
Abstract
The patterns of the feeding vessels to each muscle determine the extent of their safe transposition and the muscle’s value as a pedicled flap in reconstructive surgery. This study aimed to demonstrate the point of origin and the intra- and submuscular course of the pectoral branch of the thoracoacromial trunk (TAT) for pectoralis major (PM) flap surgery. Seventy sides of the PM were dissected based on a clinical reference line that has been used for several decades. The branching point of the TAT from the axillary artery was located lateral to the midclavicular line on the right-sided specimens (100%) and medial to the midclavicular line on the left sides (86%). The branching patterns of the pectoral branch to the PM muscle from the TAT were classified into three types. In type I the pectoral branches originated directly from the TAT (55 cases, 78.6%). In type II (11 cases, 15.7%) and type III (4 cases, 5.7%) the pectoral branch divided from the medial and lateral pedicle of the TAT, respectively. The course of the pectoral branch from the TAT in the PM was categorized into three patterns according to the degree of proximity to the midclavicular line. In 49 cases (70%), the pectoral branch in the PM ran within 1 cm of the midclavicular line. The other cases ran 2 cm (20 cases, 29%) and 3 cm (1 case, 1%) from the midclavicular line, respectively. These results provide topographic data of the pectoral branch based on anatomical landmarks, and will be useful in surgical planning as well as the procedure for PM flap surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The simple anatomy, the ease of harvest, and the proximity of the flap to the head and neck have made the pectoralis major (PM) flap available for the reconstruction of a variety of defects in the head and neck region. Anatomically, the arterial distribution of the PM is supplied by the pectoral branch of the thoracoacromial trunk (TAT), the lateral thoracic artery and the anterior intercostal arteries. In general, the pectoral branches to the PM have been evaluated as the vascular territories of main arterial supply [13]. In particular, Ariyan first described the PM flap based on the pectoral branch of the TAT in 1979 [1]. Its utility in soft tissue reconstructions was quickly recognized, and it has become the “workhorse” flap of the head and neck [4]. The reliability, size, low donor site morbidity and strategic location relative to the head and neck region of PM flaps have made them the reconstructive technique of choice in selected patient populations.
A method for surface marking of the vascular axis for the PM flap was first described by Ariyan [1]. In this surgical technique, the vascular pedicle follows a vertical line drawn down from a point halfway along the clavicle until it meets a line between the acromion and the xiphoid process, along which it then runs in a medial direction. A large number of anatomical studies on the pectoral branch of the TAT have been reported by Freeman et al. [2], Friedrich et al. [3], Moloy et al. [6] and Reid et al. [10]. However, a detailed study aimed at clarifying the Ariyan’s reference line has not been published.
The success of muscle flaps in reconstructive surgery is based on a reliable blood supply. With knowledge of the location and the subsequent preservation of the vascular pedicles to muscles, every muscle may be rotated as a flap. The pattern of the blood supply to each muscle determines the extent of the safe transposition and its value as a flap for coverage in reconstructive surgery.
The aims of this study were to describe and verify the anatomical point of origin and the intramuscular course of the pectoral branch from the TAT, and thereby to provide anatomical guidelines for PM flap design.
Materials and methods
Seventy PM formaldehyde-fixed samples (34 right, 36 left) from 41 Korean adult cadavers (22 men, 19 women; aged 35―88 years) were used in this study.
After dissecting the PM, two reference lines were marked on the specimen using two colored threads: a vertical line at the midpoint of the clavicle and an oblique line from the acromion to the xiphoid process.
The clavicular portion of the PM was detached from the clavicle and the point of origin and branching points of the TAT were identified. The arterial pedicle and branches were dissected proximal to the origin of the TAT from the axillary artery, and the anatomical landmarks of the origin and the course were investigated. After dissecting the arterial pedicle, the branching patterns of the pectoral branch to the PM were classified based on its origin.
Muscular incisions were made to investigate the origin and intramuscular course of the pectoral branches of the TAT. Using a lattice-printed film on the dissected specimens, the courses of the pectoral branches of the TAT were examined and classified according to their proximity to the midclavicular reference line.
Results
All the branches of the TAT originated from the axillary artery and ran laterally 2–3 cm below the clavicle. The point of origin of the TAT from the axillary artery was located lateral to the midclavicular line in the right sides (34 cases, 100%), whereas it was located medial to the midclavicular line in the left sides (31 cases, 86%) (Fig. 1).

Points of origin of the thoracoacromial trunk from the axillary artery
The branching patterns of the pectoral branch to the PM muscle were classified into three categories according to their origin. In 55 specimens, the pectoral branch originated directly from the TAT (type I, 78.6%; 29 right, 26 left). In type II and type III the pectoral branch branched from the medial and lateral pedicle of the TAT, respectively. Types II and III were observed in 11 cases (15.7%; 4 right, 7 left) and four cases (5.7%; 1 right, 3 left), respectively (Fig. 2).

The branching patterns of the pectoral branch to the pectoralis major muscle from the thoracoacromial trunk (TAT; arrow). In type I the pectoral branch originates directly from the trunk of the TAT. In types II and III the pectoral branch splits from the medial and lateral pedicle of the TAT, respectively. PMj, Pectoralis major; PMi, pectoralis minor; P, pectoral branch; C, clavicular branch; A, acromial branch; D, deltoid branch
The intra- and submuscular course of the pectoral branch from the TAT in the PM muscle was identified and classified according to its proximity to the midclavicular line. In 49 specimens (70%; 28 right, 21 left), the pectoral branch from the TAT ran within 1 cm of the midclavicular line. Of the 21 cases on the left side, it ran laterally in three cases and medial to the midclavicular line in 18 cases. Similarly, of 28 cases on the right side, it ran lateral to the midclavicular line in 12 cases and medial in 16 cases.
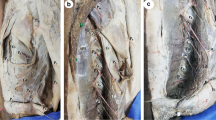
In 20 specimens (29%; 6 right, 14 left), the pectoral branch from the TAT ran 2 cm from the midclavicular line. In 17 cases (5 right, 12 left) the pectoral branch ran medial to the midclavicular line; this was the dominant type. In the other cases (3 cases; 1 right, 2 left), it ran in the lateral aspect. In only one specimen (left side, 1%) it ran 3 cm from the midclavicular line (Fig. 3).

The intra- and submuscular courses of the pectoral branch from the thoracoacromial trunk (TAT) according to its proximity to the midclavicular line. A pectoral branch (arrowheads) from the TAT (arrow) runs to within 1 cm to the midclavicular line, right side (type A); 2 cm from the midclavicular line, right side (type B); and 3 cm from the midclavicular line, left side (type C). PMj, Pectoralis major; PMi, pectoralis minor; P, pectoral branch
Discussion
Surgical treatment of the head and neck area requires extensive resections, necessitating large flaps for reconstruction. In addition, the main prerequisite for the viability of the pedicled flap is a sufficient arterial supply for the transplanted tissue. Therefore, a precise knowledge of the vascular supply to the muscle is necessary to prevent an interruption in the circulation of the muscle. This study investigated the origin and course of the pectoral branch for more reliable and safer clinical planning and application of PM flap surgery.
With knowledge of the location and subsequent preservation of the vascular pedicles to muscles, any muscle may be rotated as a flap. The pattern of the blood supply to each muscle determines the extent of the safe transposition and its worth as a flap for coverage in reconstructive surgery.
The PM is a type V muscle with one major vascular pedicle from the TAT and secondary segmental parasternal perforators. The TAT is accompanied along its course by its corresponding vein, one of the motor nerves to the PM and the lateral pectoral nerve (lateral anterior thoracic nerve) from the brachial plexus [1].
Pandey et al. [9] described the vascular supply to the PM: the superior thoracic artery, the branches from the TAT, the perforating branch of the internal thoracic artery and the pectoral branch of the lateral thoracic artery. According to Manktelow et al. [5] and Wei et al. [11], the two parts of the muscle have a separate neurovascular supply, i.e., a clavicular part which is supplied mainly by branches of the TAT (acromial, deltoid and clavicular), and a sternocostal part supplied mainly by the pectoral branch of the TAT.
Regarding the point of origin of the TAT with reference to the midclavicular line, this study has shown an obvious difference between the right and the left sides. This may be due to the influence of different subclavian arterial systems between the right and the left sides. The right subclavian system branches from the brachiocephalic trunk and the left subclavian system arises from the aortic arch [7]. Therefore, the brachiocephalic trunk exists only on the right side and the presence of the brachiocephalic trunk might influence the position of the axillary artery, indirectly acting as a factor determining the position of the TAT [12].
In this study, we investigated the vascular pattern of the TAT, focusing on the pectoral artery. In 78.6% of cases (type I), the pectoral branch originated directly from the TAT. However, in the cases where the pectoral branch divides from the medial or lateral pedicle of the TAT (types II and III), it is necessary to skeletonize the deltoid or clavicular branch in order to achieve a larger arc of flap.
Reid et al. [10] reported the vascular pattern of the TAT in 50 fixed cadaver dissections. Two main branches (the deltoid and the pectoral arteries) were shown in all cases. The origin of the acromial artery from the deltoid branch was the second most consistent feature. The clavicular artery was most responsible for variation.
In the method for surface marking the vascular axis of the PM flap reported by Ariyan [1], the vascular pedicle follows a line drawn vertically downwards from the midpoint of the clavicle until it meets a line between the acromion and xiphoid process, along which it then runs in a medial direction. In particular, based on the proximity to the midclavicular line, the intra- and submuscular courses of the pectoral branch from the TAT in the PM muscle varied in this study. Nakajima et al. [8] reported the course of the pectoral artery with reference to the median line (axis of sternum). They related the arterial course to the muscular form. Although this study did not investigate the muscle form, the course of the pectoral branch might be related to the PM form as reported by Nakajima et al. [8].
The lateral thoracic artery is not commonly believed to contribute significantly to the vascularity of the PM. However, Freeman et al. [2] and Manktelow et al. [5] reported that the lateral thoracic artery might make an important contribution to the vascular supply of this flap.
In this study, we did not try to clarify the spatial location of the musculocutaneous perforators that supply the skin paddle of a myocutaneous flap. However, we acknowledge that the reliability of the skin paddle over the PM is not simply related to the intra- or submuscular course of the pectoral branch from the TAT but also depends on the spatial distribution of the myocutaneous arterial and venous perforators. In addition, in case of the larger skin paddle of the pectoralis major myocutaneous flap, the survival of the flap can be improved through arterial anastomosis between the pectoral branch and the lateral thoracic artery. Therefore, a future study should aim at investigating the vascular anastomotic pattern within the PM muscle.
Conclusion
This study has shown the difference in the point of origin of the TAT between right and left sides. However, neither the branching pattern nor the intra- and submuscular course of the pectoral branch from the TAT showed any laterality. In addition, although many surgeons have used the reference line reported by Ariyan [1] in PM flap surgery, most pectoral branches (74.3%) ran medial to the midclavicular line. The course and origin of the pectoral branch of the TAT should not significantly influence the useful arch of rotation of the flap. However, it is of help to estimate the course of the vessels when planning the location of the incision during flap surgery. For these reasons, diagnostic tests such as Doppler sonography may be useful in identifying the individual course of the main feeding vessel to the PM in order to reduce the risk of surgical failure.
References
Ariyan S (1979) The pectoralis major myocutaneous flap: a versatile flap for reconstruction in the head and neck. Plast Reconstr Surg 63:73–81
Freeman JL, Walker EP, Wilson JSP, Shaw HJ (1981) The vascular anatomy of the pectoralis major myocutaneous flap. Br J Plast Surg 34:3–10
Friedrich W, Lierse W, Herberhold C (1988) Myocutaneous vascular territory of the thoracoacromial artery. A topographical and morphometric study of the arterial vascularization of the pectoralis major myocutaneous flap. Acta Anat 131:284–291
Liu R, Gullane P, Brown D, Irish J (2001) Pectoralis major myocutaneous pedicled flap in head and neck resection: retrospective review of indications and results in 244 consecutive cases at Toronto General Hospital. J Otolaryngol 30:34–40
Manktelow RT, McKee NH, Vettese T (1980) An anatomical study of the pectoralis major muscle as related to functioning free muscle transplantation. Plast Reconstr Surg 65:610–615
Moloy PJ, Gonzales FE (1986) Vascular anatomy of the pectoralis major myocutaneous flap. Arch Otolaryngol Head Neck Surg 112:66–69
Moore KL (1999) Clinically oriented anatomy, 4th edn. Williams & Wilkins, Baltimore, pp 143–149
Nakajima K, Ide Yu, Abe S, Okada M, Kikuchi A, Ide Yo (1997) Anatomical study of the pectoral branch of thoracoacromial artery. Bull Tokyo Dent Coll 38:207–215
Pandey SK, Tripathi FM, Shukla VK, Tripathi CB, Sonoo J, Shukla CB (1991) Anatomical basis for clinical application of the arterial supply of musculus pectoralis major. Acta Anat 141:302–306
Reid CD, Taylor GI (1984) The vascular territory of the acromiothoracic axis. Br J Plast Surg 37:194–212
Wei WI, Lam KH, Wong J (1984) The true pectoralis major myocutaneous island flap: an anatomical study. Br J Plast Surg 37:568–573
Williams PL, Bannister LH, Berry MB, Collins P, Dyson M, Dussek JE, Ferguson MWJ (1995) Gray’s anatomy, 38th edn. Churchill Livingstone, Baltimore, pp 1537–1538
Yang D, Marshall G, Morris SF (2003) Variability in the vascularity of the pectoralis major muscle. J Otolaryngol 32:12–15
Acknowledgements
This study was supported by a grant of the Korea Health 21 R&D Project, Ministry of Health & Welfare, Republic of Korea (02-PJ1-PG1-CH07–0001). We would like to express our thanks to Ms. Seung Hye Kim, a student at the dental college of Yonsei University, for reviewing this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
H.-D. Park and Y.-S. Min equally contributed to this study
Rights and permissions
About this article
Cite this article
Park, HD., Min, YS., Kwak, HH. et al. Anatomical study concerning the origin and course of the pectoral branch of the thoracoacromial trunk for the pectoralis major flap. Surg Radiol Anat 26, 428–432 (2004). https://doi.org/10.1007/s00276-004-0273-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-004-0273-8