
Abstract
Objective
To locate the intramuscular nerve branches of the flexor digitorum superficialis (FDS) and determine the accurate site for botulinum toxin injection.
Design
This study anatomically dissected 24 arms of 12 fresh adult cadavers to find intramuscular nerve endings in the FDS. The motor branch points (MBPs), proximal limit points (PLPs), and distal limit points (DLPs) of the terminal intramuscular nerve endings were identified. These three parameters were expressed in longitudinal and transverse coordinates in relation to the FDS driving as a reference line.
Results
The mean length of the reference line was 234.6 ± 11.2 mm. In the longitudinal coordinate, the MBPs, PLPs, and DLPs were located at 41.6% (standard deviation (SD) 2.6%), 35.1% (SD 4.1%), and 53.4% (SD 4.6%) of the reference line in the first main branch and 72.4% (SD 4.5%), 67.5% (SD 1.5%), and 82.0% (SD 5.7%) in the second main branch, respectively. The mean value of the transverse coordinate was not greatly deviated from the reference line.
Conclusion
The MBPs of the first and second main branches are located approximately 41.6% and 72.4% of the reference line, which considers the FDS direction, respectively. This finding helps determine the optimal injection site for botulinum toxin in the FDS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Spasticity is a state of increased muscle tone that can occur after damage to the central nervous system due to stroke, traumatic brain injury, or spinal cord injury. The prevalence of spasticity after acute stroke may vary from 19% [16] to 92% [10]; particularly, the prevalence of upper limb spasticity is approximately 25% at 1 month and 22% at 6 months after the primary injury [9].
Generally, upper limb spasticity develops as a flexor synergic pattern: shoulder adduction and internal rotation, elbow flexion, forearm pronation, wrist and finger flexion posture [18]. In particular, spasticity of the finger flexor causes impairment of hand intrinsic movements such as grasping, pinching, and manipulating objects. It also affects the finger extension, which is needed to initiate hand grasp [18]. Therefore, treating finger spasticity is crucial for improving patients’ quality of life.
Spasticity can be treated in several ways. Recently, selective treatment of focal spasticity by local injection of botulinum toxin is an important and widespread therapeutic strategy. Botulinum toxin works by blocking the presynaptic release of acetylcholine to the neuromuscular junction, thereby decreasing the abnormal increase of the muscle tone [18].
Flexor digitorum superficialis (FDS) and flexor digitorum profundus are two important muscles for flexion of the index, middle, ring, and little fingers. FDS inserted into the intermediate phalanx to flex the proximal interphalangeal joint, metacapophalangeal joint, and wrist [17]. Regarding the origin of tendons, some study reports anatomical variations. Previously published textbooks described it as having two (humeroulnar and radial) or three (medial epicondyle, coracoid process of ulnar, anterior border of radius) origins [12, 17]. Recently, a more detailed description of the origin of FDS has been reported. The middle and ring fingers derive mostly from the radius, anterior common tendon (ACT), and posterior common tendon (PCT), while the index and little fingers mostly derive from the ACT, PCT, and anterior oblique ligaments of the ulnar collateral ligament, and occasionally originate from the tendon connected to the ACT [3, 11]. FDS is divided into superficial and deep layers. The more superficial and more proximal muscles form the tendons of the middle and ring fingers, while the deeper and more distal muscles form the tendons of the index and little fingers [12, 17]. Therefore, injecting into each digastric muscle bellies is necessary to effectively treat the spasticity of FDS. Although some studies suggest botulinum toxin injection sites for the FDS, no study has suggested injection sites at the intramuscular nerve endings of each digastric muscle, especially using the FDS driving as the reference line.
Hence, this study aimed to identify the location of the intramuscular nerve branches for each digastric muscle belly of the FDS and to provide an accurate injection region for the botulinum toxin.
Methods
Twenty-four arms of 12 fresh adult cadavers were anatomically dissected to find the intramuscular nerve endings of the FDS. These cadavers were all Koreans, and the donor’s ages ranged from 61 to 97 years. None of them had any history of neuromuscular disease, and none of the arms showed any evidence of previous surgery, trauma, or deformity. All cadavers were anatomically placed. The arm was incised at the midline, from the wrist joint to the elbow joint. In addition, two transverse incisions were made: a superior incision above the antecubital fossa and an inferior one below the wrist crease. The skin and the subcutaneous fat layer were removed to expose the forearm muscles. Then, the flexor carpi radialis and pronator teres muscles were dissected, taking care not to damage the branches of the median nerve. In the dissected specimen, digital caliper (Mitutoyo Co., Japan) was used to measure the distance between the reference line and the nerve entry point, and the number of branches in each segment was counted.
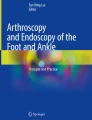
For all dissected nerves, the following points were identified: motor branch points (MBPs), which are the entry sites of the nerve into the muscle belly, and the proximal limit points (PLPs) and distal limit points (DLPs) of the terminal intramuscular nerve endings. These three parameters were expressed in longitudinal and transverse coordinates in relation to the reference line. The reference line was set as a line connecting the most prominent point of the medial epicondyle and the center of the line connecting the radial and ulnar styloid processes, taking into account the direction of the FDS. This reference line corresponds to the x-axis, and the vertical line to it is set to the y-axis. The location of each point was measured as the distance along the x-axis and y-axis, and each was defined as longitudinal and transverse coordinates. In particular, for longitudinal coordinates, the distance from the medial epicondyle was measured and divided by the reference line length to obtain a percentage value. For transverse coordinates, positive values were given when the point was located medial to the reference line. The longitudinal coordinates are expressed in % (standard deviation (SD)) and millimeter (SD), and the transverse coordinate in millimeter (SD) (Fig. 1).

Anatomic dissection showing the median nerve branch entering the flexor digitorum superficialis muscle. RS, radial styloid process; US, ulnar styloid process; ME, medial epicondyle; MBP, motor branch point; LC, longitudinal coordinate; TC transverse coordinate
Results
A total of 24 arms were investigated in 12 cadavers (7 males and 5 females: age, 79.7 ± 8.8 years). The mean length of the reference line was 25.09 ± 2.09 cm.
Of the 24 arms, 23 (95.8%) had the first and second main nerve branches, and 1 (4.2%) had only the first main branch. The number of twigs in the first main branch was 3 in 12 (50%) and 2 in 12 (50%) arms, and that in the second main branch was 3 in 6 (26.1%), 2 in 15 (65.2%), and 1 in 2 (8.7%) arms.
The longitudinal coordinates of the MBPs were 41.6% (SD 2.6%) of the reference line for the first main branch and 72.4% (SD 4.5%) for the second main branch. The longitudinal coordinates of the PLPs and DLPs were 32.9% (SD 5.9%) and 49.8% (SD 6.9%) of the reference line in the first main branch, and 65.1% (SD 5.2%) and 78.6% (SD 6.9%) in the second main branch, respectively (Fig. 2). Moreover, the mean value of the transverse coordinate was − 1.3 mm (SD 4.0 mm) in the first main branch and 2.0 mm (SD 8.5 mm) in the second main branch, indicating that each parameter did not deviate significantly from the reference line. The longitudinal and transverse coordinates of each point are listed in Table 1.

Schematic drawing of the MBP distribution in the FDS. Blue dots indicate the MBPs of the first main branch, green dots indicate the MBPs of the second main branch, and black dots indicate the average value of the MBPs in each branch. RS, radial styloid process; US, ulnar styloid process; ME, medial epicondyle; MN, median nerve; MBP1, MBP of first main branch; MBP2, MBP of second main branch
Discussion
In this study, the reference line was established considering the direction of the FDS and MBP locations of the first and second main branches were identified. The MBPs of the first and second main branch are located at approximately 40% and 70% of the reference line, respectively.
Most previous studies presenting injection points for FDS used forearm length as a reference line. Bickerton et al. identified individual digastric muscle bellies of the FDS and recommended these bellies as optimal sites for botulinum toxin injections [1]. This study found two injection points by focusing on the digastric muscle belly of FDS but could not provide an accurate injection location based only on one-dimensional information from the forearm length as a reference line. In addition, the muscle belly was suggested as the injection point, which was not based on the location of the intramuscular nerve ending,
To increase efficacy [2, 7, 13] and minimize side effects, such as paralysis of the adjacent muscles [15], the best place for botulinum toxin injections is considered to be close to the motor end plate, where the neuromuscular junction is located. In addition, targeting not only motor points but also muscle innervation areas may optimize the effectiveness of botulinum toxin injection [4, 6]. To that end, a precise knowledge on the anatomical location of intramuscular nerve endings is needed.
Some studies have recommended injection sites based on the location of intramuscular nerve endings in the FDS, but still only suggested one-dimensional locations based on the forearm length. Won et al. identified intramuscular the nerve distribution patterns of FDS using Sihler’s staining, finding two main nerve branches [19]. The entry points of each branch were 18.1% and 35.9% from the interepicondylar line. Compared to the present results, the location of each branch resulted from the proximal branch whereas that of the distal branch did not. Furthermore, Lepage et al. identified that FDS is innervated with two or three branches of the median nerve [8]. They demonstrated that end twigs of the proximal branch were located between 27.4% and 47.8% along the forearm length, those of the middle branch 44.8% and 63%, and those of the distal branch between 63.5% and 72%. The proximal and distal branches were located similarly to those in this study. However, they suggested that the penetration points of the nerve branches spread along the lateral edge of the muscle and that these sites were appropriate as the injection points. These locations are difficult to determine from the surface anatomy.
Only one previous study used the FDS direction as a reference line. Huber & Heck’s atlas suggested the injection into half of the distance between the medial epicondyle and the line connecting the radial styloid process to the ulnar one [5]. They recommended a reference line considering the origin and insertion of the FDS muscle, similar to this research. However, only one point was proposed for botulinum toxin injection; thus, the digastric muscle bellies of FDS were not considered.
A recent study revealed that the muscle belly of FDS for digit 2 is divided into proximal and distal belly and connected via the intermediate tendon [3]. In addition, most of the muscle belly of FDS for digit 5 was present, and it was suggested that the location was on the distal and ulnar side. In this study, we confirmed that the distal bellies for digits 2 and 5 are more distal than the muscle bellies for digits 3 and 4, which maybe the reason why injections are necessary for both, the distal and proximal part of FDS. In particular, given that the index finger is important for fine motor functions such as lateral and tip pinching, the spasticity of this finger must be treated. Therefore, clinicians need to inject botulinum toxin at the site of the distal nerve branch when treating spasticity of FDS.
This study has some limitations. First, the location of the intramuscular nerve ending was visually confirmed, and the pattern and density of this nerve ending could not be confirmed microscopically. However, considering the volume of botulinum toxin typically used in clinical settings, the injection should be sufficiently close to the target point—the motor end plate—even if injected into the visually confirmed intramuscular nerve ending. Second, although two-dimensional information on the injection site was obtained, the depth was not measured. Since the FDS is located in the intermediate layer of the anterior forearm muscle, the appropriate injection depth can be estimated based on the results of a study that determined the location of the FDS muscle based on magnetic resonance imaging and ultrasonography [14]. Thus, for more accurate injections, using electrical stimulation or ultrasonography as guide to determine the depth closest to the motor point is highly recommended. Third, the study has a small sample size, analyzing only 24 arms from 12 fresh adult cadavers. Thus, anatomical variants in FDS muscle bellies and location of main nerve branches may not have been fully elucidated.
Conversely, the strength of this study is that the proximal and distal intramuscular nerve branches were considered when proposing the injection site for botulinum toxin in the FDS. In addition, two-dimensional location information was proposed, with the FDS driving line used as a reference, and the points involved did not deviate greatly from the FDS line; thus, the clinicians can easily identify the points.
Conclusions
In this study, we proposed two optimal injection sites for botulinum toxin based on the FDS driving line. The MBPs of the first and second main branches were located approximately 41.6% and 72.4% of the reference line, based on the FDS direction, respectively. These findings can help determine the optimal botulinum toxin injection site in the FDS. In addition, injections in these two areas can effectively treat finger spasticity and restore hand function.
Data Availability
All data generated or analyzed during this study are included in this published article.
References
Bickerton LE, Agur AM, Ashby P (1997) Flexor digitorum superficialis: locations of individual muscle bellies for botulinum toxin injections. Muscle Nerve 20:1041–1043. https://doi.org/10.1002/(sici)1097-4598(199708)20:8<1041::aid-mus18>3.0.co;2-y
Childers MK, Kornegay JN, Aoki R et al (1998) Evaluating motor end-plate-targeted injections of botulinum toxin type A in a canine model. Muscle Nerve 21(5):653–655. https://doi.org/10.1002/(sici)1097-4598(199805)21:5<653::aid-mus15>3.0.co;2-w
Ergün S, Ghoreishi Y, Hübner S et al (2023) Old name, new face: a systematic analysis of flexor digitorum superficialis muscle with chiasma antebrachii. Ann Anat 247:152052. https://doi.org/10.1016/j.aanat.2023.152052
Guzmán-Venegas RA, Araneda OF, Silvestre RA (2014) Differences between motor point and innervation zone locations in the biceps brachii. An exploratory consideration for the treatment of spasticity with botulinum toxin. J Electromyogr Kinesiol 24(6):923–927. https://doi.org/10.1016/j.jelekin.2014.07.012
Huber M (2003) Treatment of spasticity with Botulinum A Toxin, Pocket Atlas, 2nd edn. Saentis Verlag
Im S, Park JH, Son SK et al (2014) Does botulinum toxin injection site determine outcome in post-stroke plantarflexion spasticity? Comparison study of two injection sites in the gastrocnemius muscle: a randomized double-blind controlled trial. Clin Rehabil 28(6):604–613. https://doi.org/10.1177/0269215513514983
Kinnett D (2004) Botulinum toxin a injections in children: technique and dosing issues. Am J Phys Med Rehab 83(10 Suppl). https://doi.org/10.1097/01.phm.0000141131.66648.e9. S59-S64
Lepage D, Parratte B, Tatu L et al (2005) Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: applications for selective neurotomy and for botulinum toxin injection. Surg Radiol Anat 27(5):420–430. https://doi.org/10.1007/s00276-005-0012-9
Lundström E, Smits A, Terént A et al (2010) Time-course and determinants of spasticity during the first six months following first-ever Stroke. J Rehabil Med 42(4):296–301. https://doi.org/10.2340/16501977-0509
Malhotra S, Pandyan AD, Rosewilliam S et al (2011) Spasticity and contractures at the wrist after Stroke: time course of development and their association with functional recovery of the upper limb. Clin Rehabil 25(2):184–191. https://doi.org/10.1177/0269215510381620
Matsuzawa K, Edama M, Ikezu M et al (2021) The origin structure of each finger in the flexor digitorum superficialis muscle. Surg Radiol Anat 43:3–10. https://doi.org/10.1007/s00276-020-02522-7
Moore KL (2006) Clinically oriented anatomy, 5th edn. Lippincott Williams
Parratte B, Tatu L, Vuillier F et al (2002) Intramuscular distribution of nerves in the human triceps surae muscle: anatomical bases for treatment of spastic drop foot with botulinum toxin. Surg Radiol Anat 24(2):91–96. https://doi.org/10.1007/s00276-002-0022-9
Rodrigues J, Santos-Faria D, Silva J et al (2019) Sonoanatomy of anterior forearm muscles. J Ultrasound 22(3):401–405. https://doi.org/10.1007/s40477-019-00388-z
Shaari CM, George E, Wu BL et al (1991) Quantifying the spread of botulinum toxin through muscle fascia. Laryngoscope 101(9):960–964. https://doi.org/10.1288/00005537-199109000-00006
Sommerfeld DK, Eek EU, Svensson AK et al (2004) Spasticity after Stroke: its occurrence and association with motor impairments and activity limitations. Stroke 35(1):134–139. https://doi.org/10.1161/01.STR.0000105386.05173.5E
Standring S (2016) Gray’s anatomy, 41st edn. Elsevier
Thibaut A, Chatelle C, Ziegler E, Bruno MA, Laureys S, Gosseries O (2013) Spasticity after Stroke: physiology, assessment and treatment. Brain Inj 27(10):1093–1105. https://doi.org/10.3109/02699052.2013.804202
Won SY, Hur MS, Rha DW et al (2010) Extra- and intramuscular nerve distribution patterns of the muscles of the ventral compartment of the forearm. Am J Phys Med Rehab 89(8):644–652. https://doi.org/10.1097/PHM.0b013e3181d8a116
Acknowledgements
The authors would like to thank the Department of Anatomy at College of Medicine, the Catholic University of Korea, Seoul, Korea, for its cooperation.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
J P: Data collection, Data analysis, Manuscript writing/editingD S: Data collection YJ K: Protocol/project development.
Corresponding author
Ethics declarations
Ethical approval
All human tissue used in this study was obtained from fully consented donors. All procedures performed were in accordance with the ethical standards of the institutional review board (IRB) and with the 1964 Helsinki Declaration and its later amendments. No IRB approval required for this kind of study.
Consent to publish
All the authors gave consent for the publication of the report.
Conflict of interest
None of the authors has any conflict of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Park, J., Sohn, D. & Ko, Y.J. Anatomical location of motor branch points in the flexor digitorum superficialis for the injection site of botulinum toxin. Surg Radiol Anat 45, 1593–1597 (2023). https://doi.org/10.1007/s00276-023-03260-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-023-03260-2