
Abstract
Purpose
To analyze the correlation between notch width index (NWI) and/or femoral intercondylar notch width (NW) assessed by magnetic resonance imaging (MRI) and risk of anterior cruciate ligament (ACL) injury.
Methods
We searched the PubMed, Embase, China National Knowledge Infrastructure and Wanfang databases for literature reporting a correlation between ACL injury and NWI and/or NW. Subgroup analyses were stratified by ethnicity, sex and control source. The weighted mean difference (WMD) and 95% confidence intervals (95% CIs) were calculated for the ACL injury cases and controls using random- or fixed-effects models. Begg’s test and sensitivity analyses were applied to assess publication bias and stability of the results, respectively.
Results
Twenty-eight eligible studies were finally enrolled. The NW was significantly narrowerin the ACL injury cases than in the control cases (pooled WMD, − 1.88 [95% CI, − 2.43 to − 1.32]). The results were similar when stratified by ethnicity and sex. Similarly, the NWI was lower in ACL injury cases than in the controls. Asian populations presented similar results when stratified by ethnicity, among the self-control group when stratified by control source, and among men when stratified by sex. No publication bias was identified; however, the sensitivity analysis suggested unstable results in the NWI subgroup analysis.
Conclusions
The current meta-analysis evidenced that the NW assessed via MRI was significantly smaller in ACL injury cases than in the controls. The NWI was lower in ACL injury cases among men. Prevention strategies for ACL injury could be applied for people with intercondylar notch stenosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The anterior cruciate ligament (ACL) is important for maintaining stability of the knee joint. ACL injury may result in loss of forward and rotational stability of the knee joint, leading to secondary damage (i.e., meniscus and articular cartilage damage) [1]. Hence, evaluating and identifying risk factors for ACL injury as early as possible are of clinical importance.
The femoral intercondylar notch is a specialized anatomical structure that accommodates the anterior and posterior cruciate ligaments and the tibial intercondylar spine. It exerts a vital role in maintaining knee joint stability. The shape and width of the intercondylar notch are largely affected by sex, age, height, and ethnicity [11, 21]. Everhart et al. found that women had narrower notches and higher rates of stenosis than did men. African–American men have narrower notches than Caucasian men. Height and notch width were found to be positively associated only among men [11]. Notch width index (NWI), initially proposed by Souryal et al., describes the intercondylar notch width [41]. NWI indicates the ratio of the femoral intercondylar width to that of the internal and external condyles at the plane of the popliteal tendon. NWI excludes most anatomical factors and height and weight interference; thus, it can accurately reflect the width and stenosis of the intercondylar notch. Numerous studies have explored the relationship between tibial slope and intercondylar notch dimensions, and anterior cruciate ligament injury [53, 54]. Many studies found that tibial slope and narrow intercondylar NW are risk factors for ACL injury [10, 46, 48], while others have shown that NW does not affect ACL injury [47, 54].
Intercondylar notch is analyzed by plain radiographs, computed tomography (CT) and magnetic resonance imaging (MRI) measurements. Radiographic measurements of the intercondylar notch are sometimes inaccurate even under optimal conditions, including correction technology, projection, and magnification [4]. CT shows stable reliability between observers when measuring the femur and tibia [34]. However, because of radiation, CT use in ACL imaging is limited. MRI is more accurate than are plain radiographs, with similar accuracy to that of CT [34]. MRI has high contrast resolution for soft tissue and enables clear distinguishing of the meniscus, cruciate ligament and articular cartilage of the knee joint and can yield multiple imaging parameters [31]. MRI exerts relatively high sensitivity and specificity in diagnosing ACL injuries [8, 18].
This meta-analysis explored the relationship between the intercondylar notch dimension assessed via MRI, including NW and NWI, and the risk of anterior cruciate ligament injury. We hypothesized that MRI intercondylar notch stenosis measured via MRI was a risk factor for ACL injury.
Methods
Search strategy
This meta-analysis was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) standards. Studies reporting a correlation between ACL injury and NWI and/or NW published before 30 June 2018 were searched in the PubMed, Embase, China National Knowledge Infrastructure and Wanfang databases. The keywords “intercondylar notch” OR “notch width” OR “notch width index”and “anterior cruciate ligament” were searched. Two investigators independently and manually reviewed the studies reporting ACL and NW/NWI and their reference lists.
Inclusion and exclusion criteria
Inclusion criteria were (1) observational research, including case–control or prospective studies; (2) NWI and/or NW were exposure factors and assessed via MRI; and (3) ACL was the interest outcome. Exclusion criteria were (1) controls or ACL injury cases only; (2) lacking the mean, standard deviation (SD) or confidence interval (CI); (3) reviews, letters, abstracts or animal experiments; and (4) no MRI was conducted.
Data extraction
Two investigators independently extracted the baseline characteristics and results in the included studies. A third investigator resolved any disagreements. The following information was collected: name of first author, publishing year, nationality, ethnicity, age, case resource, control resource, study design, and the mean ± SD of the main indicators (NW and/or NWI).
Statistical analyses
Data were analyzed and managed using Stata 12.0 (StataCorp., College Station, Texas, USA). The case and control groups were assigned according to ACL injury. NW and/or NWI examined via MRI were the exposure factors, and their weighted mean difference (WMD) and corresponding 95% confidence interval (95% CI) were recorded. Heterogeneity among the enrolled literature was assessed via Chi square tests and q tests. The Mantel–Haenszel fixed-effects method or the DerSimonian and Laird random-effects method were used to assess the WMD and 95% CI. Subgroup analyses were conducted based on ethnicity, sex and control source. Begg’s and Egger’s tests were performed to detect publication bias. Sensitivity was analyzed to examine the stability of our results. P < 0.05 was considered statistically significant.
Results
Baseline characteristics
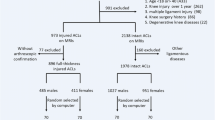
Of the 1,792 studies retrieved from the databases, 82 were selected for full-text review. Finally, 28 eligible studies were enrolled. Figure 1 shows a diagram of the literature screening. Among the 28 enrolled studies, 22 were published in English [3, 5, 6, 8, 12, 13, 16,17,18, 22, 29, 32, 33, 35, 36, 38, 39, 42, 44, 45, 51, 56], 5 were published in Chinese [19, 24, 27, 55, 57], and one was a dissertation in Chinese [26]. Patients with noncontact ACL injury were defined as the case group; these subjects exhibited noncontact ACL injuries, and patients in four studies also presented knee osteoarthritis (KOA). The population without ACL injury was defined as the control group. Controls were divided into healthy controls, patients with KOA only, self-controls (ACL injury on one side of the subject, normal on the other) and other patients (those with meniscal injuries or a diagnosis of patellofemoral pain but no ACL injury). Subjects ranged in age from 20–60 years. There were one prospective cohort study and 27 case–control studies. Eighteen studies reported NW data, and 21 reported NWI data. Table 1 lists the baseline characteristics for these studies.

Flow diagram for enrolled studies
NW and risk of ACL injury
Eighteen articles reported the relationship between NW and ACL, among which, three articles [33, 51, 56] distinguished the NW data between men and women, and these were divided into six studies according to sex. Finally, 21 studies were included in the meta-analysis (Fig. 2). NW was significantly narrower in ACL injury cases than in the overall controls (Table 2).

Forest plot for the intercondylar notch width and risk of anterior cruciate ligament injury. a Ethnicity subgroup analysis; b sex subgroup analysis. a, b Studies were divided into male and female group
Subgroup analyses were conducted based on ethnicity and sex. Further subgroup analysis showed that NW was smaller in ACL injury cases among Asian and Caucasian populations. Three articles supplied the NW data for both women and men [33, 51, 56] and were divided into six studies. Four articles confirmed the subjects’ sex [3, 5, 29, 36]. Finally, ten studies were analyzed by sex subgroup for NW. NW was significantly narrower in ACL cases among women and men than in the control cases (Table 2).
No publication biases were identified by Begg’s test (P = 0.51 for overall and ethnicity subgroup analyses; P = 0.72 for sex subgroup analysis; Fig. 3) or Egger’s test (data not shown). Sensitivity analysis showed that the findings were robust (data not shown).

Funnel plot for the intercondylar notch width and risk of anterior cruciate ligament injury. a Ethnicity subgroup analysis; b sex subgroup analysis
NWI and risk of ACL injury
Twenty-one articles reported a correlation between NWI and ACL injury. Among them, two articles identified NWI in men and women [33, 56], and one contained both healthy controls and KOA controls [16]. These three articles were divided into six studies. Finally, 24 studies were subjected to meta-analysis (Fig. 4a). In the overall analysis, the NWI was significantly narrowerin ACL cases than in the controls (Table 3).

Forest plot for the intercondylar notch width index and risk of anterior cruciate ligament injury. a Ethnicity subgroup analysis; b source of controls subgroup analysis; c sex subgroup analysis. a, b Studies were divided into male and female group. 1, 2 studies were divided into healthy control and KOA control
Subgroup analyses were performed on ethnicity, control source and sex (Table 3 and Fig. 4). NWI was significantly lower in ACL injury cases among Asian populations and others stratified by ethnicity. When stratified by control source, NWI was significantly lower in ACL injury cases than in self-control cases (Fig. 5). Eight studies were subjected to subgroup analysis by sex; a significant difference was found among men.

Funnel plot for the intercondylar notch width index and risk of anterior cruciate ligament injury. a Ethnicity subgroup analysis; b source of controls subgroup analysis; c sex subgroup analysis
No publication biases were identified by Begg’s test (P = 0.083 for the overall, ethnicity subgroup, and control source subgroup analyses; P = 0.53 for the sex subgroup analysis) or Egger’s test (data not shown). After removing one study [5], sensitivity analysis identified a significant difference for NWI results in the Caucasian population, healthy controls and women.
Discussion
Internal factors that determine the risks for ACL injury include anatomical features of the pelvis and femur, intercondylar notch width, posterior slope at the medial plateau, Q angle, joint relaxation and flexibility, and hormone differences [9, 20]. The narrow intercondylar notch angle can lead to impact from forward translation forces and forced knee valgus, which can promote ACL injury [2]. The increased posterior tibial slope may promote ACL injury by increasing anterior motion of the tibia relative to the femur or intense quadricep contraction, or increasing torsional loads in cases of differences in the medial and lateral tibial slopes [14]. Two-dimensional parameters of the femoral notch are widely used because they are convenient to measure. However, they only represent the dimension at one notch location; thus, they cannot fully reflect the overall dimension and may lead to measurement bias [50]. Three-dimensional notch volume can reflect the overall dimension; however, owing to its high technical threshold and tedious measurement, its application is limited.
Two-dimensional notch parameters, including NW and NWI, are often used to evaluate femoral notch size. In most cases, two-dimensional parameters can effectively evaluate the notch size [50]. Femoral NW and NWI were often used to assess the risk of ACL injury, but the conclusions in each study were controversial [25]. To comprehensively understand how the NWI affects ACL injury, we enrolled 28 relevant studies and performed a meta-analysis.
The NW was markedly narrower in ACL injury cases than in the controls. Subgroup analyses stratified by ethnicity and sex yielded similar results. Intercondylar notch stenosis can result in ACL injury. A narrow femoral intercondylar notch can easily induce impact between the ACL and lateral wall of the femoral intercondylar bones once the knee joint is over-bent or rotated, which is much more pronounced at the position of flexion-valgus and external rotation. Frequent impact and friction easily damage the ACL fiber bundles, which cannot easily handle large external forces [12, 15]. Stijak et al. [43] and Dienst et al. [7] considered that the intercondylar notch volume is consistent with that of the ACL it contains. People with intercondylar notch stenosis present an ACL with a smaller volume, weaker strength and worse biomechanical properties and are highly susceptible to ACL rupture. Nevertheless, some studies found no significant correlation between intercondylar notch volume and that of the ACL contained within [28, 37]. In the current analysis, the NW was narrower in ACL injury cases, which may predict ACL injury. Notably, intercondylar notch width varies greatly among individuals, possibly owing to measurement methods, measurement planes or ethnicity.
NWI is an advantageous indicator that eliminates the influences of height, weight and sex and avoids individual differences and measurement errors. The critical value for NWI differed in the relevant literature because of different measurement methods, subject positions and sample sizes. In the current analysis, NWI was smaller in the ACL injury cases than in the controls. Subgroup analyses based on ethnicity revealed that the NWI was smaller in ACL injury cases among Asian and other populations. Uhorchak et al. [47] suggested that an NWI of < 0.18 would increase the risk factor of the ACL, which was 0.19 in LaPrade’s study [23]. Domzalski et al. [8] pointed out that the average NWI in ACL injury cases is 0.24, and NWI decreases with age. Souryaland Freeman [40] reported that the NWI in healthy controls was 0.231 ± 0.044 and that an NWI < 0.20 will significantly enhance the risk of bilateral ACL injury. Souryal et al. [41] recorded NWI in a 45° kneeling position via X-ray across many healthy populations. The average NWI was 0.231 ± 0.004, suggesting that an NWI ≤ 0.20 indicated severe stenosis of the intercondylar notch. Muneta et al. [30] found no significant difference in ACL volume between people with NWI > 0.20 and those with NWI < 0.20. Simon et al. [38] demonstrated that the direction of muscle travel in the ACL was closer to vertical under the pathological condition of intercondylar notch stenosis. Vertical travel direction space larger loads on the ACL and are prone to ACL injury. ACL injury is thought to be more frequent in female athletes than in male athletes, and sex influences many anatomical parameters (i.e., NWI and NW). Compared with men, women have a smaller NW and are more susceptible to ACL injury [52]. However, hormone levels, neuromuscular levels and biomechanics are all potential factors that influence ACL injury [2, 29]. Van et al. revealed no significant difference in NWI between men and women, possibly owing to different inclusion criteria and measurement methods [49]. Here, we found NWI was lower in ACL injury cases among men. Notably, when stratified by control source, subgroup analyses identified a lower NWI in ACL injury cases in the self-control group only, suggesting that the two studies including self-controls may have affected the overall results.
This analysis had some limitations. First, the included literature was significantly heterogeneous, and some resources were unclear even after subgroup and sensitivity analyses, likely owing to different measurement methods and examination planes. To get accurate measurements, the NW and corresponding NWI of different parts of the notch should implement a unified standard. These measurements should include the notch entry width (nw_-in), the exit width (nw_-ou), and the ACL attachment (nw_-aa) [56]. Second, most studies in this meta-analysis were case–control studies, and only one was a prospective cohort study. Thus, the results may have been due to ACL injury and intercondylar notch stenosis. Some other factors may have affected our findings. Third, the study by Bouras et al. [5] may have affected the stability of our findings; this study included many cases with women, and no significant correlation was found between NWI and ACL injury. Fourth, although no significant publication biases were identified, relevant studies published in languages other than English and Chinese were lacking, and some negative results may have been missing. Finally, the small sample size in this analysis likely influenced the reliability of our findings.
Conclusion
The current meta-analysis evidenced that the NW assessed via MRI was significantly smaller in ACL injury cases than in controls. NWI was lower in ACL injury cases among men. Prevention strategies for ACL injury could be applied for people with intercondylar notch stenosis.
Data availability
Data and material are available in this submission.
References
Acevedo RJ, Rivera-Vega A, Miranda G, Micheo W (2014) Anterior cruciate ligament injury: identification of risk factors and prevention strategies. Current Sports Med Rep 13:186–191
Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lazaro-Haro C, Cugat R (2009) Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc 17:705–729
Alentorn-Geli E, Pelfort X, Mingo F, Lizano-Diez X, Leal-Blanquet J, Torres-Claramunt R, Hinarejos P, Puig-Verdie L, Monllau JC (2015) An evaluation of the association between radiographic intercondylar notch narrowing and anterior cruciate ligament injury in men: the notch angle is a better parameter than notch width. Arthrosc J Arthrosc Relat Surg 31:2004–2013
Anderson AF, Anderson CN, Gorman TM, Cross MB, Spindler KP (2007) Radiographic measurements of the intercondylar notch: are they accurate? Arthrosc J Arthrosc Relat Surg 23:261–268
Bouras T, Fennema P, Burke S, Bosman H (2018) Stenotic intercondylar notch type is correlated with anterior cruciate ligament injury in female patients using magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc 26:1252–1257
Chen C, Ma Y, Geng B, Tan X, Zhang B, Jayswal CK, Khan MS, Meng H, Ding N, Jiang J, Wu M, Wang J, Xia Y (2016) Intercondylar notch stenosis of knee osteoarthritis and relationship between stenosis and osteoarthritis complicated with anterior cruciate ligament injury: a study in MRI. Medicine 95:e3439
Dienst M, Schneider G, Altmeyer K, Voelkering K, Georg T, Kramann B, Kohn D (2007) Correlation of intercondylar notch cross sections to the ACL size: a high resolution MR tomographic in vivo analysis. Arch Orthop Trauma Surg 127:253–260
Domzalski M, Grzelak P, Gabos P (2010) Risk factors for anterior cruciate ligament injury in skeletally immature patients: analysis of intercondylar notch width using magnetic resonance imaging. Int Orthop 34:703–707
Estes K, Cheruvu B, Lawless M, Laughlin R, Goswami T (2015) Risk assessment for anterior cruciate ligament injury. Arch Orthop Trauma Surg 135:1437–1443
Evans KN, Kilcoyne KG, Dickens JF, Rue JP, Giuliani J, Gwinn D, Wilckens JH (2012) Predisposing risk factors for non-contact ACL injuries in military subjects. Knee Surg Sports Traumatol Arthrosc 20:1554–1559
Everhart JS, Flanigan DC, Chaudhari AM (2014) Anteromedial ridging of the femoral intercondylar notch: an anatomic study of 170 archival skeletal specimens. Knee Surg Sports Traumatol Arthrosc 22:80–87
Everhart JS, Flanigan DC, Simon RA, Chaudhari AM (2010) Association of noncontact anterior cruciate ligament injury with presence and thickness of a bony ridge on the anteromedial aspect of the femoral intercondylar notch. Am J Sports Med 38:1667–1673
Fernandez-Jaen T, Lopez-Alcorocho JM, Rodriguez-Inigo E, Castellan F, Hernandez JC, Guillen-Garcia P (2015) The importance of the intercondylar notch in anterior cruciate ligament tears. Orthop J Sports Med 3:2325967115597882
Feucht MJ, Mauro CS, Brucker PU, Imhoff AB, Hinterwimmer S (2013) The role of the tibial slope in sustaining and treating anterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 21:134–145
Fung DT, Hendrix RW, Koh JL, Zhang LQ (2007) ACL impingement prediction based on MRI scans of individual knees. Clin Orthop Relat Res 460:210–218
Geng B, Wang J, Ma JL, Zhang B, Jiang J, Tan XY, Xia YY (2016) Narrow intercondylar notch and anterior cruciate ligament injury in female nonathletes with knee osteoarthritis aged 41–65 years in plateau region. Chin Med J 129:2540–2545
Gormeli CA, Gormeli G, Ozturk BY, Ozdemir Z, Kahraman AS, Yildirim O, Gozukarab H (2015) The effect of the intercondylar notch width index on anterior cruciate ligament injuries: a study on groups with unilateral and bilateral ACL injury. Acta Orthop Belg 81:240–244
Hoteya K, Kato Y, Motojima S, Ingham SJ, Horaguchi T, Saito A, Tokuhashi Y (2011) Association between intercondylar notch narrowing and bilateral anterior cruciate ligament injuries in athletes. Arch Orthop Trauma Surg 131:371–376
Huang JM, Hu WJ, Li DC, Zhang Z, Wang HJ, Li YH, Cao JG, Zhao Q, Chen X (2016) Association of anterior cruciate ligament degeneration with medical meniscuss tear and intercondylar notch impingement. Chinese J Rep Reconst Surg 30:1478–1482
Huang M, Li Y, Guo N, Liao C, Yu B (2019) Relationship between intercondylar notch angle and anterior cruciate ligament injury: a magnetic resonance imaging analysis. J Inter Med Res 47:1602–1609
Ireland ML, Ballantyne BT, Little K, McClay IS (2001) A radiographic analysis of the relationship between the size and shape of the intercondylar notch and anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 9:200–205
K S, Chamala T, Kumar A (2019) Comparison of anatomical risk factors for noncontact anterior cruciate ligament injury using magnetic resonance imaging. J Clinic Orthop Traumatol 10:143–148
LaPrade RF, Burnett QM (1994) Femoral intercondylar notch stenosis and correlation to anterior cruciate ligament: injuries a prospective study. Am J Sports Med 22:198–202
Li H, Wu ZY, Wang DL (2017) Relationship between femoral intercondylar fossa, posterior tibial slope and anterior cruciate ligament injury. Chin J Bone Joint Injury 32:585–588
Li H, Zeng C, Wang Y, Wei J, Yang T, Cui Y, Xie D, Liu H, Lei GH (2018) Association between magnetic resonance imaging-measured intercondylar notch dimensions and anterior cruciate ligament injury: a meta-analysis. Arthrosc J Arthrosc Relat Surg 34:889–900
Li YL (2012) The intercondylar notch characteristics research on the signs of MRI and anterior cruciate ligament rupture. Master's thesis, Taishan Medical University, China
Liao Z, Cui H (2015) MRI measurement and its correlation between the femoral condyle and the femoral condyle after the rupture of the anterior vruciate ligament. Heilongjiang Med J 28:1218–1230
Lombardo S, Sethi PM, Starkey C (2005) Intercondylar notch stenosis is not a risk factor for anterior cruciate ligament tears in professional male basketball players: an 11-year prospective study. Am J Sports Med 33:29–34
Miljko M, Grle M, Kozul S, Kolobaric M, Djak I (2012) Intercondylar notch width and inner angle of lateral femoral condyle as the risk factors for anterior cruciate ligament injury in female handball players in Herzegovina. Coll Antropol 36:195–200
Muneta T, Takakuda K, Yamamoto H (1997) Intercondylar notch width and its relation to the configuration and cross-sectional area of the anterior cruciate ligament. A cadaveric knee study. Am J Sports Med 25:69–72
Nacey NC, Geeslin MG, Miller GW, Pierce JL (2017) Magnetic resonance imaging of the knee: an overview and update of conventional and state of the art imaging. J Magn Reson Imag 45:1257–1275
Ouyang X, Wang YH, Wang J, Hong SD, Xin F, Wang L, Yang XW, Wang JR, Wang LM, Wei BO, Wang Q, Cui WD, Fu XL (2016) MRI measurement on intercondylar notch after anterior cruciate ligament rupture and its correlation. Exp Ther Med 11:1275–1278
Park JS, Nam DC, Kim DH, Kim HK, Hwang SC (2012) Measurement of knee morphometrics using MRI: a comparative study between acl-injured and non-injured knees. Knee Surg Relat Res 24:180–185
Parkar AP, Adriaensen ME, Fischer-Bredenbeck C, Inderhaug E, Strand T, Assmus J, Solheim E (2015) Measurements of tunnel placements after anterior cruciate ligament reconstruction–a comparison between CT, radiographs and MRI. Knee 22:574–579
Pekala L, Podgorski M, Shukla A, Winnicka M, Biernacka K, Grzelak P (2019) Do variants of the intercondylar notch predispose children to the injury of the anterior cruciate ligament? Clin Anat 32:706–709
Rahnemai-Azar AA, Yaseen Z, van Eck CF, Irrgang JJ, Fu FH, Musahl V (2016) Increased lateral tibial plateau slope predisposes male college football players to anterior cruciate ligament injury. J Bone Joint Surg Am 98:1001–1006
Shelbourne KD, Davis TJ, Klootwyk TE (1998) The relationship between intercondylar notch width of the femur and the incidence of anterior cruciate ligament tears. a prospective study. Amer J Sports Med 26:402–408
Simon RA, Everhart JS, Nagaraja HN, Chaudhari AM (2010) A case-control study of anterior cruciate ligament volume, tibial plateau slopes and intercondylar notch dimensions in ACL-injured knees. J Biomech 43:1702–1707
Sonnery-Cottet B, Archbold P, Cucurulo T, Fayard JM, Bortolletto J, Thaunat M, Prost T, Chambat P (2011) The influence of the tibial slope and the size of the intercondylar notch on rupture of the anterior cruciate ligament. J Bone Joint Surg Br 93:1475–1478
Souryal TO, Freeman TR (1993) Intercondylar notch size and anterior cruciate ligament injuries in athletes. a prospective study. Am J Sports Med 21:535–539
Souryal TO, Moore HA, Evans JP (1988) Bilaterality in anterior cruciate ligament injuries: associated intercondylar notch stenosis. Am J Sports Med 16:449–454
Stein V, Li L, Guermazi A, Zhang Y, Kent Kwoh C, Eaton CB, Hunter DJ, Investigators OAI (2010) The relation of femoral notch stenosis to ACL tears in persons with knee osteoarthritis. Osteoarthr Cartil 18:192–199
Stijak L, Herzog RF, Schai P (2008) Is there an influence of the tibial slope of the lateral condyle on the ACL lesion? a case control study. Knee Surg Sports Traumatol 16:112–117
Stijak L, Bumbasirevic M, Kadija M, Stankovic G, Herzog R, Filipovic B (2014) Morphometric parameters as risk factors for anterior cruciate ligament injuries—a MRI case control study. Vojnosanit Pregl 71:271–276
Taneja AK, Miranda FC, Demange MK, Prado MP, Santos DCB, Rosemberg LA, Baroni RH (2018) Evaluation of posterior cruciate ligament and intercondylar notch in subjects with anterior cruciate ligament tear: a comparative flexed-knee 3D magnetic resonance imaging study. Arthroscopy J Arthrosc Relat Surg 34:557–565
Teitz CC, Lind BK, Sacks BM (1997) Symmetry of the femoral notch width index. Am J Sports Med 25:687–690
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P, Taylor DC (2003) Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 west point cadets. Am J Sports Med 31:831–842
van Diek FM, Wolf MR, Murawski CD, van Eck CF, Fu FH (2014) Knee morphology and risk factors for developing an anterior cruciate ligament rupture: an MRI comparison between ACL-ruptured and non-injured knees. Knee Surg Sports Traumatol Arthrosc 22:987–994
van Eck CF, Martins CA, Lorenz SG, Fu FH, Smolinski P (2010) Assessment of correlation between knee notch width index and the three-dimensional notch volume. Knee Surg Sports Traumatol Arthrosc 18:1239–1244
Van Eck CF, Martins CA, Kopf S, Lertwanich P, Fu FH, Tashman S (2011) Correlation between the 2-dimensional notch width and the 3-dimensional notch volume: a cadaveric study. Arthrosc J Arthrosc Relat Surg 27:207–212
Whitney DC, Sturnick DR, Vacek PM, DeSarno MJ, Gardner-Morse M, Tourville TW, Smith HC, Slauterbeck JR, Johnson RJ, Shultz SJ, Hashemi J, Beynnon BD (2014) Relationship between the risk of suffering a first-time noncontact ACL Injury and geometry of the femoral notch and ACL: a prospective cohort study with a nested case-control analysis. Am J Sports Med 42:1796–1805
Wolters F, Vrooijink SH, Van Eck CF, Fu FH (2011) Does notch size predict ACL insertion site size? Knee Surg Sports Traumatol Arthrosc 19(Suppl 1):S17–21
Zeng C, Cheng L, Wei J, Gao SG, Yang TB, Luo W, Li YS, Xu M, Lei GH (2014) The influence of the tibial plateau slopes on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 22:53–65
Zeng C, Gao SG, Wei J, Yang TB, Cheng L, Luo W, Tu M, Xie Q, Hu Z, Liu PF, Li H, Yang T, Zhou B, Lei GH (2013) The influence of the intercondylar notch dimensions on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 21:804–815
Zhang B, Geng B, Tan XY, Chen C, Yang LJ, Wang J, Wang CF, Xia YY (2015) Relationship between first-time noncontact ACL injury and geometry of the femoral intercondylar notch: a highresolution MRI research. Orthopedic J China 23:1888–1892
Zhang C, Zhang X, Fang Z, Wang F, Yuan F, Xie G, Zhao J (2019) The correlation between common 2D femoral notch parameters and 3D notch volume: a retrospective MRI study. BMC Musculoskelet Disord 20:146
Zhang PR, Xu B, Xu HG, Wang R, Zhang HY (2015) Association between intercondylar notch width and noncontact anterior cruciate ligament injury. Chin J Bone Joint Injury 30:1058–1061
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. ZL, CL, LL, and PW prepared the material and collected and analyzed the data. ZL wrote the first draft of the manuscript, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, Z., Li, C., Li, L. et al. Correlation between notch width index assessed via magnetic resonance imaging and risk of anterior cruciate ligament injury: an updated meta-analysis. Surg Radiol Anat 42, 1209–1217 (2020). https://doi.org/10.1007/s00276-020-02496-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-020-02496-6