
Abstract
Purpose
In our study, we aimed to determine the topographic analysis of sternal foramen cases incidentally detected in patients underwent thoracic computed tomography.
Materials and methods
Patients aged 18 and over who were admitted to the thoracic surgery outpatient clinic for various reasons and underwent thoracic computed tomography (CT) between January 1, 2018 and January 1, 2019 were evaluated retrospectively. Thoracic CT scans of all patients with sternal foramen were evaluated by applying 3D bone configuration to evaluate foramina in the sternum and ribs. The data obtained were analyzed statistically by SPSS (Statistical Package for Social Sciences Version 21.0).
Results
Nine hundred and twelve patients were evaluated and sternal foramen prevalence was found to be 8.44% in our study. Of the 68 patients included in the study, 48 were male and 20 were female. The sternal foramen was localized in the corpus in 66.2% of the patients, whereas it was localized in xiphoid in 33.8%. Nine patients had scoliosis deformity and three patients had foramen in the rib.
Conclusion
Sternal foramen is a more common defect than thought, and should be kept in mind in clinical practice to prevent complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The sternum emerges in the form of two sternal bars consisting of mesenchymal tissue at the sixth week of fetal life and these bars begin to meet craniocaudally in the midline from the tenth week of fetal life. The connecting bars usually begin to ossify at six points from the 5th to 6th month of pregnancy. Ossification initially starts from the manubrium and corpus extending to the xiphoid and lasts until puberty. Each bone segment from which ossification begins is called the sternebra and usually six are present in the sternum. It may take up to 25 years for these sternabras to fully fuse from top to bottom. Failure to connect the sternal bars to the midline in the fetal period may result in multiple ossification centers, which may cause the development of oval shaped sternal foramina [3, 4, 7, 8, 14].
Sternal foramen (SF) was first described in 1707 [2, 7]. It has been reported in the conducted studies to be an isolated anomaly in the caudal part of the corpus stern, with a prevalence of 2.5–18.3% [1,2,3,4, 7, 8, 10, 12, 14, 16]. Previous studies usually include case reports or cadaver examinations [8, 9, 11,12,13]. Previous CT studies usually include radiology examinations performed in limited time periods [4, 6, 10, 14]. In our study, we aimed to topographically evaluate sternal foramen cases that were detected incidentally in the thoracic surgery outpatient clinic for a period of 1 year.
Materials and methods
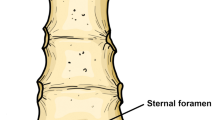
Patients aged 18 and over who were admitted to the thoracic surgery outpatient clinic for various reasons and underwent thoracic computed tomography (CT) between January 1, 2018 and January 1, 2019 were evaluated retrospectively. Patients who had sternal foramen detected in their CT were included in the study. Thoracic CT scans of all patients with sternal foramen were evaluated by applying 3D bone configuration to evaluate foramina in the sternum and ribs (Fig. 1). Patients who could not perform foramen measurements with thoracic CT or 3D bone configuration were excluded from our study.

a Sternal and costal foramen, b sternal foramen
Patients included in the study were first evaluated for age, sex, and known bone and skeletal system pathologies. The diameters of the detected sternal foramina were measured transversely and vertically in the coronal section of the thoracic CT bone window (Fig. 2). The sternal section where the sternal foramen is located, presence of accompanying costal foramen, the thickness of the bone with the foramen, subcutaneous fatty tissue thickness on the bone with foramen, thickness of tissue from the skin to intrathoracic area and intrathoracic organ under the foramen were detected (Fig. 3).

Measurement of transverse and vertical diameter of sternal foramen

Measurement of bone width, subcutaneous adipose tissue and distance from skin to intrathoracic area in thorax CT
The data obtained were analyzed statistically by SPSS (Statistical Package for Social Sciences Version 21.0). The data were checked with the Kolmogorov Smirnov test for normality. Skewness and Kurtosis data in the lower fractures of the analysis were analyzed. Independent samples t test and Mann–Whitney U test were used for group comparisons. The correlations between categorical variables were investigated by Fisher’s exact test, while the correlations between quantitative variables were investigated by Pearson correlation coefficient. In all statistical analyzes, those with p values less than 0.05 were considered significant.
Our study complies with the Helsinki Declaration. In our study, having the approval of Balıkesir University Faculty of Medicine Clinical Research Ethics Committee (Decision No: 2019/46) taken, our biggest limitation was the inability to perform a comparative topographic analysis as a result of not being able to get the general body measurements of the patients.
Results
In our study, 912 patients (574 males and 338 females) who were admitted to the outpatient clinic for various reasons and underwent thoracic CT were evaluated. Among these patients, while 77 patients with sternal foramen were evaluated, 9 (seven males and two females) of them were excluded from the study due to the lack of measurement from thoracic CT. The prevalence of sternal foramen was found to be 8.44% in our study.
Of the 68 patients included in the study, 48 (70.6%) were male and 20 (29.4%) were female. The mean age of the patients included in the study was 46.16 (± 15.34) years. Nine patients had scoliosis deformity and three patients had foramen in the rib. In three cases who had foramen in the rib, foramina was detected in the right ribs and was located in the anterior part of the corpus of the ribs. The sternal foramen was localized in the corpus in 66.2% of the patients, whereas it was localized in xiphoid in 33.8% (Table 1).
While it was found that the mean transverse width of the foramena located in corpus was 4.55 ± 2.04 and the vertical width was 6.48 ± 3.89; the mean transverse width of the foramena located in the xiphoid was found to be 5.39 ± 2.33, and the vertical width was 8.80 ± 4.39. While no statistically significant difference was detected between foramen localization and transverse width of foramen (p = 0.133), vertical width was detected to be significantly wider in foramena located in the xiphoid than those located in the corpus (p = 0.029).
While no statistically significant difference was detected between foramen transverse and vertical widths and sex, bone width was significantly higher in men, subcutaneous fatty tissue thickness and distance from skin to intrathoracic area were significantly higher in women (Table 2).
When the correlation between the transverse and vertical widths of the foramina and the width of the bone was investigated, it was detected that as the bone width decreased, the transverse and vertical widths of the foramen were significantly wider (Table 3).
Discussion
The sternal foramen is usually an oval-shaped defect originating from the manubrium, corpus or xiphoid part of the sternum as a result of a defect that occurs during the fusion of the sternal bars that make up the sternum in the embryological life. SF are usually isolated defects and may rarely be accompanied by other congenital anomalies [12, 13]. There are studies showing the correlation with sternal cleft in the literature [5, 12, 14, 16].
The frequency of sternal foramen varies in the conducted studies. Gossner et al. [10] determined the incidence of SF as 4.5% in 352 patients with thoracic CT, while Gkantsinikoudis et al. [9] determined it as 14.6% SF in their examination of 35 dried cadaver specimens. In the literature the series with the highest incidence of sternal foramen, Xie et al. [15] determined the rate of SF as 57.7% in xiphoid during in their study of 41 cadaver specimens and 926 patients with thoracic CT. El-Busaid et al. [8] determined the SF prevalence as 13.8% in 82 cadaver specimens in Kenya population, whereas Paraskevas et al. [12] determined SF prevalence to be 18.3% in 60 cadaver specimens in the Greek population. In our study, we performed our scan using thoracic CT scan and found the frequency of SF to be 8.44% in 912 patients undergoing thoracic CT for various reasons.
While the mean age showed a variability between 55 and 77 in cadaver studies, it showed a variability between 45 and 69.5 in CT studies. No significant correlation was found when the correlation between sex and SF was investigated [4, 6, 9, 10, 12]. In our study, the mean age was 46.16 and there was no statistically significant correlation detected between gender and the presence of SF.
Yekeler et al. [16] in their published series, while they detected SFs in 4.5% of all patients in the sternum corpus, they detected that 27.4% of the foramena were in xiphoid and none were in the manubrium. In the series with the highest prevalence published by Xie et al. [15], foramena were also detected in the xiphoid part of the sternum. El-Busaid et al. [8] detected foramen in the sternum corp and at the level of the fifth intercostal space in 77.8% of SF cadaver specimens. In our study, SFs were most commonly located in the sternum corpus with a percentage of 66.2%.
Sternal foramen sizes vary in various studies. Yekeler et al. [16] detected that the mean foramen width in the studies they conducted on the Turkish population was 6.5 mm (2–16 mm), while Gossner et al. [10] detected that the foramen width was 3.3 mm. Boruah et al. [6] also detected that the mean transverse diameter of SF was 5.58 mm while the vertical diameter was 6.66 mm. One of the largest SFs in the literature was detected in an anatomical cadaver in India with a transverse diameter of 11.4 mm and a vertical diameter of 20.8 mm [11]. In our study and similar to the literature, it was detected that the mean transverse diameter of the SFs in our study was 5.13 mm (0.8–15.3 mm) while the vertical diameter was 7.75 mm (1.1–20.1 mm). In addition, the foramen width was found to be larger as the bone width decreased, and the foramena located in the xiphoid were found to be wider in our study.
It is the intrathoracic tissue beneath the sternal foramena that makes them clinically important. Complications may occur especially in cases where the presence of foramen is not known during bone marrow biopsies or acupuncture applications. Pneumothorax may occur in case of the presence of the lungs under the foramen, intrathoracic haemorrhage, tamponade may occur in the presence of pericardium or heart, these injuries may even have mortal consequences [7, 9, 10, 12]. Bone marrow biopsies are usually made from the iliac bone and the sternum is the first choice in medical situations where the iliac bone cannot be used. In this case, complying with biopsy procedures alone is not enough to prevent the complication. In biopsies to be performed at the lower end of the sternum, a good evaluation or even control by ultrasonography is recommended [7]. Acupuncture is a reliable method and can be performed correctly with good education, since this condition is rarely met, good sternal anatomy knowledge is a must. Inclined insertion of the needle is recommended as a safe method but is not sufficient alone [4]. In our study, mostly the heart or pericardium was found under the foremen. None of our patients had a history of traumatic pathology due to foramen.
In traumatic pathology due to internal foramen, needle length, procedure and distance from skin to intrathoracic area are important. Gossner et al. [7] determined the mean distance from the skin to the intrathoracic area to be 49.6 mm, while Boruah et al. [6] determined the mean distance to be 21.53 mm. Babinski et al. [4] while they determined in their studies that the mean distance from the skin to the intrathoracic area was 37 mm, they specified that this distance was 34 mm in women and 42 mm in men. In our study, we determined that the mean distance from the skin to the intrathoracic area was 22.64 mm, while it was 27.27 mm in women and 20.95 mm in men. We detected that this difference between men and women was statistically significant. Although statistically significant bone width was higher in men, the fact that subcutaneous fatty tissue was significantly higher in women caused this difference.
Conclusion
When literature is reviewed, it is found that sternal foramen is a sternal defect that is not as rare as thought. This asymptomatic defect is more important when considering the internal bone marrow biopsies, acupuncture applications, traumas to the anterior chest wall and the forensic conditions caused by them. Therefore, it should be kept in mind that sternal foramen may be present, especially in order not to cause iatrogenic thoracic trauma and forensic problems, necessary precautions should be taken beforehand.
References
Aktan ZA, Savas R (1998) Anatomic and HRCT demonstration of midline sternal foramina. Turk J Med Sci 28:511–514
Ashley GT (1956) The relationship between the pattern of ossification and the definitive shape of the mesosternum in man. J Anat 90:87–105
Azizi S, Bakhtiary MK, Goodarzi M (2012) Congenital sternal foramen in a stillborn Holstein calf. Asian Pac J Trop Biomed 2:83–84
Babinski MA, de Lemos L, Babinski MS, Goncalves MV, De Paula RC, Fernandes RM (2015) Frequency of sternal foramen evaluated by MDCT: a minor variation of great relevance. Surg Radiol Anat 37:287–291
Bayarogulları H, Yengil E, Davran R, Aglagul E, Karazincir S, Balcı A (2014) Evaluation of the postnatal development of the sternum and sternal variations using multidetector CT. Diagn Interv Radiol 20(1):82–89
Boruah DK, Prakash A, Yadav RR, Dhingani DD, Achar S, Augustine A, Mahanta K (2016) The safe zone for blinded sternal interventions based on CT evaluation of midline congenital sternal foramina. Skelet Radiol 45:1619–1628
Choi PJ, Iwanaga J, Tubbs RS (2017) A comprehensive review of the sternal foramina and its clinical significance. Cureus 9(12):e1929. https://doi.org/10.7759/cureus.1929(Published online 8 Dec 2017)
El-Busaid H, Kaisha W, Hassanali J, Hassan S, Ogeng'o J, Mandela P (2012) Sternal foramina and variant xiphoid morphology in a Kenyan population. Folia Morphol 71:19–22
Gkantsinikoudis N, Chaniotakis C, Gkasdaris G, Georgiou N, Kapetanakis S (2017) Morphological approach of the sternal foramen: an anatomic study and a short review of the literature. Folia Morphol 76(3):484–490
Gossner J (2013) Relationship of sternal foramina to vital structures of the chest: A computed tomographic study. Anat Res Int 2013:650601. https://doi.org/10.1155/2013/650601(Published online 2 Oct 2013)
Kumarasamy SA, Agrawal R (2011) A large sternal foramen. IJAV 4:195–198
Paraskevas G, Tzika M, Anastasopoulos N, Kitsoulis P, Sofidis G, Natsis K (2015) Sternal foramina: incidence in Greek population, anatomy and clinical considerations. Surg Radiol Anat 37(7):845–851
Paraskevas GK, Tzika M, Natsis K (2016) Double sternal foramina in a dried sternum: a rare normal variant and its radiologic assessment. Surg Radiol Anat 38(8):991–993
Saccheri P, Sabbadini G, Toso F, Travan L (2012) A keyhole-shaped sternal defect in an ancient human skeleton. Surg Radiol Anat 34:965–968
Xie YZ, Wang BJ, Yun JS, Chung GH, Ma ZB, Li XJ et al (2014) Morphology of the human xiphoid process: dissection and radiography of cadavers and MDCT of patients. Surg Radiol Anat 36(3):209–217
Yekeler E, Tunaci M, Tunaci A, Dursun M, Acunas G (2006) Frequency of sternal variations and anomalies evaluated by MDCT. Am J Roentgenol 186(4):956–960
Funding
The authors received no financial support for the research and/or authorship of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kuzucuoglu, M., Albayrak, I. Topographic evaluation of sternal foramen patients with thoracic computed tomography. Surg Radiol Anat 42, 405–409 (2020). https://doi.org/10.1007/s00276-019-02416-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-019-02416-3