novel therapeutic approaches [18, 21].
GTI-2040 is a synthetic phosphorothioate oligonucleotide complementary to the mRNA of the R2 subunit of ribonucleotide reductase (RNR). RNR is required for the reductive conversion of ribonucleotides to deoxynucleotides, a rate-limiting step in DNA synthesis and repair [14]. RNR is composed of two dissimilar subunits, R1 and R2, encoded on different chromosomes. R1 is present during the entire cell cycle and has a half-life of 18–24 h, while R2 expression increases dramatically in late G1/early S phase and has a half-life of only 3 h [2]. Although R2 is not an oncogene, it is overexpressed in many tumor tissues, and therefore may play a role in both tumorigenesis and drug resistance [7, 8].
GTI-2040 demonstrates dose-dependent growth inhibition of tumor cell lines including human prostate cancer cells and xenografts. At concentrations ≥0.2 μM, GTI-2040 decreases RNR R2 mRNA expression in human tumor cell lines and arrests cells in early G1/S phase. Efficacy in vivo against chemotherapy-resistant tumors has also been documented, including those tumors resistant to other RNR inhibitors such as gemcitabine and hydroxyurea. GTI 2040 has shown synergistic tumor weight reduction when combined with conventional chemotherapy, including the taxanes that arrests cells in a different phase (G2/M) of the cell cycle compared with GTI-2040 [14, 17].
A single agent phase I trial of GTI-2040 defined a maximally tolerate dose (MTD) of 185 mg/m2/day continuous infusion (CIV) over 21 days every 4 weeks. Fatigue and anorexia were the most common constitutional toxicities. The main dose-limiting toxicity (DLT) was reversible hepatic toxicity [6]. A phase I/II trial of GTI-2040 in combination with cytarabine in refractory and relapsed acute myelogenous leukemia (AML) has been successfully completed with plans for further study of this combination in AML [11]. A phase I/II study of GTI-2040 in combination with docetaxel (Study 6104) defined a recommended phase II dose (RP2D) of docetaxel 75 mg/m2 IV day 1 plus GTI-2040 5 mg/kg/day by continuous intravenous infusion day 1–14 on a 21-day cycle, with prednisone 5 mg orally twice daily. In this study, the main toxicities were neutropenia, sepsis, fatigue and GI toxicity, but DLT were not observed. One CRPC patient on this phase I/II study achieved a PSA response [15].
Given the preclinical activity of GTI-2040 in prostate cancer cell lines and xenografts, synergy of GTI-2040 with the taxanes and PSA response seen in the phase I/II study, this phase II trial of GTI-2040 in combination with docetaxel and prednisone in chemo-naïve CRPC patients was undertaken.
Patients and methods
Eligible patients had confirmed prostate adenocarcinoma with adequate organ function, ECOG PS 0/1, a PSA ≥20 ng/mL and disease progression (defined as ≥2 consecutive rises in PSA, 1 wk apart) despite castrate testosterone levels (<50 ng/mL). Anti-androgens (flutamide, nilutamide or cyproterone acetate) were stopped ≥4 weeks and bicalutamide ≥6 weeks prior to enrollment. Prior radiation was permitted provided ≥4 weeks elapsed prior to study entry. Key exclusion criteria were prior chemotherapy, radioisotope therapy or investigational agents for CRPC; brain metastases, symptomatic peripheral neuropathy ≥grade 2, or uncontrolled intercurrent illness. Due to the risk of pharmacokinetic interactions between anti-retroviral therapy and GTI-2040, HIV-positive patients were excluded. Patients receiving anti-coagulants except low-dose warfarin were also excluded.
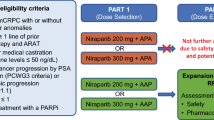
Study design and treatment
This was a multi-institutional phase II study conducted by the Princess Margaret Hospital (PMH) Phase II Consortium and the National Cancer Institute Cancer Therapy Evaluation Program (NCI CTEP). Ethics boards at all participating sites approved the study, and patients signed a written informed consent form. GTI-2040 manufactured by Lorus Therapeutics Inc., was supplied by NCI CTEP. All patients initially received docetaxel 75 mg/m2 IV day 1 plus GTI-2040 5 mg/kg/day by continuous intravenous infusion day 1–14 on a 21 day cycle, with prednisone 5 mg orally twice daily. Doses were adjusted for severe toxicity. In cycle 1, docetaxel was given on day 3 to allow pharmacokinetic analysis of GTI-2040 alone; on subsequent cycles, both drugs were given on day 1.
Treatment with GTI-2040, docetaxel and prednisone continued for 10 cycles or until one of the following: (1) disease progression defined as new/worsening disease symptoms requiring a change in management, objective progression in measurable disease by RECIST criteria, or two consecutive increases in PSA at least 25% over nadir and an absolute increase of at least 5 ng/mL), (2) intercurrent illness (3) unacceptable adverse event, (4) patient withdrawal or (5) investigator’s discretion.
Baseline and follow-up studies
Baseline assessment included a history, physical, height, weight, PS assessment; CBC with differential serum chemistries, prothrombin time, prostate-specific antigen (PSA), testosterone, EKG; chest X-ray or chest-computed tomography (CT), and abdominal and pelvis CT scans. Bone scans were performed if clinically indicated. PSA response was evaluated every 3 weeks with confirmatory PSA performed at least 3 weeks following PSA response. Measurable disease was evaluated every 3 cycles with confirmatory scans done 4–6 weeks following initial objective response. Blood samples for the pharmacokinetics of GTI-2040 were collected on day 1 pretreatment and cycle 1 at 2, 4, 8, 24, 48 h, day 15 and day 22 and cycle 2 day 15 and analyzed in the pharmacology laboratory at PMH using a previously described HPLC method [23]. Peripheral blood mononuclear cells (PBMC) were collected from only 8 patients at baseline and on day 3 of treatment for analysis of ribonucleotide reductase. Total RNA was extracted from PBMC, and higher quality samples were analyzed for mRNA expression of R1 and R2 and for the housekeeping genes (ß-actin, 18S, HuPo and TBP) by real-time PCR using the ABI 7900HT PCR system [9].
Response assessment
Patients receiving at least one cycle of therapy and having ≥2 PSA values at least 3 weeks apart from baseline were evaluable for PSA response. PSA response was defined as a 50% decrease in PSA from baseline confirmed by a second PSA value ≥3 weeks later. The PSA response duration began the date of the first 50% decline in PSA and ended when PSA increased by 25% over the nadir PSA with an increase of at least 5 ng/mL and confirmed by a second measurement [3]. Measurable response was evaluated using Response Evaluation Criteria in Solid Tumors criteria (RECIST) [22]. Treatment failure was defined as new or worsening disease, symptoms requiring change in management, a decrease in ECOG PS by two levels, new or objective progression in measurable disease, or a 25% increase over the baseline or nadir PSA (whichever was lower), with an increase of at least 5 ng/mL, confirmed by a second measurement. All patients receiving treatment were assessable for toxicity.
Statistical considerations
The primary end point was PSA response. A two-stage design based on both response and progression was used to ensure early closure if the regimen was inactive [20]. The study design was based around the PSA response rate expected with docetaxel and prednisone alone and the hypotheses of P 0 = 0.40 and P 1 = 0.60, α = 0.10, β = 0.10. Under this design, stage I was to accrue 18 patients with continuation to stage II if ≥8 PSA responses were observed. The true α = 0.095 and true β = 0.100 for this design.
Results
Patient population
Twenty-two patients were accrued to stage 1 from September 2004–2005. This included 3 patients treated at the recommended phase II dose (RP2D) from the phase I/II dose escalation study (Study 6104) at our institution. Patient baseline characteristics are listed in Table 1.
Adverse events (AE)
In total, 121 cycles of treatment were administered. Most frequent AE were anemia, fatigue, lymphopenia, alopecia and elevated alkaline phosphatase (Table 2). Twenty patients across 78 cycles experienced at least one grade 3 or higher adverse event. Four or more patients experienced grade 3+ neutropenia, lymphopenia, leucopenia, fatigue, febrile neutropenia and hypophosphatemia (Table 3).
Response
All 22 CRPC patients (from both studies) were evaluable for response. Nine patients had a confirmed PSA response (41%, 95% CI 21–64%) and thirteen patients had no PSA response, including one patient who had a PSA response that was unconfirmed due to no repeat test. From this phase II study alone, 8/19 had a confirmed PSA response, while 11 (including one unconfirmed response) had no PSA response. Since the stage I accrual target, considering all patients treated at the RP2D level was exceeded, and all 22 patients were evaluable for response, adjustments to the statistical design were necessary to mimic the initial hypotheses. The design was adjusted to test P 0 = 0.40 versus P 1 = 0.60, α = 0.10, β = 0.10 with stage I sample size fixed at 22. Using this design, >9 PSA responses were required to continue to stage 2.
Of the 16 patients overall who had measurable disease, 1 had PR, 12 had SD and 3 had PD. The patient with an objective PR also had a PSA response, as did 4/12 patients with SD, and 2/3 with PD. Patients coming off treatment were censored in the analysis of time to progression (TTP). Median TTP was 4.1 months (95% CI 3.5-not reached), and 6-month progression-free estimate was 41% (95% CI 22–77%) (Table 4).
Treatment discontinuation
All 22 patients are now off-study. Ten patients came off-treatment due to PD (two clinical PD), 5 due to adverse events (grade 5 febrile neutropenia, grade 4 fatigue, grade 4 infection, grade 3 lymphopenia and grade 3 febrile neutropenia), 1 pt came off at the investigators discretion, and 2 patients withdrew consent after cycle 3. Four patients completed 10 cycles of treatment and were removed having completed protocol. Median duration on study treatment was 3.5 mos (95% CI 3.0–5.1) with five patients remaining on treatment longer than 6 months (Table 4).
Deaths
As of this writing, 16 patients are known to have died. One patient included from the prior phase I/II study died due to febrile neutropenia during cycle 2. All other patients died >30 days after completion of study. Six-month survival is estimated at 82% (95% CI 67.2–99.6%), 1-year survival is estimated at 54% (95% CI 36.4–79.7%), and median survival is estimated to be 13.1 mo (95% CI 9.4-not reached) (Table 4).
Pharmacodynamic and pharmacokinetic studies
Figure 1 summarizes the expression data from 8 evaluable patients for R1 and R2 genes normalized to RPLP2 (a stable ribosomal housekeeping gene). The changes in expression of R1 were not significant during GTI-2040 treatment (Fig. 1a). R2 expression levels decreased in two patients, who responded to GTI-2040 on gene expression level, but did not change or slightly increased in the remaining 6 patients’ samples (Fig 1b). Figure 1c shows changes in R1 and R2 expression in 2 patients responding at the gene expression level. Only one of these patients showed a PSA response. Figure 1d shows expression changes in the 6 non-responding patients. This data was not robust enough to draw any firm conclusions. Pharmacokinetic analysis, showed T max to be 8 h (range 8–336 h), C max was 3.9 ± 2.3 ug/mL and AUC(0–336) 798 ± 624 ug*h/mL (Fig. 2).

RRM1 and RRM2 expression in patients’ WBC samples (PHL-024)

Pharmacokinetics of GTI-2040 treatment
Discussion
Docetaxel combined with prednisone administered every 3 weeks is currently the standard of care for the first-line treatment of CRPC. In the TAX 327 study, the PSA response rate of this regimen given every 3 weeks was 45%, with a median duration of response of 7.7 months, and updated overall survival of 17.9 months. The every 3-week docetaxel regimen also showed a response in terms of decreasing pain of 35% and improvements in quality of life of 22% [1, 21]. The goal of this phase II study was to determine whether the addition of the antisense oligonucleotide GTI-2040 to the every 3-week docetaxel and prednisone regimen was tolerable and would improve antitumor efficacy using PSA response rate as the primary endpoint.
The main toxicities of the combination of GTI-2040 with docetaxel and prednisone were anemia, fatigue and lymphopenia. In particular, the incidence of fatigue was 91%, which was much higher than the 53% incidence of fatigue reported on the TAX 327 study with docetaxel and prednisone alone [21].
The PSA response rate seen with the addition of GTI-2040 to docetaxel and prednisone was only 44% (9/22 patients), which was comparable to the 45% response rate seen with docetaxel and prednisone alone and just met the minimum phase II criteria for further enrollment. Although from a strictly response standpoint, the original criteria used to determine whether or not to proceed to stage 2 was appropriate, several important clinical factors became apparent that led to the study closing after stage 1. For example, only a median of 5 cycles of treatment with GTI-2040 could be delivered (time to progression was 4.1 months) compared with 9.5 cycles delivered on the TAX 327 study. Also, GTI-2040 required central venous access for the 14-day infusion, which was both inconvenient for a palliative regimen and associated with risks such as infection.
Despite the small number of samples collected in the study for pharmacodynamic analysis, reduced RRM2 was seen in only two patients, possibly indicating insufficient dosing of GTI-2040 to achieve adequate target downregulation. In elderly AML patients, Marcucci et al. [12] have explored a higher 7 mg/kg/day dosing and reported tolerability when administered over a shorter duration, in combination with cytarabine. Another issue is the optimal scheduling of these two agents. Preclinical studies are now showing that sequential rather than concurrent dosing may have superadditive effects. In a study by Lee et al., two cell lines were transfected with a suboptimal dose of GTI-2040 for 4 h followed by treatment with a suboptimal dose of docetaxel the same day or 24, 48 or 72 h later. The greatest effect was seen when docetaxel was administered 24 h post transfection, with similar results seen in a xenograft mouse model. Synergistic effects in the induction of cell-cycle arrest and apoptosis were also observed for the 48-h treatment schedule [13]. Taken together, altered dosing and scheduling may need to be explored further clinically. But at this point, it is unclear whether CRPC would be the ideal setting in which to do this because there is no confirmation that RRM2 is a key target in this disease. Notably, another RNR inhibitor, the chemotherapeutic drug gemcitabine has not shown activity in this disease [4, 5, 16].
Unfortunately in CRPC two recent studies combining standard first-line docetaxel with targeted therapies have either been stopped early due to toxicity or failed to meet their primary efficacy endpoints [10, 19]. This raises an important issue, which is the risk of compromising proven therapy when it is used in combination with other agents. Although response rates in this GTI 2040 study were similar to that seen with docetaxel alone, nearly every outcome listed in Table 4 was worse in a patient population that was not appreciably sicker or more heavily pretreated than the TAX 327 population. That coupled with the fact that fewer cycles could be delivered (5 cycles vs. 9 cycles on TAX 327) may explain why the median survival was only 13.2 months.
In conclusion, the PSA response rate of GTI-2040 in combination with docetaxel and prednisone in this study just met the minimum phase II criteria for further enrollment. However, after careful evaluation of all the clinical data, further study of this dose and schedule of GTI-2040 in CRPC was not recommended.
References
Berthold DR, Pond GR, Roessner M, de Wit R, Eisenberger M, Tannock AI (2008) Treatment of hormone-refractory prostate cancer with docetaxel or mitoxantrone: relationships between prostate-specific antigen, pain, and quality of life response and survival in the TAX-327 study. Clin Cancer Res 14:2763–2767
Bjorklund S, Skog S, Tribukait B, Thelander L (1990) S-phase-specific expression of mammalian ribonucleotide reductase R1 and R2 subunit mRNAs. Biochemistry 29:5452–5458
Bubley GJ, Carducci M, Dahut W, Dawson N, Daliani D, Eisenberger M, Figg WD, Freidlin B, Halabi S, Hudes G, Hussain M, Kaplan R, Myers C, Oh W, Petrylak DP, Reed E, Roth B, Sartor O, Scher H, Simons J, Sinibaldi V, Small EJ, Smith MR, Trump DL, Wilding G et al (1999) Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: recommendations from the Prostate-Specific Antigen Working Group. J Clin Oncol 17:3461–3467
Buch-Hansen TZ, Bentzen L, Hansen S, Hoeyer M, Jensen NV, Saxe C, Sengeloev L (2009) Phase I/II study on docetaxel, gemcitabine and prednisone in castrate refractory metastatic prostate cancer. Cancer Chemother Pharmacol
Cricca A, Marino A, Valenti D, Melotti B, Amaducci E, Guardigli C, Lenzi M, Martorana G, Buli P, Martoni AA (2006) Gemcitabine plus mitoxantrone and prednisone in the palliative treatment of hormone-resistant prostate cancer (HRPC): a phase II study (GOAM 01.01 study). Anticancer Res 26:2301–2306
Desai AA, Schilsky RL, Young A, Janisch L, Stadler WM, Vogelzang NJ, Cadden S, Wright JA, Ratain MJ (2005) A phase I study of antisense oligonucleotide GTI-2040 given by continuous intravenous infusion in patients with advanced solid tumors. Ann Oncol 16:958–965
Fan H, Villegas C, Huang A, Wright JA (1998) The mammalian ribonucleotide reductase R2 component cooperates with a variety of oncogenes in mechanisms of cellular transformation. Cancer Res 58:1650–1653
Huang A, Fan H, Taylor WR, Wright JA (1997) Ribonucleotide reductase R2 gene expression and changes in drug sensitivity and genome stability. Cancer Res 57:4876–4881
Juhasz A, Vassilakos A, Chew HK, Gandara D, Yen Y (2006) Analysis of ribonucleotide reductase M2 mRNA levels in patient samples after GTI-2040 antisense drug treatment. Oncol Rep 15:1299–1304
Kelly W, Halabi S, Carducci M, George DJ, Mahoney JF, Stadler WM, Morris MJ, Kantoff P, Monk JP, Small EJ (2010) A randomized, double-blind, placebo-controlled phase III trial comparing docetaxel, prednisone, and placebo with docetaxel, prednisone, and bevacizumab in men with metastatic castration-resistant prostate cancer (mCRPC): survival results of CALGB 90401. J Clin Oncol, Annu Meet Proc: Abstract No. LBA4511
Klisovic RB, Blum W, Wei X, Liu S, Liu Z, Xie Z, Vukosavljevic T, Kefauver C, Huynh L, Pang J, Zwiebel JA, Devine S, Byrd JC, Grever MR, Chan K, Marcucci G (2008) Phase I study of GTI-2040, an antisense to ribonucleotide reductase, in combination with high-dose cytarabine in patients with acute myeloid leukemia. Clin Cancer Res 14:3889–3895
Klisovic RB, Blum W, X W, S L, C K, L H, Zwiebel JA, Byrd JC, Grever MR, Marcucci G (2009) A phase 1 study of GTI-2040, an antisense to ribonucleotide reductase (RNR) in combination with high dose cytarabine (HiDAC) in relapsed or refractory acute myeloid leukemia (AML): pharmacokinetics (PK), pharmacodynamic (PD) and clinical results. Blood (Ash Annu Meet Abstr) 106
Lee Y, Avolino T, Feng N, Xiong K, Jin H, Wang M, Wright J, Young A (2007) Determination of optimized administration schedule of GTI-2040 and docetaxel combination treatment for NSCLC cells in vitro and in vivo. In: Proceedings of the American Association of Cancer Research Annual Meeting
Lee Y, Vassilakos A, Feng N, Lam V, Xie H, Wang M, Jin H, Xiong K, Liu C, Wright J, Young A (2003) GTI-2040, an antisense agent targeting the small subunit component (R2) of human ribonucleotide reductase, shows potent antitumor activity against a variety of tumors. Cancer Res 63:2802–2811
Leighl NB, Laurie SA, Knox JJ, Ellis PM, Shepherd FA, Burkes RL, Vincent M, Pond GR, Zwiebel JA, Moore MJ (2005) Phase I/II study of GTI-2040 plus docetaxel as 2nd-line treatment in non-small cell lung cancer (NSCLC) and other solid tumors. J Clin Oncol, Annu Meet Proc: Abstract No. 7253
Morant R, Bernhard J, Maibach R, Borner M, Fey MF, Thurlimann B, Jacky E, Trinkler F, Bauer J, Zulian G, Hanselmann S, Hurny C, Hering F (2000) Response and palliation in a phase II trial of gemcitabine in hormone-refractory metastatic prostatic carcinoma. Swiss Group for Clinical Cancer Research (SAKK). Ann Oncol 11:183–188
Orr RM (2001) GTI-2040. Lorus therapeutics. Curr Opin Investig Drugs 2:1462–1466
Petrylak DP, Tangen CM, Hussain MH, Lara PN Jr, Jones JA, Taplin ME, Burch PA, Berry D, Moinpour C, Kohli M, Benson MC, Small EJ, Raghavan D, Crawford ED (2004) Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med 351:1513–1520
Scher H, Chi KN, De Wit R, Berry WR, Albers P, Henick B, Venner P, Heidenreich A, Chu L, Heller G (2010) Docetaxel (D) plus high-dose calcitriol versus D plus prednisone (P) for patients (Pts) with progressive castration-resistant prostate cancer (CRPC): results from Phase III ASCENT2 trial. J Clin Oncol, Annu Meet Proc: Abstract No. 4509
Simon R (1989) Optimal two-stage designs for phase II clinical trials. Control Clin Trials 10:1–10
Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA (2004) Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 351:1502–1512
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, Gwyther SG (2000) New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 92:205–216
Zhang W, Leighl N, Zawisza D, Moore MJ, Chen EX (2005) Determination of GTI-2040, a novel antisense oligonucleotide, in human plasma by using HPLC combined with solid phase and liquid-liquid extractions. J Chromatogr B Analyt Technol Biomed Life Sci 829:45–49
Acknowledgments
Grant support: NIH grant. NCI contracts N01CM17107, N01CM62203.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sridhar, S.S., Canil, C.M., Chi, K.N. et al. A phase II study of the antisense oligonucleotide GTI-2040 plus docetaxel and prednisone as first-line treatment in castration-resistant prostate cancer. Cancer Chemother Pharmacol 67, 927–933 (2011). https://doi.org/10.1007/s00280-010-1389-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-010-1389-7