
Abstract
Purpose
The flexor digitorum superficialis muscle (FDS) is considered the most important of the forearm flexors for maintaining elbow valgus stability. However, the relationships between the origin structure of each finger of the FDS and the anterior oblique ligament (AOL) of the ulnar collateral ligament and the common tendon (CT) in the proximal part, and morphological features are unclear. The purpose of this study was to clarify the relationships between the origin structure of each finger of the FDS and the AOL and the CT, as well as to clarify the morphological features of the muscle belly of each finger of the FDS.
Methods
This study examined 20 elbows. The origin of each finger was examined. Muscle mass, muscle fiber bundle length, and the pennation angle of each finger were also measured.
Results
In all cases, the third and fourth digits originated from the radius, the anterior common tendon (ACT), and the posterior common tendon (PCT). The second and fifth digits (18 elbows) or an independent fifth digit (2 elbows) originated from the ACT, the PCT, the AOL, and other soft tissues of the elbow. Muscle mass and muscle fiber bundle length in the muscle belly of the third and fourth digits were significantly heavier and longer, respectively, than in the muscle belly of the second and fifth digits.
Conclusion
Because the second and fifth digits or an independent fifth digit originated from the AOL, their contraction may cause tension in the AOL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ulnar collateral ligament (UCL) injuries are common in overhead-throwing athletes [25]. The mechanism of UCL injuries is thought to involve repeated valgus stress on the elbow during throwing motions [15]. The UCL is thought to be the primary static stabilizer against elbow valgus stress [20]. During pitching motions, the elbow is subject to a maximum of about 64 Nm of elbow valgus stress [9]. The UCL is reported to have a failure strength of about 34 Nm [2]. Therefore, elbow valgus stress during pitching motions exceeds the failure strength of the UCL, and the forearm flexors are thought to provide dynamic stabilization against elbow valgus stress [5, 6, 11, 12, 19, 22, 23, 27, 29]. Thus, elbow valgus stability provided by the forearm flexors is thought to be important for preventing UCL injuries.
An anatomical study reported that the forearm flexors are involved in valgus stability function depending on the positional relationship with the UCL [5, 10, 22]. In a biomechanical study, the contraction of the forearm flexors was involved in valgus stability function [4, 12, 19, 23, 29], and, in particular, the flexor digitorum superficialis muscle (FDS) was reported to be the most important of the forearm flexors [29]. In studies using ultrasound, the humero-ulnaris joint space decreased with finger flexion when loading elbow valgus stress, so the FDS was reported to be important for elbow valgus stability [13, 24]. Given the above, the FDS is important for elbow valgus stability, and FDS exercises are considered vital. Though the importance of FDS exercise was described in the previous studies [7, 14], there are a few studies of the methods of exercise [13].
An anatomical study of the FDS by Otoshi et al. reported that FDS muscle fibers originated directly from the anterior aspect of the medial epicondyle to the medial joint capsule, just over the anterior oblique ligament (AOL) of the UCL [22]. Furthermore, the FDS is composed of the deep layer and the superficial layer in the distal part; the deep layer is composed of the second and fifth digits of the FDS, and the superficial layer is composed of the third and fourth digits of the FDS [1, 21]. In recent years, some studies reported that a common tendon (CT) exists between the FDS and pronator teres and between the FDS and flexor carpi ulnaris [14, 22], and it is assumed that the forearm flexors transmit muscular power to the humero-ulnaris joint via the CT [14]. However, to the best of our knowledge, the relationships between the origin structure of each finger of the FDS and the AOL and between the origin structure of each finger of the FDS and the CT in the proximal part are not clear. If they were clear, it could lead to investigating the contraction of each finger of the FDS and how it is involved in the valgus stability function and through which tissues. Based on this, it is thought that examination of various contraction methods of the FDS could lead to the development of effective FDS exercises for the preventive care of UCL injuries. In addition, regarding the morphological features of the muscle, it has been reported that differences in muscle fiber bundle length and the pennation angle cause differences in the characteristics of muscle contraction [18].
The purpose of this study was to clarify the relationships between the origin structure of each finger of the FDS and the AOL, and between the origin structure of each finger of the FDS and the common tendon, and to clarify the morphological features of the muscle belly of each finger of the FDS. We hypothesized that the second and fifth digits are in the deep layer in the proximal part, and the second and fifth digits originate from the AOL, because the second and fifth digits are also in the deep layer in the distal part.
Methods
Cadavers
Twenty elbows from 12 Japanese cadavers (mean age at death, 82 ± 11 years; 12 sides from men, eight sides from women; nine right sides, 11 left sides) donated to the university anatomy program were examined. All cadavers were placed in 10% formalin and then dehydrated in alcohol. No sides showed signs of previous major surgery around the upper extremity.
Methods
This study referred to the previous studies for dissection [14, 22]. The gleno-humeral joint was sectioned to prepare an isolated upper limb. The skin and subcutaneous tissue were then removed (Fig. 1a). The muscle fibers of the palmaris longus muscle (PL), flexor carpi radialis muscle (FCR), pronator teres muscle (PT), and flexor carpi ulnaris muscle (FCU) were carefully removed from the anterior common tendon (ACT) [22] and the posterior common tendon (PCT) [22] (Fig. 1b). The flexor retinaculum and the tendinous insertion of the second-to-fifth digits of the FDS were incised at the wrist, and the origin was examined after separation from the distal to proximal muscle belly of each digit (Fig. 1c). As in the previous studies [1, 21], the deep layer of the FDS was composed of the second and fifth digits, and the superficial layer of the FDS was composed of the third and fourth digits in the distal part. In addition, in the proximal part, the muscle belly of the third and fourth digits covered the muscle belly of the second and fifth digits as a wrapping, and the two layers could be clearly separated when the connective tissue was carefully removed. Therefore, the muscle fibers were carefully inverted to the origin so as not to break them.

Structure of the forearm flexors (left side, medial view). a Forearm flexors after the skin and subcutaneous tissue are removed. b Muscle fibers of the palmaris longus muscle (PL), flexor carpi radialis muscle (FCR), pronator teres muscle (PT), and flexor carpi ulnaris muscle (FCU) are carefully removed from the anterior common tendon [22] and posterior common tendon [22], and c the tendinous insertions of the second-to-fifth digits of the FDS are incised at the wrist, separated from the distal to proximal muscle belly of each digit. MEC medial epicondyle of the humerus, FDP flexor digitorum profundus, P proximal, D distal, II second digit, III third digit, IV fourth digit, V fifth digit
Morphological measurements were performed by one examiner, and the measurements included muscle mass, muscle fiber bundle length, and the pennation angle. Muscle mass was measured using an electronic balance (Electronic Balance, Jinroom, Wuhan, China) after the muscle belly was removed and sufficiently immersed in storage solution. Muscle mass was calculated as a percentage of total FDS mass. This study referred to the previous studies for muscle fiber bundle length and the pennation angle [26, 30]. The muscle bundle was photographed using a digital camera (Finepix F600EXR; Fujifilm, Tokyo, Japan) after the muscle belly and the connective tissue were carefully removed. As the reference lines for measurement of the pennation angle, straight lines were made to connect the center of the width of the distal end of the tendinous insertion and the center of the width of the tendon at the point where the most distal muscle fiber attached to the tendinous insertion using a computer. The muscle fiber bundle length and the pennation angle were measured in the distal one-third, middle third, and proximal one-third portions of the muscle length, and the average value of the three points was calculated (Fig. 2). The pennation angle was defined as the angle of the muscle fiber bundle with respect to the reference line. In the case of a digastric muscle, the pennation angle in the muscle belly proximal to the intermediate tendon was measured as the angle of the muscle fiber bundle with respect to the straight line passing through the center of the width of the intermediate tendon, and in the muscle belly distal to the intermediate tendon, it was measured as the angle of the muscle fiber bundle with respect to the reference line. Muscle fiber bundle length and the pennation angle of each finger muscle belly were measured three times, and the average value and standard deviation were calculated. Measurements of the muscle fiber bundle lengths and the pennation angles were made using image analysis software (Image J; NIH, Bethesda, MD, USA). The intra-rater reliabilities of muscle fiber bundle length and pennation angle measurements were assessed using the intraclass correlation coefficient (ICC) (1, 3) for seven cadavers (mean age at death, 84 ± 12 years; ten elbows: three sides from men and seven sides from women) in this study. The ICC (1, 3) for the measurement of muscle fiber bundle length was 0.93–0.99, and that of the pennation angle was 0.94–0.99. Thus, sufficient reliability was obtained according to the criteria of Landis et al. [17].

Measurement of muscle fiber bundle length and the pennation angle (FDS of the left side). a Skin surface of the muscle belly, third digit and b bone surface of the muscle belly, second and fifth digits. Black line: reference line, Green line: muscle fiber bundle length. θ pennation angle, P proximal, D distal, II second digit, V fifth digit, Pennation angle the angle of the muscle fiber bundle with respect to the reference line (colour figure online)
Statistical analysis
Comparisons of muscle mass in each muscle belly were performed using paired t tests. Comparisons between the muscle fiber bundle length and the pennation angle in each digit were performed using one-way repeated-measures analysis of variance and Bonferroni’s method. Comparisons of the sexes were performed using Student’s t test. The level of significance was 5%.
Results
The origin structure of each finger in the FDS (Figs. 3, 4)

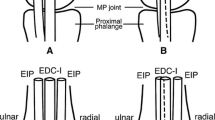
The origin structure of each finger in the FDS (left side, medial view). Aa The origin structure of the third and fourth digits. This originates from the radius, the anterior common tendon (ACT), and the posterior common tendon (PCT) (red line), with one muscle belly that divides into the third digit and fourth digit. White arrows: PCT. Bb The structure showing that the second and fifth digits have a common origin (18/20 elbows). This originates from the ACT, the PCT, the AOL, and the capsule of the elbow (red line), and divides into the second and fifth digits. The third and fourth digits are carefully removed from the ACT and the PCT (green paint), and the ACT and the PCT are inverted. Cc The structure showing that the second and fifth digits have a different origin (2/20 elbows). A muscle fiber originates from the tendon that connects to the ACT and becomes the tendinous insertion of the second digit (blue line), and a muscle fiber originates from the ACT, the PCT, the AOL, and the capsule of the elbow, and becomes the tendinous insertion of the fifth digit (red line). The third and fourth digits are carefully removed from the ACT and the PCT (green paint), and the ACT and the PCT are inverted. MEC medial epicondyle of the humerus, II second digit, III third digit, IV fourth digit of the FDS, V fifth digit, P proximal, D distal (colour figure online)

The structure around the FDS (left side, medial view). a In the structure showing that the second and fifth digits have a common origin (18 elbows, Fig. 3Bb), the muscle fibers of the second and fifth digits are removed. b In the structure showing that the second and fifth digits have a different origin (two elbows, Fig. 3Cc), the muscle fibers of the fifth digit are removed. ACT anterior common tendon, PCT posterior common tendon, *Anterior oblique ligament of the ulna collateral ligament, II second digit, P proximal, D distal
In all cases, the third and fourth digits originated from the radius, the ACT, and the PCT, with one muscle belly that divided into the third and fourth digits. On the other hand, a difference was observed for the second and fifth digits. In one type (18/20 elbows), the muscle fibers originated from the ACT, the PCT, the AOL, and the other soft tissues of the elbow and divided into the second and fifth digits. In the other type (2/20 elbows), a muscle fiber originated from the tendon that connected to the ACT and became the tendinous insertion of the second digit, and a muscle fiber originated from the ACT, the PCT, the AOL, and the other soft tissues of the elbow and became the tendinous insertion of the fifth digit.
Morphological characteristics (Tables 1, 2, 3)
Muscle mass was measured by dividing it into the third and fourth digits and the second and fifth digits, because the FDS was divided into each muscle belly. Muscle mass was calculated as the ratio of each muscle belly to the total mass of the FDS. Muscle mass was significantly greater in the muscle belly of the third and fourth digits than in the muscle belly of the second and fifth digits (p < 0.01).
The muscle belly of the third and fourth digits was divided into parts for the third digit and the fourth digit. The muscle belly of the second and fifth digits was composed of a digastric muscle. The second digit and the fifth digit had a common muscle belly proximal to the intermediate tendon, or the second digit and the fifth digit had their respective muscle bellies and a tendinous insertion distal to the intermediate tendon. The muscle belly of the independent fifth digit was also composed of a digastric muscle. Therefore, measurements were made of the third digit, fourth digit, the muscle belly proximal to the intermediate tendon (hereinafter called “digastric”), second digit, and fifth digit. For muscle fiber bundle length, the third digit and fourth digit were measured on the skin surface of the muscle belly, and the second and fifth digits or the second digit, the fifth digit, and the digastric were measured on the bone surface of the muscle belly. Muscle fiber bundle length was significantly longer in the third digit than in the second digit, fifth digit, and the digastric (p < 0.01). Muscle fiber bundle length was significantly longer in the fourth digit than in the second digit, fifth digit, and the digastric (p < 0.01). No significant differences in the pennation angle were seen among the muscle bellies of each finger (p > 0.05).
With respect to sex differences, the muscle fiber bundle length of the fifth digit was significantly longer in men than in women (p < 0.05).
Discussion
This study clarified the relationships between the origin structure of each finger of the FDS and the AOL and between the origin structure of each finger of the FDS and the CT. In addition, this study measured muscle mass, the muscle fiber bundle length, and the pennation angle, and clarified the differences in each muscle belly and between the sexes.
Otoshi et al. reported that the FDS muscle fibers originated directly from the anterior aspect of the medial epicondyle to the medial joint capsule, just over the AOL [22]. However, their study did not examine the origin structure of the FDS separately for each digit. The present study examined the origin structure of the FDS separately for each digit, and showed that the second and fifth digits or an independent fifth digit originated from the AOL. Therefore, contraction of the second and fifth digits or an independent fifth digit may cause tension in the AOL. In addition, Hoshika et al. [14] reported that forearm flexors transmit muscular power to the humero-ulnaris joint via the CT. Therefore, it appears that the contraction of all fingers can be involved in humero-ulnaris joint stability via the CT.
In addition, UCL reconstruction has been done with methods using a muscle splitting approach. Muscle splitting is done in the posterior one-third of the common flexor mass, because the UCL lies under the common flexor mass [28]. Based on the present study, the FDS that is located superficial in the AOL could be split. FDS exercises have been recommended for rehabilitation after UCL reconstruction [7]. A previous study using rats reported that, in the lateral collateral ligament of the elbow–capsule complex injury model, soft-tissue adhesions, and synovial proliferation occurred [16]. The current study showed that the second and fifth digits or an independent fifth digit originated from the AOL. Therefore, UCL injury and the invasion of UCL reconstruction appear to cause adhesions of the AOL and the second and fifth digits or an independent fifth digit. Therefore, exercises of the second and fifth digits or an independent fifth digit are an important focus for rehabilitation after UCL reconstruction.
Based on the present results for the morphological features, muscle mass was significantly greater in the muscle belly of the third and fourth digits than of the second and fifth digits. Furthermore, muscle fiber bundle length was significantly longer in the third digit and fourth digit than in the second digit and fifth digit. In a previous study, the physiological cross-sectional area (PCSA) was calculated according to the following equation [30]:
where θ is the pennation angle, and ρ is muscle density calculated in a previous study [30]. Therefore, following this equation, no significant differences were seen between the PCSA in the third and fourth digits and that in the second and fifth digits, considering the effect of architecture using an example of two muscles with identical PCSAs and pennation angles, but different lengths. It is considered that the PCSAs are equal, but muscle fiber bundle lengths are different (long fibers and short fibers), and maximum tensions are the same, because the PCSAs are the same, but the long fibers can demonstrate maximum tension over a wider muscle active range (i.e., active range of motion) [18]. Furthermore, in relation to muscle velocity, the long fibers can demonstrate greater muscle strength when muscle maximum contraction velocity increases [18]. Therefore, it appears that the third and fourth digits can demonstrate maximum tension in a wider active range of motion than the second and fifth digits.
With respect to sex differences, the muscle fiber bundle length of the fifth digit was significantly longer in men than in women. It is unclear why there was a sex difference only in the muscle fiber bundle length of the fifth digit. However, it appears that one of the factors that causes a sex difference is that normalization based on physical constitutional differences was not performed.
Based on the origin structure and morphological features found in the present study, it is necessary to consider the second and fifth digits and the third and fourth digits separately, because the origins of the second and fifth digits and of the third and fourth digits were different, and the features of muscle contraction of the second and fifth digits and of the third and fourth digits were different. In the future, it will be necessary to clarify whether muscle contractions of the second and fifth digits and of the third and fourth digits contribute to stabilization against elbow valgus stress. Furthermore, it is necessary to create effective FDS exercises based on this study, because there are a few studies regarding the methods of exercise of the FDS [13].
This study has three limitations. First, histological examinations could not be performed. Hoshika et al. [14] reported that the AOL could be interpreted as part of the complex including the tendinous septa and deep aponeurosis of the FDS. Because only gross anatomical examination was performed, soft tissue that could not be included in the AOL, the ACT, and PCT were considered “other soft tissues”. Second, measurement of muscle fiber bundle length could not be normalized to sarcomere length. A previous study reported that muscle fiber bundle length depends on the fixed position of the joint, so that normalization by sarcomere length is required [8]. However, in most cadavers used in the present study, the elbow was in a slightly flexed position and a forearm pronated position. This study examined only the FDS, and comparison was performed within the same muscle. Therefore, it is considered that the comparison was performed under the same conditions. Third, regarding the variation of the FDS, Belbl et al. [3] reported that there were cases of an absent flexor digitorum profundus muscle and variant FDS. However, no such cases were found in the current study. In the future, an increased number of samples will need to be examined.
Conclusion
In all cases, the third and fourth digits of the FDS originated from the radius, the ACT, and the PCT, with one muscle belly that divided into the third digit of the FDS and the fourth digit of the FDS. On the other hand, a difference was observed in the second and fifth digits of the FDS. One type originated from the ACT, the PCT, the AOL, and the capsule of the elbow and divided into the second digit of the FDS and the fifth digit of the FDS, whereas in another type, the muscle fibers originated from the tendon that connected to the ACT and became the tendinous insertion of the second digit of the FDS, and the muscle fibers originated from the ACT, the PCT, the AOL, and the capsule of the elbow and became the tendinous insertion of the fifth digit of the FDS.
Therefore, the contraction of the second and fifth digits or an independent fifth digit may cause tension in the AOL, because they originate from the AOL.
References
Agee J, McCarroll HR, Hollister A (1991) The anatomy of the flexor digitorum superficialis relevant to tendon transfers. J Hand Surg 16:68–69
Ahmad CS, Lee TQ, ElAttrache NS (2003) Biomechanical evaluation of a new ulnar collateral ligament reconstruction technique with interference screw fixation. Am J Sports Med 31:332–337. https://doi.org/10.1177/03635465030310030201
Belbl M, Kunc V, Kachlik D (2020) Absence of flexor digitorum profundus muscle and variation of flexor digitorum superficialis muscle in a little finger: two case reports. Surg Radiol Anat. https://doi.org/10.1007/s00276-020-02420-y
Buffi JH, Werner K, Kepple T, Murray WM (2015) Computing muscle, ligament, and osseous contributions to the elbow varus moment during baseball pitching. Ann Biomed Eng 43:404–415. https://doi.org/10.1007/s10439-014-1144-z
Davidson PA, Pink M, Perry J, Jobe FW (1995) Functional anatomy of the flexor pronator muscle group in relation to the medial collateral ligament of the elbow. Am J Sports Med 23:245–250. https://doi.org/10.1177/036354659502300220
Digiovine NM, Jobe FW, Pink M, Perry J (1992) An electromyographic analysis of the upper extremity in pitching. J Shoulder Elb Surg 1:15–25. https://doi.org/10.1016/s1058-2746(09)80011-6
Ellenbecker TS, Wilk KE, Altchek DW, Andrews JR (2009) Current concepts in rehabilitation following ulnar collateral ligament reconstruction. Sports Health 1:301–313. https://doi.org/10.1177/1941738109338553
Felder A, Ward SR, Lieber RL (2005) Sarcomere length measurement permits high resolution normalization of muscle fiber length in architectural studies. J Exp Biol 208:3275–3279. https://doi.org/10.1242/jeb.01763
Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF (1995) Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 23:233–239. https://doi.org/10.1177/036354659502300218
Frangiamore SJ, Moatshe G, Kruckeberg BM, Civitarese DM, Muckenhirn KJ, Chahla J, Brady AW, Cinque ME, Oleson ML, Provencher MT, Hackett TR, LaPrade RF (2018) Qualitative and quantitative analyses of the dynamic and static stabilizers of the medial elbow: an anatomic study. Am J Sports Med 46:687–694. https://doi.org/10.1177/0363546517743749
Glousman RE, Barron J, Jobe FW, Perry J, Pink M (1992) An electromyographic analysis of the elbow in normal and injured pitchers with medial collateral ligament insufficiency. Am J Sports Med 20:311–317. https://doi.org/10.1177/036354659202000313
Hamilton CD, Glousman RE, Jobe FW, Brault J, Pink M, Perry J (1996) Dynamic stability of the elbow: electromyographic analysis of the flexor pronator group and the extensor group in pitchers with valgus instability. J Shoulder Elb Surg 5:347–354
Hoshika S, Nimura A, Takahashi N, Sugaya H, Akita K (2020) Valgus stability is enhanced by flexor digitorum superficialis muscle contraction of the index and middle fingers. J Orthop Surg Res 15:121. https://doi.org/10.1186/s13018-020-01640-7
Hoshika S, Nimura A, Yamaguchi R, Nasu H, Yamaguchi K, Sugaya H, Akita K (2019) Medial elbow anatomy: a paradigm shift for UCL injury prevention and management. Clin Anat 32:379–389. https://doi.org/10.1002/ca.23322
Jobe FW, Stark H, Lombardo SJ (1986) Reconstruction of the ulnar collateral ligament in athletes. J Bone Jt Surg [Am] 68:1158–1163
Lake SP, Castile RM, Borinsky S, Dunham CL, Havlioglu N, Galatz LM (2016) Development and use of an animal model to study post-traumatic stiffness and contracture of the elbow. J Orthop Res 34:354–364. https://doi.org/10.1002/jor.22981
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Lieber RL (2010) Skeletal muscle structure, function, and plasticity: the physiological basis of rehabilitation, 3rd edn. Lippincott Williams & Wilkins, Baltimore
Lin F, Kohli N, Perlmutter S, Lim D, Nuber GW, Makhsous M (2007) Muscle contribution to elbow joint valgus stability. J Shoulder Elb Surg 16:795–802. https://doi.org/10.1016/j.jse.2007.03.024
Morrey BF, Tanaka S, An KN (1991) Valgus stability of the elbow. A definition of primary and secondary constraints. Clin Orthop Related Res 265:187–195
Ohtani O (1979) Structure of the flexor digitorum superficialis. Okajimas Folia Anat Jpn 56:277–288
Otoshi K, Kikuchi S, Shishido H, Konno S (2014) The proximal origins of the flexor-pronator muscles and their role in the dynamic stabilization of the elbow joint: an anatomical study. Surg Radiol Anat 36:289–294. https://doi.org/10.1007/s00276-013-1168-3
Park MC, Ahmad CS (2004) Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Jt Surg Am 86-a:2268–2274
Pexa BS, Ryan ED, Myers JB (2018) Medial elbow joint space increases with valgus stress and decreases when cued to perform a maximal grip contraction. Am J Sports Med 46:1114–1119. https://doi.org/10.1177/0363546518755149
Rebolledo BJ, Dugas JR, Bedi A, Ciccotti MG, Altchek DW, Dines JS (2017) Avoiding tommy john surgery: what are the alternatives? Am J Sports Med 45:3143–3148. https://doi.org/10.1177/0363546517692548
Sacks RD, Roy RR (1982) Architecture of the hind limb muscles of cats: functional significance. J Morphol 173:185–195. https://doi.org/10.1002/jmor.1051730206
Sisto DJ, Jobe FW, Moynes DR, Antonelli DJ (1987) An electromyographic analysis of the elbow in pitching. Am J Sports Med 15:260–263. https://doi.org/10.1177/036354658701500314
Smith GR, Altchek DW, Pagnani MJ, Keeley JR (1996) A muscle-splitting approach to the ulnar collateral ligament of the elbow. Neuroanatomy and operative technique. Am J Sports Med 24:575–580. https://doi.org/10.1177/036354659602400503
Udall JH, Fitzpatrick MJ, McGarry MH, Leba TB, Lee TQ (2009) Effects of flexor-pronator muscle loading on valgus stability of the elbow with an intact, stretched, and resected medial ulnar collateral ligament. J Shoulder Elb Surg 18:773–778. https://doi.org/10.1016/j.jse.2009.03.008
Ward SR, Eng CM, Smallwood LH, Lieber RL (2009) Are current measurements of lower extremity muscle architecture accurate? Clin Orthop Relat Res 467:1074–1082. https://doi.org/10.1007/s11999-008-0594-8
Acknowledgements
The authors would like to acknowledge and thank those anonymous individuals who generously donated their bodies and so enabled this study to be performed. This study was supported by a Grant-in-Aid for Scientific Research (19K11358) from the Japan Society for the Promotion of Science (JSPS) and a Grant-in-Aid program from Niigata University of Health and Welfare (H30B05).
Author information
Authors and Affiliations
Contributions
KM: protocol/project development, data collection, data analysis, manuscript, writing/editing. ME: protocol/project development, data collection, data analysis, manuscript writing/editing. MI: data collection, manuscript writing/editing. FK: data collection, manuscript writing/editing. RH: data collection and manuscript writing/editing. IK: protocol/project development, data collection, data analysis, and manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All methods were carried out in accordance with the 1964 Declaration of Helsinki, and all cadavers were legally donated for research purposes to the Nippon Dental University of Life Dentistry at Niigata, Japan.
Informed consent
Informed consent was obtained from the families of all subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Matsuzawa, K., Edama, M., Ikezu, M. et al. The origin structure of each finger in the flexor digitorum superficialis muscle. Surg Radiol Anat 43, 3–10 (2021). https://doi.org/10.1007/s00276-020-02522-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-020-02522-7