
Abstract
Hepatocellular adenomas (HCAs) are benign liver lesions which may be complicated by spontaneous intratumoral bleeding, with or without rupture into the abdominal cavity, or malignant degeneration. Recent advances in radiological interventional techniques now offer selective transcatheter arterial embolization (TAE) as an alternative approach to surgery as the initial treatment to stop the bleeding or as an elective treatment to reduce the tumor mass of the HCA. Herein, we report our initial experience using TAE in the management of HCA. Five female patients and one male patient presented with spontaneous hemorrhage of HCA. Four patients were initially treated with selective TAE to stop the bleeding. In two patients in whom the bleeding stopped spontaneously, TAE was electively undertaken 1 year after presentation to reduce the tumor mass of HCAs >5 cm. Selective TAE as initial treatment in patients with spontaneous bleeding of HCA with or without rupture is effective and will change the need for urgent laparotomy to control bleeding. Selective TAE may also be used as an elective treatment to reduce the tumor mass of larger HCAs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular adenomas (HCAs) are uncommon benign liver tumors [1, 2] which usually affect woman between 15 and 45 years of age. These lesions may present with complications such as spontaneous intratumoral bleeding with or without hemiperitoneum [3], which can be life-threatening due to massive bleeding [4]. Another complication is the risk of malignant transformation in HCAs, which has led to the advice to resect lesions >5 cm [5, 6].
Several authors have suggested immediate partial liver resection or perihepatic packing as initial treatment in cases of spontaneous bleeding. However, it is known that emergency liver resection is associated with a high morbidity and mortality [3, 7]. In recent years, selective transcatheter arterial embolization (TAE) has been applied as initial treatment in patients presenting with acute bleeding due to trauma or ruptured liver tumors. Selective TAE has also been described as an elective treatment for large HCAs in an attempt to reduce the tumor mass [8].
In this report, we describe six patients who presented with bleeding HCA. The liver bleed was successively treated by selective TEA in four patients. In two patients, who responded to conservative treatment, TAE was used to reduce the tumor mass of HCAs >5 cm.
Case Report
Case 1
A 35-year-old woman presented at a hospital elsewhere with acute onset of right upper abdominal pain combined with abdominal distension, nausea, and vomiting. No abdominal trauma had occurred. She had a history of oral contraceptive (OCC) use for 18 years. The patient was pale and painful, with a blood pressure of 110/70 mm Hg and a pulse rate of 120 beats/min. Hemoglobin (Hb) and hematocrit values were 5.2 mmol/L and 0.24, respectively. Liver function tests showed elevated plasma levels (AST, 11,480 U/L; ALT, 3209 U/L; AF, 202 U/L; LDH, 3191 U/L). Contrast-enhanced computed tomography (CT) showed an inhomogeneous mass with mixed densities in segments 2 and 3 of the liver in conjunction with free fluid with a high density consistent with blood in the abdomen. A presumptive diagnosis of HCA with spontaneous hemorrhage and rupture into the free peritoneal cavity was made. The patient was referred to our institution for further diagnosis and treatment after transfusion of 4 U of red blood cells. Because the patient did not respond to infusion and became hemodynamically instable, TAE was decided on.
TAE was performed under local anesthesia using a femoral approach. Selective diagnostic angiography of the superior mesenteric artery and celiac axis was performed using standard visceral catheters. Multiple vessels supplying the HCA were visualized, originating from the proper hepatic artery as well as the left gastric artery. These branches were subsequently selectively catheterized using a coaxial microcatheter system and the supplying arteries were embolized using platinum embolization coils. Care was taken to preserve gastric vascularisation. A completion angiogram showed complete cessation of blood flow to the HCA.
Liver function tests after TAE improved. Follow-up CT 8 months after embolization showed a mass of 10.4 cm, composed of an organized haematoma in a solid lesion, most likely residual HCA. Because of the persisting mass, the lesion was removed 1 year after initial presentation by resection of segments 2 and 3. Histopathological examination showed a lesion of 6 cm with fragments of HCA with old and recent areas of necrotic liver parenchymal tissue. No complications were encountered postoperatively.
Case 2
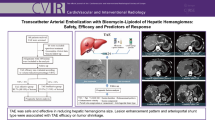
A 42-year-old woman presented with acute onset of abdominal pain in the right upper abdomen and nausea. The patient was known to have used OCC for 20 years. During physical examination, the patient had pain with diffuse tenderness in the right upper abdomen. Laboratory values showed the following abnormalities: Hb, 6.3 mmol/L; AST, 608 U/L; ALT, 1163 U/L; AF, 121 U/L; and GGT, 211 U/L. Abdominal ultrasound (US) showed diffuse fatty changes of the liver and two echogenic lesions in the left liver lobe as well as a subcapsular hematoma in the right liver lobe. Contrast-enhanced CT of the liver showed a hyperdense lesion in segment 6 surrounded by a subcapsular hematoma with hypodense and hyperdense foci. The largest lesion, 5.2 cm, was located in segment 2 with the characteristic enhancement pattern of a HCA (Fig. 1). Because the patient was stable, she was treated conservatively. Follow-up CT 1 year after presentation revealed resorption of the hematoma, but the size of the lesion in the left liver lobe remained unchanged despite cessation of OCC use. In an attempt to reduce the tumor mass of the HCA in the left liver lobe, selective TAE was performed. The HCA was visualized and the supplying branches were selectively catheterized and subsequently embolized using polyvinyl alcohol particles (Ivalon; 300–500 μm) (Figs. 2 and 3). Follow-up CT, 6 months after embolization, showed regression of the lesion in the left liver lobe to 3.7 cm. All other lesions were smaller in size and could be left untreated.

Contrast-enhanced CT of the liver in patient 2 shows a 7-cm enhancing lesion cranially in the right lobe, containing a hypodense area of hemorrhage. A large subcapsular hematoma is seen adjacent to the lesion. In addition, another enhancing mass with a diameter of 5 cm is seen in segment 2 of the left liver lobe

The same patient as in Fig. 1. Selective angiogram with the angiographic catheter positioned in the celiac axis. A microcatheter is advanced through the angiographic catheter into the segment 2 branch of the left hepatic artery. Contrast injection through the microcatheter shows pathological branches and tumor staining of the HCA in the left liver lobe

Selective angiogram of the common hepatic artery in patient 2 shows a large adenoma in the right liver lobe. Pathological branches and splaying of normal branches by the adenoma are observed
Case 3
A 29-year-old woman was admitted to a hospital elsewhere because of acute right upper abdominal pain and nausea. The patient was known to use oral contraceptives. She had pain during physical examination, with diffuse tenderness in the right upper quadrant (blood pressure, 160/90 mmHg; pulse rate, 96 beats/min). Laboratory values were within normal range. CT showed an inhomogeneous mass of 8 cm localized in segment 4 of the liver, with hyperdense areas corresponding with recent hemorrhage. Under the presumptive diagnosis of a bleeding HCA, the patient was referred to our hospital for further treatment. Selective angiography showed a large hypervacular lesion in the left liver lobe. Embolization of the lesion was performed using Gelfoam and platinum embolization coils. Liver function test remained within normal range after the TAE procedure. A control CT 3 months after presentation showed cystic degeneration at the site of the lesion, with a cystic component of 4.4 cm and a lesion compatible with an HCA of 1.8 cm. As there were no complaints, the patient was observed further.
Case 4
A 44-year-old woman presented elsewhere with a 1-day history of abdominal pain in the right upper abdomen. She had a history of OCC use. During physical examination, she was pale and had pain with diffuse tenderness in her right upper abdomen. US showed a large subcapsular hematoma, 18 cm, in the right liver lobe, without signs of rupture to the peritoneal cavity. The patient was referred to our hospital for further diagnosis and management. Besides the subcapsular hematoma in the right liver, multiple intrahepatic hypodense areas were also seen on CT (Fig. 4). An anomalous cluster of blood vessels was detected cranially in the right liver lobe. One vessel ended in a spherical structure showing enhancement during the arterial and venous phase, suggesting contrast extravasation (Fig. 5). The imaging findings were suggestive of hemorrhage of a HCA. Because of decreasing hemoglobin level and an increase in pain, TAE was successfully performed. Follow-up CT 3 months after embolization showed a large hypodense subcapsular fluid collection, 13.5 × 7.7 cm, in the right liver lobe. During the portal phase an inhomogeneous enhancement was seen in segments 5 and 6 and subcapsularly in segment 7. The latter findings were compatible with fragments of HCA. Five months after selective TAE, a right hemihepatectomy was undertaken. On histopathological examination, no certain diagnosis was made because the site of the bleeding only revealed necrosis and fibrosis (Fig. 6).

Contrast-enhanced CT scan of the liver in patient 4 shows a large area of hemorrhage in the right liver lobe as well as a subcapsular hematoma. Posterior to the area of hemorrhage in the liver a hypodense mass is seen, which represents an HCA

Selective angiography showed contrast extravasation at the bleeding focus

Macroscopic cut sections of the resection specimen of patient 4 were inconclusive because of necrosis and fibrosis at the site of the hematoma (arrows)
Case 5
A 45-year-old woman presented elsewhere with a 1-day history of acute abdominal pain in the right upper abdomen radiating to the right shoulder. She had a history of OCC use for a period of 23 years. The patient had pain during physical examination, with diffuse tenderness in the right upper quadrant (blood pressure, 130/77 mmHg;, pulse rate, 76 beats/min). Abdominal US demonstrated a solid mass in segments 5 and 6 of the liver, with hyperdense and hypodense areas, and free peritoneal fluid around the liver. CT showed an inhomogeneous mass of 5.5 cm with hyperdense areas corresponding with hemorrhage. The imaging findings were suggestive of hemorrhage of HCA with rupture to the peritoneal cavity. The patient was referred to our hospital for further management. Because the patient was hemodynamically stable, she was treated conservatively. Follow-up CT 6 months after presentation showed a cluster of hyperdense HCA lesions with inhomogeneous enhancement during the arterial and portal phase located in the right liver lobe. One of these lesions, from which the bleeding originated, showed regression to 3.1 cm. Furthermore, two hypervascular lesions, 1.3 and 5.1 cm, respectively, were seen in the left liver lobe. TAE was performed under local anesthesia using the right femoral approach. Selective diagnostic angiography of the hepatic artery was performed using standard visceral catheters. The left hepatic artery was subsequently selectively catheterized using a coaxial microcatheter system. The HCA in the left liver lobe was embolized using 300- to 500-μm polyvinyl alcohol particles (Ivalon) A completion angiogram showed complete cessation of blood flow to the HCA.
The procedure was uneventful and the patient was discharged from hospital the same day. Follow-up CT 3 months after TAE showed total regression of the lesion in the left liver lobe.
Case 6
A 47-year-old male presented elsewhere with acute abdominal pain in the right upper abdomen radiating to the right shoulder after a fall on his right side. He had a history of anabolic steroid use. Laboratory values showed abnormal liver function tests (AST, 161 U/L; ALT, 242 U/L). Contrast-enhanced CT showed a large subcapsular hematoma in the right liver lobe with free peritoneal fluid around the liver. On arterial images, a small hyperdense area was seen centrally in the liver, probably corresponding with a contrast blush. Also, two large hyperdense areas were seen cranial of the liver. No lesion specific for HCA could be identified because of the extensive bleeding. However, the findings on imaging studies in combination with a history of anabolic steroid use were suggestive for the diagnosis of hemorrhage of HCA with rupture to the peritoneal cavity. The patient was hemodynamically unstable and was therefore referred to our hospital for further management.
Selective angiography of the hepatic artery was performed showing multiple small areas of contrast extravasation in the periphery of the liver, probably the result of disruption of the liver capsule by the large subcapsular hemorrhage. One larger arterial branch showed extravasation more centrally in the right liver lobe and this branch was selectively catheterized with a microcatheter. Subsequently, embolization was performed using four platinum microcoils with a diameter of 3 mm. Postembolization angiography showed cessation of contrast extravasation. Control of the bleed was achieved by supplying coagulation factors and red cell transfusions. Laparotomy was subsequently undertaken for removal of the large, intra-abdominal hematoma. Follow-up CT 4 months after embolization showed a decrease in and organization of the subcapsular hematoma. In segment 8, an inhomogeneous lesion with hypodense and hyperdense areas was seen, presumably a necrotic area at the previous bleeding site. No complications were encountered and the patient was discharged from hospital.
Discussion
In this report, we describe six patients with spontaneous bleeding of focal liver lesions that were highly suspicious of HCA (Table 1) [1, 3, 9–11]. These patients were diagnosed by a hepatobiliary consultation group consisting of experienced hepatopancreaticobiliary (HPB) surgeons, a hepatologist, and HPB radiologists according to certain criteria: typical findings on imaging studies in combination with young age, lack of underlying parenchymal liver disease, and a history of longstanding use of OCC or anabolic steroids. The precise incidence of HCA is unknown but considered very low. The risk of bleeding complications is also difficult to estimate [12]. Remarkably, approximately 65% of patients with HCA who use OCC present with bleeding and rupture, compared to 25% of patients without OCC use [3]. Especially, patients with lesions >5 cm or multiple lesions have a high risk of developing spontaneous bleeding with or without rupture [6]. Another complication described for HCA is the possibility of malignant degeneration to hepatocellular carcinoma (HCC) [5]. It is crucial to differentiate HCA from other liver lesions which may present with hemorrhage, especially HCC. In contrast to patients with bleeding liver tumors in the Western world, bleeding from HCC is the most common cause of fatal hemoperitoneum in the Far East. Patients with bleeding due to HCC usually have a medical history of hepatitis, presence of underlying cirrhosis, and/or elevated plasma levels of AFP [13]. Another benign liver lesion often found in young women is focal nodular hyperplasia (FNH). However, there are few reports of spontaneous bleeding and rupture in FNH [14]. Spontaneous bleeding may also occur in patients with other rare conditions such as giant liver hemangiomas [15], liver metastases [16], and HELLP syndrome, or amyloidosis.
In patients with extensive intrahepatic bleeding or rupture of HCA to the peritoneal cavity, hemodynamic stabilisation and rapid accurate diagnosis are mandatory because of the life-threatening condition. The most rapid imaging method to detect intrahepatic bleeding in liver tumors is abdominal US. HCA appears as a hyperechogenic lesion. It is also useful to visualize free fluid in the peritoneal cavity as a sign of spontaneous rupture of HCA [17]. However, contrast-enhanced CT is more reliable for imaging with which the hematoma is clearly visualized, and the diagnosis of a bleeding tumor is suggested by the presence of hyperdense parts inside a solid lesion that are connected with a subcapsular hematoma [18]. In the case of active bleeding a contrast blush may be seen. According to a recent analysis of patients presenting with spontaneous bleeding of HCA, most patients (41%) are in stable condition on admission and therefore only require observation with intravenous fluid supplementation and, occasionally, red cell transfusion [19, 20]. Some authors have suggested acute partial liver resection as initial treatment in patients with a bleeding HCA. However, this procedure is associated with the high mortality rate of 10% [3]. Another possibility is laparotomy and packing of the ruptured liver or even ligation of the right or left hepatic artery, depending on the location of the bleeding lesion [21].
Owing to advances in radiological interventional techniques, selective arterial embolization has emerged as an alternative approach in patients presenting with bleeding due to HCA [19]. Experience has accumulated with TAE for bleeding caused by liver trauma [22], spontaneous ruptured hepatocellular carcinomas [23], and other bleeding liver tumors [24]. A prerequisite for successful, selective embolization is visualization of the focus of the bleeding or the vessels supplying the lesion [25].
Overall, selective TAE is a safe procedure owing to its minimal invasiveness compared to exploration and surgical treatment. The development of microcatheters has provided useful tools for selective embolization of small supplying arteries. The risk of concomitant ischemic damage of liver parenchyma remains low because of the portal vein tributaries accounting for 70% of the total blood supply to the liver. Preprocedural, elevated liver function tests usually show a return to normal values after TAE, as seen in our patients. Caution is necessary, however, not to compromise branches of the major liver arteries, to avoid unnecessary liver damage. The materials for embolization should be easy to use and capable of occluding the supplying vessel without compromising the flow of the main liver arteries. Materials available for embolization are Gelfoam, steel coils, and polyvinyl alcohol particles. At our institution, Ivalon particles and coils are preferred because of their capacity to occlude small supplying arteries. It is also important to correct any disturbed coagulation of patients prior to TAE for an optimal occluding effect of the embolization particles. Complications of TAE are rare and mostly consist of complications of the angiographic procedure, use of contrast medium, and postembolization syndrome. The latter syndrome consists of pain, nausea, and fever [26] which hardly requires intervention because of its self-limiting character.
In the case of HCAs >5 cm, surgical resection is advised because of the increased risk of intratumoral bleeding and malignant transformation [5, 6]. However, before considering surgical resection the use of OCC should be discontinued in an attempt to reduce the size or to induce complete regression of the lesion [27].
The advice to discontinue OCC use should also be given to all patients who present with a bleeding complication of HCA, even after successful treatment with TAE to stop the bleeding. Observation and regular radiological follow-up are justified in the case of HCA <5 cm. Surgical resection of these lesions is advised when growth progression is noted.
Several reports have focused on the elective use of TAE for HCAs >5 cm with the aim of obliterating the tumor mass by complete cessation of the arterial blood flow [6, 28]. When reduction of size to <5 cm is achieved after embolization, regular observation is justified. We have performed selective TAE within 1 year after presentation in two patients on an elective basis, to accomplish a reduction of tumor size. This approach proved successful in these two patients (nos. 2 and 5). The effectiveness of TAE, however, as elective treatment of large HCAs should be confirmed in larger clinical series.
In conclusion, selective TAE as the initial treatment in unstable patients with spontaneous bleeding of HCA with or without intra-abdominal rupture may reduce the need for urgent laparotomy to control bleeding. This method may also be used electively to reduce the tumor mass of larger HCAs.
References
Little JM, Kenny J, Hollands MJ (1990) Hepatic incidentaloma: a modern problem. World J Surg 14:448–451
Rooks JB, Ory HW, Ishak KG, et al. (1979) Epidemiology of hepatocellular adenoma. The role of oral contraceptive use. JAMA 242:644–648
Shortell CK, Schwartz SI (1991) Hepatic adenoma and focal nodular hyperplasia. Surg Gynecol Obstet 173:426–431
Tao LC (1991) Oral contraceptive-associated liver cell adenoma and hepatocellular carcinoma. Cytomorphology and mechanism of malignant transformation. Cancer 68:341–347
Ault GT, Wren SM, Ralls PW, Reynolds TB, Stain SC (1996) Selective management of hepatic adenomas. Am Surg 62:825–829
Leese T, Farges O, Bismuth H (1988) Liver cell adenomas. A 12-year surgical experience from a specialist hepato-biliary unit. Ann Surg 208:558–564
Flowers BF, McBurney RP, Vera SR (1990) Ruptured hepatic adenoma. A spectrum of presentation and treatment. Am Surg 56:380–383
Huurman VA, Stoot JH, van der Linden E, Terpstra OT, Schaapherder AF (2006) Necrosis of a large hepatic tumor after hemorrhage and subsequent selective arterial embolization. World J Gastroenterol 12(37):6059–6061
Baum JK, Bookstein JJ, Holtz F, Klein EW (1973) Possible association between benign hepatomas and oral contraceptives. Lancet 2:926–929
Soe KL, Soe M, Gluud C (1992) Liver pathology associated with the use of anabolic-androgenic steroids. Liver 12:73–79
Belghiti J, Pateron D, Panis Y, et al. (1993) Resection of presumed benign liver tumours. Br J Surg 80:380–383
Rubin RA, Mitchell DG (1996) Evaluation of the solid hepatic mass. Med Clin North Am 80:907–928
Vergara V, Muratore A, Bouzari H, et al. (2000) Spontaneous rupture of hepatocelluar carcinoma: surgical resection and long-term survival. Eur J Surg Oncol 26:770–772
Rahili A, Cai J, Trastour C, et al. (2005) Spontaneous rupture and hemorrhage of hepatic focal nodular hyperplasia in lobus caudatus. J Hepatobil Pancreat Surg 12:138–142
Corigliano N, Mercantini P, Amodio PM, et al. (2003) Hemoperitoneum from a spontaneous rupture of a giant hemangioma of the liver: report of a case. Surg Today 33:459–463
Murakami R, Taniai N, Kumazaki T, Kobayashi Y, Ogura J, Ichikawa T (2000) Rupture of a hepatic metastasis from renal cell carcinoma. Clin Imaging 24:72–74
Grazioli L, Federle MP, Brancatelli G, Ichikawa T, Olivetti L, Blachar A (2001) Hepatic adenomas: imaging and pathologic findings. Radiographics 21:877–892
Casillas VJ, Amendola MA, Gascue A, Pinnar N, Levi JU, Perez JM (2000) Imaging of nontraumatic hemorrhagic hepatic lesions. Radiographics 20:367–378
Marini P, Vilgrain V, Belghiti J (2002) Management of spontaneous rupture of liver tumours. Dig Surg 19:109–113
Erdogan D, Busch OR, van Delden OM, Ten Kate FJ, Gouma DJ, van Gulik TM (2006) Management of spontaneous haemorrhage and rupture of hepatocellular adenomas. A single centre experience. Liver Int 26:433–438
Lai EC, Wu KM, Choi TK, Fan ST, Wong J (1989) Spontaneous ruptured hepatocellular carcinoma. An appraisal of surgical treatment. Ann Surg 210:24–28
Hagiwara A, Murata A, Matsuda T, Matsuda H, Shimazaki S (2002) The efficacy and limitations of transarterial embolization for severe hepatic injury. J Trauma 52:1091–1096
Liu CL, Fan ST, Lo CM, et al. (2001) Management of spontaneous rupture of hepatocellular carcinoma: single-center experience. J Clin Oncol 19:3725–3732
Murakami R, Taniai N, Kumazaki T, Kobayashi Y, Ogura J, Ichikawa T (2000) Rupture of a hepatic metastasis from renal cell carcinoma. Clin Imaging 24:72–74
Ngan H, Tso WK, Lai CL, Fan ST (1998) The role of hepatic arterial embolization in the treatment of spontaneous rupture of hepatocellular carcinoma. Clin Radiol 53:338–341
Castells L, Moreiras M, Quiroga S, et al. (2001) Hemoperitoneum as a first manifestation of hepatocellular carcinoma in western patients with liver cirrhosis: effectiveness of emergency treatment with transcatheter arterial embolization. Dig Dis Sci 46:555–562
Kawakatsu M, Vilgrain V, Erlinger S, Nahum H (1997) Disappearance of liver cell adenoma: CT and MR imaging. Abdom Imaging 22:274–276
Wheeler PG, Melia W, Dubbins P, et al. (1979) Non-operative arterial embolisation in primary liver tumours. Br Med J 2:242–244
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Erdogan, D., van Delden, O.M., Busch, O.R.C. et al. Selective Transcatheter Arterial Embolization for Treatment of Bleeding Complications or Reduction of Tumor Mass of Hepatocellular Adenomas. Cardiovasc Intervent Radiol 30, 1252–1258 (2007). https://doi.org/10.1007/s00270-007-9108-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-007-9108-4