
Abstract
Purpose
The aim of this anatomical study was to describe a local perforator flap, for covering shoulder defects, by determining the features of the acromial branch of the thoraco-acromial artery (abTAA), and the supplied cutaneous area.
Methods
Thirteen fresh cadaveric thoraxes were dissected bilaterally. A precise and reproducible protocol was performed. For each abTAA flap cadaveric dissection, the following parameters were measured after arterial injection: distances between the origin of the perforator artery on the abTAA and the sternum, the acromion, the clavicle, diameter of the perforator artery of the abTAA, length of the perforator pedicle course through major pectoralis muscle, and rotation arc. We also calculated the surface of the injected skin paddle. These measurements were related to morphometric parameters evaluated through the distance between sternum and acromion.
Results
The mean distances measured from the origin of the perforator artery on the abTAA were 14.25 cm to the sternum, 3.45 cm to the acromion, 5.65 cm to the clavicle. The mean diameter of the abTAA was 1.20 mm ± 0.2. The arc of rotation was 180°, and the length of the perforator pedicle could be extended to 7.46 cm ± 1.15. We observed an colored elliptical cutaneous paddle with a longer radius 18 cm and a small radius 15 cm.
Conclusions
Our results suggest that this type of flap could be useful in clinical practice for reconstruction and covering of the acromial area with a thin cutaneous flap with low sequelae on the donor site.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The loss of tissues around the shoulder joint is a surgical emergency. Numerous complications can occur such as infection, injury to the capsule and rotator cuff, early arthritis of the shoulder joint [21]. The loss of substance caused by a trauma, a tumor or an infection in the acromial area, can be a challenge for surgeons. Many reconstruction techniques are possible, all having their respective advantages and disadvantages. The specificity of the shoulder region is its wide mobility range. Each reconstruction technique needs to allow early mobilization to limit stiffness and contracture risks [3]. We can quote numerous flap options to cover defects of shoulder, the most described one being the thoracodorsal flap [8].
Progress in reconstructive surgery has redefined standard procedures. Thanks to Manchot who published his pioneering work describing the arteries of the skin in 1889, the introduction of the perforator flap has extended the reconstruction possibilities [16]. In 1935, Salmon expanded these observations using radiopaque injection studies [24]. Taylor and Palmer published their work defining the vascular territories of source arteries, which they named angiosomes [28]. Koshima and Soeda described perforator flaps in 1989, for limiting the donor-site morbidity and sequelae related to the musculocutaneous flaps [12]. Saint-Cyr et al. depicted the perforasomes of the human body [23].
Nowadays, perforator flaps have become the main reconstructive techniques for restoring defects throughout the body with a reduced donor-site morbidity, an easier covering using thin flaps on the recipient site, a longer pedicle than the one of the parent musculocutaneous flap, and larger possibility for orientation of the pedicle. In addition, aesthetic results are satisfactory. A standardized nomenclature describing all perforator flaps according to the main artery of origin [2, 22] has been agreed on.
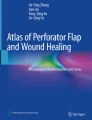
For covering skin and soft tissues defects on the upper part of the shoulder area, translation of the pectoralis major muscle has often been suggested by trauma surgeons, with secondary skin graft. We aimed to search for a possibility of local cutaneous flap and to determine the presence of perforator arteries that could supply it. Three source arteries (thoraco-acromial, intercostal perforators of the internal mammary and terminal branches of the lateral thoracic arteries) supply the major pectoralis (Fig. 1). Variations of the thoraco-acromial artery (TAA) are rare and it commonly arise from the second segment of the axillary artery. It constitutes the major blood supply to the major pectoralis.

An horizontal line was drawn laterally from the sternocostoclavicular joint (S). A vertical was drawn from the anterolateral angle of the acromion (a). A vertical line crossing the horizontal line at the junction two medial thirds/one lateral third showed at the crossing point the localization of the abTAA perforator origin (the green cross)
The aim of this anatomical study was to describe a local perforator flap, for covering shoulder defects, by determining the features the perforator artery originating from the acromial branch of the thoraco-acromial artery (abTAA), and supplying the perforator flap.
Materials and methods
This study was conducted in the Laboratory of Anatomy of the University of Rouen. Dissections were performed by one single operator bilaterally on thirteen fresh cadaveric thoraxes (6 men and 7 women), available according to the rules of the Donation Bodies Program of the Rouen University. Donated bodies with scars in the shoulder region were excluded from the study. The morphometric parameters were measured: a vertical line was drawned from the anterolateral angle of the acromion, and the distance between this line and the clavicular facet of the sternum was measured along a horizontal line (Fig. 1). The study has been divided into three steps, the localization of the perforator artery, the harvesting of the perforator flap, the supplied area of the flap.
First step: the goal was to identify the perforator artery: Ten shoulders were dissected: the bodies were placed in supine position with the arm along the thorax. The clavicular, sternal, and acromial landmarks were labelled with a drawing pencil (Fig. 1). A medial skin incision was made along the sternum lateral border, and the skin and superficial fascia were carefully removed from medial to lateral. We could observe the perforator artery on the ventral surface of the pectoralis major muscle. Then we could follow the perforator artery in the thickness of the pectoralis major muscle (PM), and localize the origin of the vessel. The PM was elevated from medial to lateral, the pectoralis minor muscle was respected, and the thoraco-acromial artery (TAA) was individualized (Fig. 2a, b).
Fig. 2 
a AP-view of the axillary and pectoral regions. The pectoralis major muscle has been removed. The thoraco-acromial artery is exposed with its three branches [pectoral (elevated by the forceps), clavicular and delto-acromial]; b the three branches of the thoraco-acromial artery (TAA) are exposed
Second step: the determination of the perforator flap:
On the 16 remaining shoulders: The abTAA could be found around the point of a vertical line crossing the junction of the two medial thirds and the lateral third of the horizontal drawn line, usually located 7 cm below the clavicle (Fig. 1). A dissection was performed deep to the superficial fascia, starting 4 cm lateral to the sternum and extending to the lateral thorax. Dissection needed to be meticulous around the area of perforator origin on the abTAA. The skin paddle could be raised when the perforating vessels were found (Fig. 3a, b). The pedicle could then be dissected, as proximally as possible, to obtain a longer pedicle length (Fig. 4a, b).
Fig. 3 
a AP-view of the thorax. The skin and superficial fascia are elevated; b the course of the abTAA perforator artery is seen from the pectoralis muscle surface to the skin
Fig. 4 
a The pectoralis major muscle has been fenestrated around the pedicle, and the perforator artery is seen through the muscle; b the length of the complete medical is measured, from the origin to the muscle
Third step: Coloring the skin paddle of the perforator flap: The isolated vascular delto-acromial pedicle needed to be dissected and the deltoid branch of the TAA identified and ligated, for only keeping and inject the acromial branch. Sixty milliliters (ml) of acetone were injected through a catheter placed in the delto-acromial branch, that was used as a chamber of injection (Fig. 5), to wash and dilate the vessels. A waiting period of 24 h was observed before injecting 20 ml of diluted ink solution in the acromial branch of TAA (Colorex; Pebeo, Gemenos, France), and a second 24 h period was needed before observing the coloration of the skin paddle (Fig. 6a, b).
Fig. 5 
60 ml-acetone injection in the acromial branch of the thoraco-acromial artery (TAA). The complete skin of the pectoral and axillary regions and the pectoralis muscle have been resected
Fig. 6 
Selective injection of acromial branch of the TAA with diluted ink solution; a colored skin area photographed at 0 h; b colored skin area photographed after 24 h





Measurements: all the measurements and data collection were performed 24 h after injection, by a single operator. For each abTAA flap cadaveric dissection, the previously measured parameters were controlled: distance between sternum and perforator artery (SP), distance between acromion and perforator artery (AP), distance between clavicle and perforator artery (CP), distance between sternum and acromion (SA), diameter of acromial branch of TAA (D), length of the pedicle through major pectoralis (PM) path (LMP) and radius of the rotation arc (R) that corresponded to the useful length of the pedicle. We also reported and calculated the surface of injected skin area in cm2 (elliptic area = major length × smaller length × π). All data were measured with a centimetric rule (Fig. 6b) except D and LMP for which we used a millimetric caliper (Mitutuyo*) (Fig. 4b).
Results
Data were collected for the twenty-six thorax dissections performed and are compiled in Table 1. During these dissections, the perforator was constantly found.
The origin of the acromial branch was variable, as it could arise from the delto-acromial branch or directly from the TAA. The acromial branch of TAA (abTAA) pierced the PM close to the delto-pectoral groove along a direct linear intramuscular course. The long subcutaneous course allowed an important rotation arc for the perforator flap. This perforator artery originating from the TAA was accompanied by two venae comitantes, which could provide a venous drainage.
The mean distances ± standard deviation was—sternum to the abTAA: 14.25 ± 1.93 cm—acromion to the abTAA: 3.45 ± 1.05 cm—clavicle to the perforator artery: 5.65 ± 0.72 cm—sternum to acromion: 17.7 ± 1.50 cm. The mean diameter of the abTAA was 1.20 ± 0.20 mm, and the length of the pedicle through the PM was 0.97 ± 0.12 cm. The radius of the arc of rotation was 7.46 ± 1.15 cm.
During the injection of the perforator flaps, we observed that an elliptical cutaneous paddle was supplied, with a major length (R) 18 cm and a smaller length (r) 15 cm. The measured colored skin area was (π × R × r) 848.23 cm2.
Discussion
These anatomic dissections aimed to provide possibilities about the different options to cover a post-traumatic shoulder. During our literature researches, we noted that there were limited articles concerning the post-traumatic context. The flaps for the thoracic region were mainly described for covering a loss of substance after cancer [10], hidradenitis suppurativa [6, 8, 18] for the axillary region, wide scar [8, 27], or after a burn [21]. The flaps of the upper thoracic region were mostly described and clinically used for head and neck areas [5, 20, 26].
The thoracodorsal artery (TDA) flap was widely described for the shoulder reconstruction [29] as others myo-cutaneous flaps such as scapular, parascapular, para-umbilical perforator, latissimus dorsi flaps [9, 15, 30] or some free flaps such as superior gluteal artery perforator flap [14].
We wanted to find a more aesthetic and thinner surgical flap option than the myo-cutaneous flap. The perforator concept is focused on the distal circulation which allows to harvest thinner portions of tissue from the conventional donor sites of myocutaneous flaps [11]. Knowledge of perforasomes is useful for a better flap design and clinical use. During the first dissections of our study, we systematically found a perforating artery that arose from the pectoralis major muscle, originating from the thoraco-abdominal artery (TAA) which was found by a deeper dissection.
Only a few articles report about TAA perforator flaps [13], and for the most part they studied the pectoral branch [4] or the clavicular branch for post-fracture loss of the clavicle [25]. Geddes et al., during their anatomical dissection, saw the potential of the delto-acromial branch as they though it be a cutaneous flap [4]. We proceeded to continue their work, as a clear understanding of the vascular anatomy of an individual perforator relative to its vascular territory and flow characteristics determine both flap design and harvesting.
Musculo-cutaneous perforators from the clavicular and deltoid arteries and variable septo-cutaneous vessels from the transverse cervical, suprascapular, and supraclavicular branches of the thyrocervical trunk supply the superior integument of the thorax [7].
Geddes and al. also found that the thoraco-acromial axis consistently gave rise to perforators in the upper portion of the PM muscle, as well as the existence of reliable perforators from the clavicular and deltoid branches of the thoraco-acromial artery [4]. Based on the literature review and clinical experiences, the delto-acromial branch of the TAA is the dominant cutaneous blood supply to the anterior lateral chest wall with its perforasome supplying the anterior shoulder and the lateral infra-clavicular anterior chest skin lying between the nipple and anterior axillary line [17].
The perforator flap we defined confirmed their observations and is interesting for soft tissues defects in the shoulder area because it is a local flap with a rather large skin paddle. The shape of the cutaneous flap can be tailored to the loss of substance, and the flap is thin. It is a reliable cutaneous flap with a favorable color match and robust blood supply with a pedicle that can reliably reach the acromion when it is raised as propeller flap.
Before considering reconstructive surgery, it is better to locate the perforator vessel with an US-doppler because it can exist some vascular variations. The origin of variations in the branching pattern of the upper limb arteries is attributed to defects in the embryonic development.
Therefore, there is no need to have a secondary minor debulking procedure. If the arc of rotation is not sufficient, for example if the soft tissue defect is extended to the posterior face of the shoulder, we can dissect the pedicle without damages and the length of the arc of rotation can be doubled if the dissection is going to the origin of the delto-acromial trunk of the TAA.
Donor sites should be evaluated according to their tissue quality and anticipated donor site morbidity [7]. In this case, donor site needs to be closed by a skin graft. The aesthetic aspect is quite good and less morbid because the skin covering is thin. It is almost identical to the thigh skin used for skin graft.
For women, care must be taken when choosing the skin paddle location to avoid the breast. The healing of the skin graft can create breast asymmetry. In our opinion, the skin paddle is sufficiently important in the lateral area to avoid or limit this complication. No difference between the gender was seen in this limited sample.
Chaput and al. studied venous perforasomes, which represents the skin surface drained by the veins (one or two venae comitantes) associated with a perforating artery. This territory is not quantifiable in an anatomical study because it is a dynamic phenomenon that requires 48–72 h to implement [1].
These anatomical findings are consistent with previous anatomical studies performed by others [4, 19].
Conclusion
Our results suggest that the acromial branch of the TAA perforator is a constant and provide a reliable blood supply to a cutaneous flap. This type of flap could be useful in clinical practice for the reconstruction of the acromial area with a thin flap with low sequelae on the donor site, with a more robust circulation than other regional flaps, because it is a primary perforasome and its relatively long pedicle length.
References
Chaput B, Grolleau JL, Garrido I et al (2017) Delayed procedure in propeller perforator flap: defining the venous perforasome. J Plast Reconstr Aesthet Surg 70:286–289. https://doi.org/10.1016/j.bjps.2016.11.011
Cormack GC, Lamberty BGH (1995) The arterial anatomy of skin flaps. Churchill Livingstone, Edinburgh
Gandolfi S, Auquit-Auckbur I, Poirot Y et al (2018) Focus on anatomical aspects of soft tissue coverage options in elbow reconstruction: an updating review. Surg Radiol Anat. https://doi.org/10.1007/s00276-018-2066-5
Geddes CR, Tang M, Yang D, Morris SF (2003) An assessment of the anatomical basis of the thoracoacromial artery perforator flap. Can J Plast Surg J Can Chir Plast 11:23–27
Hallock GG (2011) The island thoracoacromial artery muscle perforator flap. Ann Plast Surg 66:168–171. https://doi.org/10.1097/SAP.0b013e3181dc83cd
Halmy C, Szetei K, Nádai Z et al (2009) Posterior circumflex humeral artery perforator flap (PCHAP-flap) in axillary scar release. Orv Hetil 150:603–606. https://doi.org/10.1556/OH.2009.28556
Hamdi M, Stillaert FBJL (2010) Pedicled perforator flaps in the trunk. Clin Plast Surg 37(655–665):vii. https://doi.org/10.1016/j.cps.2010.06.004
Haq EU, Javaid RH, Hameed S et al (2015) Thoracodorsal artery perforator flap for upper limb reconstruction. J Ayub Med Coll Abbottabad 27:451–457
Izadi D, Paget JT-EH, Haj-Basheer M, Khan UM (2012) Fasciocutaneous flaps of the subscapular artery axis to reconstruct large extremity defects. J Plast Reconstr Aesthetic Surg 65:1357–1362. https://doi.org/10.1016/j.bjps.2012.04.032
Katsuragi Y, Katagiri H, Nagamatsu S et al (2010) Combined sliding flap using a single perforator enables simple closure of the donor site: a case report. J Plast Reconstr Aesthetic Surg 63:e543–e546. https://doi.org/10.1016/j.bjps.2009.11.017
Kim JT, Kim SW (2015) Perforator flap versus conventional flap. J Korean Med Sci 30:514–522. https://doi.org/10.3346/jkms.2015.30.5.514
Koshima I, Soeda S (1989) Inferior epigastric artery skin flaps without rectus abdominis muscle. Br J Plast Surg 42:645–648
Kosutic D (2010) Use of pectoralis major perforators for local “free-style” perforator flap in axillary reconstruction: a case report. Microsurgery 30:159–162. https://doi.org/10.1002/micr.20711
Lachica RD (2012) Resurfacing a traumatic upper extremity contour deformity: a new application of the free superior gluteal artery perforator flap. Plast Reconstr Surg 129:210e–212e. https://doi.org/10.1097/PRS.0b013e3182365d28
Lee K-T, Mun G-H (2014) A systematic review of functional donor-site morbidity after latissimus dorsi muscle transfer. Plast Reconstr Surg 134:303–314. https://doi.org/10.1097/PRS.0000000000000365
Manchot (2011) Die Hautarterien des menschlichen Körpers: [Reprint of the Original from 1889] (German Edition). EOD Network (May 6, 2011)
Mojallal ABF (2015) Atlas des artères perforantes cutanées du tronc et des membres. Elsevier, Paris
Nail-Barthelemy R, Stroumza N, Qassemyar Q et al (2018) Evaluation of the mobility of the shoulder and quality of life after perforator flaps for recalcitrant axillary hidradenitis. Ann Chir Plast Esthet. https://doi.org/10.1016/j.anplas.2018.01.003
Ooi ASH, Butz DR, Teven CM, Gottlieb LJ (2018) Re-introducing the delto-acromial perforator flap: clinical experience and cadaver dissection. J Plast Reconstr Aesthet Surg 71:402–409. https://doi.org/10.1016/j.bjps.2017.08.029
Qassemyar Q, Havet E, Sinna R (2012) Vascular basis of the facial artery perforator flap: analysis of 101 perforator territories. Plast Reconstr Surg 129:421–429. https://doi.org/10.1097/PRS.0b013e31822b6771
Rout DK, Nayak BB, Choudhury AK, Pati AK (2014) Reconstruction of high voltage electric burn wound with exposed shoulder joint by thoracoacromial artery perforator propeller flap. Indian J Plast Surg Off Publ Assoc Plast Surg India 47:256–258. https://doi.org/10.4103/0970-0358.138971
Saint-Cyr M, Schaverien MV, Rohrich RJ (2009) Perforator flaps: history, controversies, physiology, anatomy, and use in reconstruction. Plast Reconstr Surg 123:132e–145e. https://doi.org/10.1097/PRS.0b013e31819f2c6a
Saint-Cyr M, Wong C, Schaverien M et al (2009) The perforasome theory: vascular anatomy and clinical implications. Plast Reconstr Surg 124:1529–1544. https://doi.org/10.1097/PRS.0b013e3181b98a6c
Salmon M, Taylor GI, Tempest MN (1988) Arteries of the skin, 1st edn. Churchill Livingstone, London
Seikaly H, Moshaver A, Chau J et al (2007) Clavipectoral osteomyocutaneous free flap in oromandibular reconstruction. J Otolaryngol 36:186–190
Song DJ, Li Z, Zhou X et al (2018) Clinical application of modified bilobed chimeric thoracoacromial artery perforator flap for reconstruction of hypopharyngeal defect with anterior neck skin loss. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 53:364–368. https://doi.org/10.3760/cma.j.issn.1673-0860.2018.05.007
Stillaert FB, Casaer B, Roche N et al (2008) The inframammary extending lateral intercostal artery perforator flap for reconstruction of axillary contractures: a case report. J Plast Reconstr Aesthet Surg 61:e7–e11. https://doi.org/10.1016/j.bjps.2008.03.070
Taylor GI (2003) The angiosomes of the body and their supply to perforator flaps. Clin Plast Surg 30(331):342
Turner AJ, Haywood RM (2008) Extending the reach of the thoracodorsal artery perforator flap for coverage of the shoulder. J Plast Reconstr Aesthet Surg 61:989–990. https://doi.org/10.1016/j.bjps.2007.10.073
Yousif NJ, Ye Z, Grunert BK et al (1998) Analysis of the distribution of cutaneous perforators in cutaneous flaps. Plast Reconstr Surg 101:72–84
Author information
Authors and Affiliations
Contributions
ACP: Manuscript writing—Data collection—Data analysis. FD: Protocol development—Data collection—Manuscript editing. IAA: Data management. LG: Data collection. BE: Data collection. AC: Manuscript editing
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Portenard, Ac., Auquit-Auckbur, I., Gardeil, L. et al. Anatomical study of the perforator flap based on the acromial branch of the thoraco-acromial artery (abTAA flap): a cadaveric study. Surg Radiol Anat 41, 1361–1367 (2019). https://doi.org/10.1007/s00276-019-02322-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-019-02322-8