
Abstract
Background
Vascular complications from intravenous drug abuse pose significant challenges to vascular surgeons. No formalized polices have been reached on surgical management of the resultant infected pseudoaneurysm.
Methods
A retrospective review of all patients who underwent surgery for pseudoaneurysms due to chronic intravenous drug abuse from July 2005 to February 2008 was performed.
Results
A total of 15 patients with infected pseudoaneurysms from chronic intravenous drug abuse were operated on during the study period. The sites of involvement were restricted to the femoral (86.7%) and brachial (13.3%) areas. The drug involved was buprenorphine (Subutex) in all cases. Pain over the limb swelling (100%), pulsatility (60%), and symptoms suggestive of septicemia (46.7%) were the most common symptoms. Staphylococcus aureus was present in 93.3%. Diagnosis was achieved clinically in 26.7%, by duplex ultrasonography in 60.0%, and by computed tomography (CT) angiography in 13.3%. In the two patients with brachial pseudoaneurysms, the brachial artery was ligated in one, and a basilic vein patch was used in the other. In the 13 patients with femoral pseudoaneurysms, the pseudoaneurysm was ligated and excised in 8 (61.5%), and immediate reconstructive bypass surgery was performed in 5 (38.5%). Two patients had critical ischemia after ligation and required reconstructive bypass surgery a few weeks later. Postoperative complications included claudication, digital gangrene, localized wound infection, and rebleeding. There was no associated mortality.
Conclusions
Pseudoaneurysm from intravenous drug abuse continues to pose significant challenges to surgeons worldwide, ranging from an accurate diagnosis to the choice of surgery. The aims of surgery must be to achieve adequate débridement and control infection and hemorrhage. Any associated postoperative complications must be identified and dealt with.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vascular complications from intravenous drug abuse continue to pose a sizeable challenge to vascular surgeons worldwide, with femoral and brachial artery pseudoaneurysms the most commonly reported. The complications of pseudoaneurysms include painful swelling, skin necrosis, septicemia, injuries to adjacent structures, thrombosis, digital embolization, life-threatening hemorrhage, limb loss, and even death [1–3].
Buprenorphine, more commonly known as Subutex (Reckitt Benckiser Pharmaceuticals, Richmond, VA, USA) has been marketed in Singapore since 2002 as an opiate substitute to help heroin addicts wean off their dependence, but it gradually became a favorite among recalcitrant drug addicts. Patients are known to crush the tablets and dissolve the powder before injecting the mixture into themselves. The good intention to help these addicts had unfortunately yielded negative and unexpected results, and they currently account for most of the related vascular complications.
This article seeks to highlight the range of presentations and the outcomes of the surgeries performed for patients with infected pseudoaneurysms from intravenous drug abuse over a 3-year period in a single institution. Our second objective was to suggest an algorithm for the management of pseudoaneurysms from intravenous drug abuse.
Methods
Tan Tock Seng Hospital is a 1300-bed institution in Singapore that provides medical care to more than 1.5 million people. We performed a retrospective review of all patients who underwent surgery for pseudoaneurysms due to chronic intravenous drug abuse from July 2005 to February 2008.
Information recorded for each patient included age, sex, presenting signs and symptoms, hematologic investigations, microbiologic results, diagnostic modality, operative details, outcome of surgery, and postoperative complications.
All patients were started on intravenous broad-spectrum antibiotics, and operative treatment was performed in the emergency theater by the vascular surgeons in the institution. These patients were also counseled by our in-house psychiatrists during their stay so that appropriate management could be implemented. Subsequent arrangements were also made to introduce them to the community addiction management programme, which is conducted and monitored by the Institution of Mental Health, Singapore.
Results
During the study period, 15 patients with infected pseudoaneurysms from chronic intravenous drug abuse underwent surgery. The majority were male (93.3%), and of Malay ethnicity (53.3%). The median age was 43 years (25–58 years). The sites of involvement were restricted to the femoral (86.7%) and brachial (13.3%) areas, with 8 (53.3%) being on the right and 7 (46.7%) on the left. The drug abused was buprenorphine (Subutex) in all cases. Table 1 shows the characteristics of these 15 patients.
Pain over the limb swelling was the most common finding and was reported in all cases (Fig. 1). Other symptoms included a pulsatile mass (60.0%), symptoms of septicemia (46.7%) (e.g., fever, chills, rigors), and a purulent discharge (13.3%). Bleeding was present in five (33.3%) patients, and one of them was hypotensive in the emergency department and had to be brought immediately to the operating theater for surgery. The remaining 14 patients were sent to the operating theater only after being further evaluated in the general ward. All patients were operated on within 48 hours of admission, with or without further investigations. Eleven (73.3%) patients had anemia, and almost all (93.3%) had leukocytosis. Table 2 shows the various symptoms and signs in these patients.

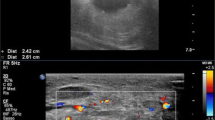
Patient with a right brachial artery pseudoaneurysm
Diagnosis was achieved via duplex ultrasonography (n = 9, 60.0%), computed tomography (CT) angiography (n = 2, 13.3%) (Fig. 2), and clinically in the rest (26.7%) (Table 3). Microbiologic study was performed for all patients during the surgery. Staphylococcus aureus was present in 93.3%, with two being methicillin-resistant. Some of the other bacteria cultured included Streptococcus, Corynebacterium, and Enterobacter.

Computed tomography angiography image of a patient with a left femoral pseudoaneurysm
Of the two patients with brachial artery pseudoaneurysms, one underwent ligation and the other had a vein patch taken from the basilic vein. Both were discharged well with no postoperative complications. For the remaining 13 femoral pseudoaneurysms, ligation and excision of the pseudoaneurysm was performed in 8 (61.5%), and immediate reconstructive bypass surgery was performed in 5 (38.5%).
For the eight patients, simultaneous ligation of the common (CFA) and superficial (SFA) femoral artery and the profunda femoris was performed in six, one had ligation of the CFA and SFA, and the other had ligation only of the SFA. Two of the above patients were readmitted a few weeks later with signs and symptoms of critical limb ischemia; bypass surgery from the external iliac artery (EIA) to the distal SFA using polytetrafluoroethylene (PTFE) graft was performed immediately.
Immediate reconstructive surgery using PTFE grafts were used in the other five patients during the first surgery. All were anastomosed from the EIA to the distal SFA through the obturator foramen. Unfortunately, in one patient the graft became infected from further intravenous drug abuse after discharge and was removed 1 year later. Critical ischemia of the limb ensued several weeks later for which bypass surgery from the common iliac artery (CIA) to the tibioperoneal (TP) trunk was again performed. Table 4 highlights the surgeries undertaken.
Postoperatively, six patients were asymptomatic, eight patients complained of occasional claudication pain, one had a Ray amputation of the fifth toe after the patient complained of duskiness and purulent discharge from the toe a few weeks after the surgery, three had evidence of localized wound infection, and one had significant postoperatively rebleeding, for which further surgery was necessary.
There was no associated mortality in this series, and all were discharged with a viable limb. The median length of stay was 10 days (range 3–107 days). The only patient who stayed for more than 3 months had associated cervical osteomyelitis and an epidural abscess, necessitating long-term antibiotics and rehabilitation.
Only 8 (53.3%) of the 15 patients attended our follow-up clinic after discharge. Half of them underwent simple ligation and excision of the pseudoaneurysm, and only one of them complained of claudication; none require further surgery. The other half, who underwent immediate or delayed vascular reconstruction, had no significant complaints. Unfortunately, the median follow-up was only 6 months (range 1–20 months).
Discussion
Pseudoaneurysm occurs as a result of inadvertent intraarterial or periarterial injection of habitual drugs, with the femoral artery and brachial artery the most commonly involved. Extravasation of blood and contamination of the subsequent hematoma result in the erosion and eventual rupture of the vessel wall, with the formation of an infected pseudoaneurysm [1, 2]. Hemorrhage could ensue if the condition deteriorates, as seen in 33.3% of our patients.
Apart from bleeding, symptoms and signs of systemic infection (including fever, leukocytosis, bacteremia) and even sepsis often accompany the painful pulsatile limb swelling, similar to patients in our series [3]. Pus, blood, and a pulsatile mass have been described by some as the unforgettable triad of an infected pseudoaneurysm [2]. If left untreated, it can lead to systemic sepsis, life-threatening hemorrhage, limb loss, and even death. Apart from the pseudoaneurysm and its infective complications, intravenous drug abuse results in many other complications, such as infective endocarditis, venous obstruction, and insufficiency [3].
Hence, any patient with a history of previous attempted intravenous injection into the groin or cubital fossa who presents with a painful mass in these areas must be suspected of harboring an infected pseudoaneurysm [1]. These patients typically present in one of two possible scenarios. First, they might present to the emergency department with massive bleeding from a cubital or groin pulsatile mass, with or without circulatory collapse. As with all standard resuscitative protocols, securing the airway of patients in circulatory collapse is imperative. Immediate life-saving surgery and aggressive volume replacement using blood products and crystalloid/colloidal solutions are also crucial. Intravenous broad-spectrum antibiotics and universal contact precautions must be adopted in these high-risk patients. During the surgery, after securing the inflow and outflow of the pseudoaneurysm, its simple ligation is suggested to allow continual resuscitation in the surgical intensive care unit.
For the other group of patients who do not require immediate surgery, clinical differentiating a pseudoaneurysm from an abscess is of paramount importance as an erroneous diagnosis could lead to significant hemorrhage. This situation may be encountered by any physician, whether based in rural health institutions or tertiary centers. An in-depth history and thorough physical examination may just be adequate to achieve the diagnosis, as shown in 26.7% of our patients, especially if these patients presented with the typical features of a pulsatile limb mass with surrounding erythema, induration, or significant hemorrhage from the swelling. The history of intravenous drug abuse should always be obtained. However, when diagnosis is uncertain, using the available diagnostic modalities is suggested.
The authors proposed use of duplex ultrasonography (US) in these circumstances. It has been shown to be extremely helpful and accurate for confirming the diagnosis [4]. It could also screen the deep veins for associated thrombosis and occlusion. Furthermore, it can help distinguish a localized abscess, cellulitis, and venous thrombosis from a pseudoaneurysm. Should a pseudoaneurysm be present, bidirectional blood flow in the tract connecting the cavity and the involved artery (neck of the aneurysm) can be identified. However, duplex US often fails to detect the presence or extent of infection; moreover, it is not always reliable for defining the inflow anatomy and a compromised adjacent vessel.
Invasive angiography has long been the method of choice for evaluating pseudoaneurysms [5]; but because of its numerous complications, its role has diminished with the increased utilization, technologic advancement, and expertise of duplex US and CT scans.
Computed tomograpy angiography has been deemed by some authors to be the most reliable study for assessing pseudoaneurysms. It allows accurate definition of the arterial anatomy, including the location of the pseudoaneurysm. Moreover, involvement of the branch vessels, the anatomy of the surrounding structures, the presence of anatomic variants, and the arterial supply to the distal extremity can also be clearly delineated [6]. Blood flow or leakage can also be seen; and an abscess containing gas is easily differentiated from a hematoma. The issues of radiation exposure and intravenous contrast are the major drawbacks.
Intravenous broad-spectrum antibiotics must be commenced upon admission to cover the numerous associated bacteria. Staphylococcus aureus, either sensitive or resistant to methicillin, is the most commonly cultured organism detected in these patients worldwide, including our series [7]. Other gram-positive and gram-negative species are also not uncommon. Cultures should be repeated at short intervals to optimize antimicrobial use and determine the duration of treatment. Screening for communicable disease such as hepatitis B and C, and human immunodeficiency virus (HIV) should always be considered in these high-risk patients. Hence, universal blood precaution is extremely important to protect all involved.
Conservative treatment of infected pseudoaneurysm is rarely an option, as these lesions do not heal; and there are serious complications, such as life-threatening hemorrhage from rupture and septicemia [8]. Surgical treatment is aimed toward controlling infection, adequate débridement of all necrotic tissue, cessation of hemorrhage, and preservation of distal circulation.
The surgical options are still controversial, with no formalized policy adopted worldwide [9, 10]. They range from primary amputation, primary repair with extensive local débridement, ligation and excision of the pseudoaneurysm with or without early arterial revascularization, and ligation and excision of the pseudoaneurysm with immediate arterial revascularization using either vein or prosthetic graft. Primary amputation may be inevitable if the affected limb is nonviable. The presence of extensive tissue necrosis or necrotizing fasciitis is a contraindication to any attempt at revascularization. Primary repair of the pseudoaneurysm after extensive local debridement is also not recommended by the authors as the risk of secondary hemorrhage and infection is considerable.
Ligation and excision of the pseudoaneurysm with thorough débridement without immediate revascularization was performed in 61.5% of our patients. This strategy avoids the significant morbidity and occasional mortality of aggressive simultaneous arterial revascularization. In addition, the procedure is technically less challenging and faster; it also offers definitive control of the bleeding and is unlikely to lead to major tissue loss [11, 12]. However, complications such as critical ischemia and amputation have been widely reported [2, 11, 12] and were also seen in several of our patients, two whom required subsequent bypass surgery. The severity of claudication corresponds to the number of vessels ligated.
There has been a huge variation among reports regarding the incidence of severe claudication after triple ligation, ranging from 33% to 100% [8, 13, 14], while the amputation rate ranged from 6.5% to 35.0% [10]. There has been no reliable method to predict which patient would require revascularization after ligation and excision of the pseudoaneurysm. Apart from palpable pulse(s), a positive Doppler signal is suggestive of adequate distal perfusion, but this is not foolproof. The absence of pulse or a positive Doppler signal does not necessitate immediate amputation as the presence of collaterals is not uncommon in these patients. Hence, vigilant postoperative monitoring and intervention is crucial. Furthermore, fasciotomy should be considered early to prevent compartment syndrome and possible limb loss in these patients.
Delayed revascularization after ligation and excision has been proposed to reduce the risk of limb loss. The main aim is to identify limbs at risk of critical ischemia early and intervene surgically after initially ligating and excising the pseudoaneurysm. Determining the critical point is of paramount importance, as a delayed diagnosis may result in irreversible ischemia. Recognition of ischemia during the first 6 hours either clinically or using Doppler signals is vital. Delay of more than 6 hours has been associated with a worse outcome [15].
Immediate vascular reconstruction during the initial surgery is another option that has been often described in the literature [16, 17]. Although the option of creating a conduit in an anatomically sterile field is attractive, there are numerous considerations. Vein grafts are deemed the most suitable, but more often than not, irreversible damage to the veins from previous direct injections and thrombosis makes them unsuitable. Moreover, the veins may not be of suitable caliber for reconstruction of more proximal arterial segments.
The absence of a suitable vein graft makes the use of a prosthetic graft inevitable. However the major drawback is the significant higher risk of reinfection, bacteremia, and even life-threatening hemorrhage if these patients use the prosthetic grafts as a route for injection [16, 17]. Even if the extraanatomic bypass grafts avoided the contaminated field, either through the lateral thigh or the obturator route, the incidence of graft infection, thrombosis, and amputation remains high [16, 17]. Five immediate extraanatomical bypass surgeries were performed in our series, and one subsequently presented with graft infection, necessitating its removal.
The present study has several limitations as all patients were enrolled from a single institution and the data were reviewed retrospectively. The high proportion of patients who were lost to follow-up also affected our findings, but this is not unexpected or preventable. In addition, there was no previous fixed protocol adopted in our institution for managing these patients. This has already been changed. We have adopted the algorithm shown in Fig. 3. Primary ligation and excision of the pseudoaneurysm has become the surgery of choice in our institution because of the numerous advantages discussed above. However, extreme vigilance is emphasized to identify those patients with critical ischemia, and early vascular reconstruction within 6 hours is recommended. Immediate vascular reconstruction is performed only if there is early intraoperative evidence of critical ischemia.

Suggested algorithm for management of pseudoaneurysms due to intravenous drug abuse. U/S: ultrasonography; CT: computed tomography < PRODUCTION > Note that this algorithm was in the pdf file but not in the manuscript file
Although these limitations are significant, this study is important for highlighting the issues surrounding infective pseudoaneurysms in intravenous drug abusers. We have also suggested a simple algorithm based on the results from the literature for all physicians, especially as it is unlikely that any large prospective trials with long-term follow-up can be conducted.
In addition, this study is one of the largest in the literature evaluating surgical management following intravenous abuse of buprenorphine. The introduction of buprenorphine is an example of good intention that has led to unintended detrimental outcomes [18]. The good intention to help heroin addicts had unfortunately yielded negative and unexpected results, with vascular and lethal complications commonly mentioned [19]. Should the respective health authorities neglect the potential harm of buprenorphine, complications from its abuse will definitely increase and pose a new problem for health care workers. Strict rules and regulations must be enforced to minimize this potential abuse.
Conclusion
Pseudoaneurysms from intravenous drug abuse continue to pose significant challenges to surgeons worldwide, ranging from accurate diagnosis to the choice of surgery. Even though every surgical modality is associated with numerous limitations, the aims of surgery must be to achieve adequate débridement and control infection and hemorrhage. Heightened awareness must be emphasized to detect any associated complications early and to institute appropriate treatment.
References
Welch GH, Reid DB, Pollock JG (1990) Infected false aneurysms in the groin of intravenous drug abusers. Br J Surg 77:330–333
Ting AC, Cheng SW (1997) Femoral pseudoaneurysms in drug addicts. World J Surg 21:783–786
Anderson CB, Butcher HR, Ballinger WF (1974) Mycotic aneurysm of the drug addict. Arch Surg 109:712–717
Sandler MA, Alpern MB, Madrazo BL et al (1984) Inflammatory lesions of the groin: ultrasonic evaluation. Radiology 151:747–750
Shetty PC, Krasicky GA, Sharma RP et al (1985) Mycotic aneurysms in intravenous drug abusers: the utility of intravenous digital subtraction angiography. Radiology 155:319–321
Tsao JW, Marder SR, Goldstone J et al (2002) Presentation, diagnosis, and management of arterial mycotic pseudoaneurysms in injection drug users. Ann Vasc Surg 16:652–662
Behera A, Menakuru SR, Jindal R (2003) Vascular complications of drug abuse: an Indian experience. ANZ J Surg 73:1004–1007
Gan JP, Leiberman DP, Pollock JG (2000) Outcome after ligation of infected false femoral aneurysms in intravenous drug abusers. Eur J Vasc Endovasc Surg 19:158–161
Padberg F Jr, Hobson R, Bing L et al (1992) Femoral pseudoaneurysm from drugs of abuse: ligation or reconstruction? J Vasc Surg 15:642–648
Georgiadis GS, Lazarides MK, Polychronidis A et al (2005) Surgical treatment of femoral artery infected false aneurysms in drug abusers. ANZ J Surg 75:1005–1010
Arora S, Weber MA, Fox CJ et al (2001) Common femoral artery ligation and local debridement: a safe treatment for infected femoral artery pseudoaneurysms. J Vasc Surg 33:990–993
Naqi SA, Khan HM, Akhtar S et al (2006) Femoral pseudoaneurysm in drug addicts–excision without revascularization is a viable option. Eur J Vasc Endovasc Surg 31:585–587
Reddy DJ, Smith RF, Elliot JP et al (1986) Infected femoral artery false aneurysms in drug addicts: evolution of selective vascular reconstruction. J Vasc Surg 3:718–724
Cheng SWK, Fok M, Wong J (1992) Infected femoral pseudoaneurysm in intravenous drug abusers. Br J Surg 79:510–512
Benitez PR, Newell MA (1986) Vascular trauma in drug abuse: patterns of injury. Ann Vasc Surg 1:175–181
Yegane RA, Salehi NA, Ghaseminegad A et al (2006) Surgical approach to vascular complications of intravenous drug abuse. Eur J Vasc Endovasc Surg 32:397–401
Patel KR, Semel L, Clauss RH (1988) Routine revascularisation with resection of infected femoral pseudoaneurysms from substance abuse. J Vasc Surg 8:321–328
Lee CE (2006) Tackling Subutex abuse in Singapore. Singapore Med J 47:919–921
Tracqui A, Kintz P, Ludes B (1998) Buprenorphine-related deaths among drug addicts in France: a report on 20 fatalities. J Anal Toxicol 22:430–434
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tan, KK., Chen, K., Chia, KH. et al. Surgical Management of Infected Pseudoaneurysms in Intravenous Drug Abusers: Single Institution Experience and a Proposed Algorithm. World J Surg 33, 1830–1835 (2009). https://doi.org/10.1007/s00268-009-0123-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0123-2