
Abstract
A 67-year-old patient who presented with a right cerebellar hemorrhage underwent vascular workup for suspicion of underlying vascular anomalies. A diagnostic cerebral angiogram demonstrated a duplicated basilar system fed solely by a persistent primitive trigeminal artery. The findings proved to be incidental and unrelated to the patient’s hemorrhage. These developmental abnormalities are consistent with embryological development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During embryonic development, the internal carotid artery (ICA) provides fetal anastomoses to the vertebrobasilar circulations at the 4-mm fetal stage, which include the caudal division of the primitive ICA (the precursor of the posterior communicating artery), trigeminal arteries, otic arteries, hypoglossal arteries, and proatlantal arteries [5]. The primitive trigeminal artery is the most common adult remnant after the posterior communicating artery [6]. It branches from the primitive ICA to join the ipsilateral paired ventral longitudinal neural arterial axis, which will eventually fuse to form the basilar artery [3]. At the 7- to 14-mm fetal stage, the anastomoses remodel, with the trigeminal artery being the last in line of regression [2]. The persistence of this fetal circulation remnant has a reported incidence in the literature of 0.1–1.25 % [1].
The paired ventral longitudinal neural arteries, which initially receive their blood supply from the anterior circulation, coalesce across the midline at the 7- to 12-mm fetal stage, to form the basilar artery. As it loses its anterior input, the posterior circulation proximally anastomoses to the fourth aortic arch, which will subsequently become the subclavian artery [4].
Case report
A 67-year-old female presented to the emergency department with a right cerebellar hemorrhage with associated subarachnoid hemorrhage status post fall, while on warfarin. Due to the atypical location of the bleed, the patient received further neurovascular studies in the form of a computed tomographic angiography (CTA) and a diagnostic cerebral angiogram (DCA). The investigation did not reveal the etiology of the hemorrhage, but it did demonstrate an incidental vascular variant that we have reported here.
Discussion
The first finding that is demonstrated in this patient’s angiography is a failure of regression of the PTA, which normally recedes at 7–14 mm. The second finding is that of a duplicated basilar system adjacent to the basilar artery. This likely occurred at the 7–12 mm embryonic stage, where there was failure of fusion of the ipsilateral longitudinal neural artery. This duplicated basilar is fed solely by the persistent primitive trigeminal artery (PPTA) (Figs. 1, 2, 3).

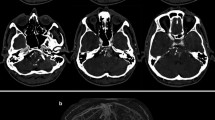
Non-invasive imaging. a CT angiogram reconstruction of the posterior circulation demonstrates the persistent primitive trigeminal artery (solid arrow) feeding the duplicate embryologic basilar system, which parallels the mature basilar artery (arrow head) before ultimately merging (dashed arrow). b T2-weighted magnetic resonance imaging demonstrates the smaller embryologic duplicate basilar system (dashed arrow) paralleling the larger basilar artery (solid arrow)

Diagnostic cerebral angiogram injection of the right internal carotid artery. a The junction of the persistent primitive trigeminal artery and the basilar artery typically occurs in the middle to distal third of basilar, directly into the artery (solid arrow). b In our reported variant, there is a separate ascending channel (arrowhead) running parallel to the mature basilar artery. This fills into the distal portion of the mature basilar artery, as demonstrated by the contrast washout in the vertebrobasilar system (dashed arrow)

Magnified diagnostic cerebral angiogram injections of the a right vertebral artery and the b right internal carotid artery illustrate where the duplicate embryologic basilar system enters the mature basilar artery, as demonstrated by the contrast washout in the vertebrobasilar system (dashed arrow). The solid arrow depicts where a typical persistent trigeminal artery would merge at the mid-basilar trunk
Conclusion
The developmental abnormality visualized here is that of a persistent primitive trigeminal artery in the setting of a failed fusion of the longitudinal arterial plexus. It is important that physicians understand this variation and not confuse it for an aneurysm.
References
Alcalá-Cerra G, Tubbs RS, Niño-Hernández LM (2012) Anatomical features and clinical relevance of a persistent trigeminal artery. Surg Neurol Int 3:111
Bai M, Guo Q, Li S (2013) Persistent trigeminal artery/persistent trigeminal artery variant and coexisting variants of the head and neck vessels diagnosed using 3 T MRA. Clin Radiol 68:e578–e585
Luh GY, Dean BL, Tomsick TA, Wallace RC (1999) The persistent fetal carotid-vertebrobasilar anastomoses. AJR Am J Roentgenol 172:1427–1432
Morris PP (2007) Practical neuroangiography, 2nd edn. Lippincott Williams & Wilkins, Philadelphia, pp 115–124
Uchino A, Saito N, Kurita H et al (2012) Persistent trigeminal artery arising from the arterial ring/fenestration of the cavernous segment of the internal carotid artery. Surg Radiol Anat 34:651–654
Uchino A, Saito N, Okada Y et al (2012) Persistent trigeminal artery and its variants on MR angiography. Surg Radiol Anat 34:271–276
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest concerning the information presented in this paper or the findings specified.
Rights and permissions
About this article

Cite this article
Mohammad, L.M., Carlson, A.P. Unusual persistent primitive trigeminal artery with a superior duplicated basilar system. Surg Radiol Anat 38, 605–607 (2016). https://doi.org/10.1007/s00276-015-1559-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-015-1559-8