
Abstract
Purpose
Explore the application of endovascular covered stent-graft (SG) placement in femoral pseudoaneurysms in intravenous drug addicts.
Materials and Methods
We evaluated a consecutive series of pseudoaneurysm in intravenous drug addicts treated with SGs from August 2010 to December 2013.
Results
15 patients with 16 arterial pseudoaneurysms were enrolled in this study. All were males with a mean age of 36.9 years. Hemorrhage was the most common reason (93.8 %) for seeking medical care, and 3 of these patients were in hemorrhagic shock at admission. All patients received broad-spectrum antibiotics, and debridement and drainage were implemented after SG placement. 7 of the 13 cases which had microbiologic results showed mixed infections, while gram-negative bacteria were the major pathogens. Except for 2 patients, who were lost to follow-up, two new pseudoaneurysms formed due to delayed debridement, and one stent thrombosis occurred, none of the remaining cases had SG infection or developed claudication.
Conclusions
SG placement controls massive hemorrhage rapidly, gives enough time for subsequent treatment for pseudoaneurysms due to intravenous drug abuse, and reduces the incidence of postoperative claudication. With appropriate broad-spectrum antibiotics and early debridement, the incidence of SG infection is relatively low. It is an effective alternative especially as temporary bridge measure for critical patients. However, the high cost, uncertain long-term prospects, high demand for medical adherence, and the risk of using the conduits for re-puncture call for a cautious selection of patients. More evidence is required for the application of this treatment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Intravascular injections with drugs are associated with many dangerous and life threatening complications including arterial pseudoaneurysms at the injection site. Arterial pseudoaneurysms are most likely to occur in femoral arteries as the inguinal area is easy to access.
The annual prevalence of arterial pseudoaneurysm in the presenting population was estimated to be 0.03 % [1]. Since pseudoaneurysms due to intravenous drug abuse are relatively rare, the experiences of surgical management remain limited. Ligation alone without revascularization, primary and delayed vascular reconstruction, and revascularization in cases with limb ischemia have been reported. However, none of these techniques have been proved to be safe in terms of overall surgical complications and outcomes [2].
In this study, we present 15 patients with 16 femoral pseudoaneurysms caused by intravascular drug abuse over a 40-month period in a single institution. All had endovascular stent-graft (SG) placement as the primary treatment, although infection, which is always accompanied in pseudoaneurysms under these circumstances, has been considered a contraindication for use of SGs according to traditional view. To the best of our knowledge, this is the first reported series of SG placement in the management for femoral pseudoaneurysms in drug abusers.
Materials and Methods
All patients who were admitted to our hospital from August 2010 to December 2013 and underwent endovascular SG placement for inguinal area pseudoaneurysms due to intravenous drug abuse were enrolled in this retrospective study. Diagnosis was made in regard to the previous history of local injection and the existence of a pulsatile lump at the injection site. Computed tomographic angiography (CTA), ultrasonography, or digital subtraction angiography (DSA) was conducted in all these cases to confirm the diagnosis. Information recorded for each patient included age, sex, presenting signs and symptoms, microbiologic results, antibiotic therapy details, operative details, outcome of surgery, length of stay, and postoperative medication and complications.
All patients received broad-spectrum antibiotics due to the high risk of infection once they were admitted. Secretions from the pseudoaneurysms were obtained during debridement and sent for culture. Blood culture was ordered if the patient got a fever with body temperature over 38.5 °C (101.3 K). Antibiotic regimen was adjusted according to the microbiologic results.
The follow-up was kept on except reaching end points. The end points were set as if (1) the patient died, (2) complications appeared, which required secondary surgical or interventional treatment. Data were collected from both outpatient visits and telephone calls. For all patients attended clinics, color Doppler ultrasound was used to evaluate the SG patency. Frequency and prevalence of the specified variables were then calculated.
Results
Clinical Presentation
15 patients with 16 arterial pseudoaneurysms of the inguinal area due to injection drug abuse were admitted (1 patient came back 24 months later with a new pseudoaneurysm in the contralateral limb for relapse). All patients were male with ages ranging between 25 and 49 years (mean age: 36.9 ± 8.7 years). The right and left lower limbs were affected in 11(68.8 %) and 5 cases (31.2 %), respectively (Table 1).
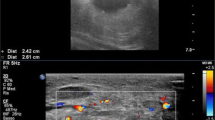
Hemorrhage on account of the ruptured pseudoaneurysms was the most common reason for seeking medical care (15/16, 93.8 %). 13 patients (81.3 %) had a history of bleeding more than once. Three patients went into hemorrhagic shock when admitted to the emergency department, and the lowest hemoglobin level was as low as 51 g/L. Hemorrhage had been temporarily stopped in another 6 cases when they were admitted (Fig. 1).

A CTA-MIP reconstruction showing a pseudoaneurysm located in the right DFA (arrow) near the CFA bifurcation. B CTA transfer scan showing thrombus filling most of the pseudoaneurysm cavity, which breaks through the skin (arrow). C Non-subtracted completion DSA image demonstrating blood flow in the pseudoaneurysm. There is no reconstitution of the DFA distal to the pseudoaneurysm. D Non-subtracted completion DSA image demonstrating successfully excluded pseudoaneurysm and sacrificed DFA
Fever was present in 31.3 % of the patients. Leucocytes and/or neutrophils were increased in 10 cases (62.5 %). Other symptoms or signs such as pain, pulsatile lump, and purulent discharge are also presented in some patients (Table 2).
Ultrasonography was used to diagnose 2 cases (12.5 %) with supplementary non-enhanced CT. Because elastic bandages and multilayer dressing which had been used for compression hemostasia prevented ultrasonography, CTA was performed in 11 cases(68.8 %). 3 patients(18.8 %), who had been in hemorrhagic shock when admitted, had diagnostic DSA directly, followed by SG placement.
These imaging examinations and intraoperative observation showed that 9 cases (56.3 %) had pseudoaneurysms in the common femoral arteries (CFA); 6 cases (37.5 %) were located in the superficial femoral arteries (SFA), and 1 case (6.2 %) was in the deep femoral artery (DFA) (Table 1).
Microbiologic Results and Antibiotic Regimens
Cefuroxime (Zinacef®, GlaxoSmithKline, Brentford, England) was given to the patients once they were admitted during August 2010 to October 2011. Since we had noticed that the antibacterial spectrum of cefuroxime could not cover the pathogens we cultured, we changed initial antibiotic regimen to piperacillin–tazobactam (Tazocin®, Wyeth, New Jersey, USA). Microbiologic studies were done as described above, and the antibiotic regimens were adjusted according to the results.
7 of the 13 patients who had microbiologic results showed mixed infections (1 of the 4 blood-culture-positive patients also had a mixed infection). Gram-negative bacteria were the major pathogens, and Pseudomonas aeruginosa and Acinetobacter baumannii were separately cultured in 5 and 3 cases. Staphylococcus aureus was the most common gram-positive bacteria and present in 4 patients, with 3 of them being methicillin-resistant. Some of the other bacteria cultured included Coagulase negative staphylococcus, Klebsiella pneumoniae, Enterococcus faecalis, Enterobacter cloacae, Streptococcus, Stenotrophomonas maltophilia, Morganella morganii, Candida tropicalis, and Candida glabrada (Table 3).
Except three patients who left hospital without formal discharge, all others received intravenous antibiotics for 12 days to 3 weeks. Oral long-term suppressive antibiotic therapy was case-specific administrated according to the clinical and laboratory parameters of the infection.
Surgical Management
Under local anesthesia, percutaneous accesses to the opposite femoral arteries were achieved by Seldinger technique in 15 cases. Brachial arterial puncture was performed in one patient as a covered stent had been placed in the opposite CFA 2 years earlier. Heparin was administered 50 U/kg of body weight. Covered self-expanding stents (Fluency®, Bard, New Jersey, USA) were delivered via guiding wires to the pseudoaneurysms site and deployed. Completion angiography demonstrated successful exclusion of the pseudoaneurysms in all cases. DFA was sacrificed in 2 cases as the pseudoaneurysms were located very close to the CFA bifurcation (Fig. 1). There were no procedure-related complications.
Debridement and drainage were implemented under local anesthesia 1–2 days following SG placement in most patients. However, there were 2 patients who had delayed debridement and drainage. These two left the hospital without permission after SG placement and came back for medical care 7 days later and received debridement and drainage. 100 mg aspirin per day was continued combining with a 3-month course of 75 mg clopidogrel per day in all cases who had formal discharge.
Follow-up Results
The median length of stay was 16.3 days (range 4–44 days). 3 of them unauthorizedly left hospital without formal discharge. Wound care in the outpatient clinic was still needed in most cases after discharge, and the longest time noted after discharge was 3 months.
13 (81.3 %) of the 15 patients (14 (87.5 %) of the 16 cases) were enrolled in our follow-up. 10 (62.5 %) patients attended our follow-up clinic at least once after discharge. 3 (18.8 %) of them only received telephone follow-up. The rest 2 patients were lost (Table 4). The median follow-up was 13.3 months (range 3–38 months). 8 of the 13 patients were followed for at least 12 months, and 2 patients were over 24 months.
There was no amputation in this series. But these two patients who got delayed debridement and drainage came back to hospital 3 and 4 months later for postoperative rebleeding. CTA revealed no obvious leakage, but enormous hematoma were shown (Fig. 2). Both received surgical exploration during which nearly bare Fluency stents were found with little vascular wall wrapping around them. At the proximal end of the Fluency stent, there was a new pseudoaneurysm filled with thrombus, and there was blood leaking, although this was not demonstrated on the CTA. One of them had common femoral artery ligation then, and the other received open-surgical reconstruction using an 18-cm-long small saphenous vein as an implant.

CTA images in a patient who presented with post-stent-graft placement re-bleeding after 3 months. A 3D reconstruction & B MIP Showing the patency of the stent-graft without conspicuous leakage. C Transverse CTA scan showing thrombus surrounding the patent stent-graft without any apparent contrast extravasation
For the remaining 11 cases who received SG placement, only one patient developed claudication 3 months after the procedure because of stent thrombosis. The other 7 cases which had color doppler ultrasound examinations displayed satisfactory primary SG patency.
Discussion
Femoral artery pseudoaneurysm due to intravascular self-injection is quite rare, but the incidence is higher in the sub-group of patients with a long history of intravenous drug abuse. Due to the fact that pseudoaneurysms in drug addicts are always accompanied by infection, it represents a serious challenge for surgeons to manage them.
Recent advances have made endovascular SG placement as an effective and minimally invasive alternative technique for the treatment of aneurysms. However, placing an endoprosthesis in an infected field is debatable. Semba et al. reported the first cases in which endovascular SGs were used to repair mycotic aneurysms of the thoracic aorta [3]. Since then SGs have been placed to exclude mycotic aneurysms located in carotid artery, coronary artery, and femoral artery [4–8]. Combining with antibiotic therapy, it provided a new treatment modality in critically ill patients at high surgical risk [7] and in emergency situations such as ruptured infected anastomotic femoral artery pseudoaneurysms [9].
The first SG placing in pseudoaneurysm caused by drug abuse was published in 2009 [10]. It was in fact a remedial measure rather than primary intervention. The pseudoaneurysm was first treated by surgical resection followed by vessel reconstruction with autologous material. But a sudden leakage from the vein graft anastomosis with massive bleeding made endovascular SG placement used as bailout.
The first time we used SG for femoral artery pseudoaneurysm in drug user was also for emergency hemostasis. Ligation without arterial revascularization, which is the traditional management, can also achieve fast hemostasis. However, even though the collateral circulations are well opened after ligation, the mean arterial pressure levels of back-flow from the DFA and the SFA are still significantly decreased [11]. It results in a high percentage of claudication and disability (54.4 % in early stage and 44.3 % in late stage [2]), whereas the amputation rate ranges from 5 to 33 % [12–14]. Especially, for pseudoaneurysms involving the common femoral bifurcation, ligation and debridement lead to a much greater risk for limb loss [12, 15]. Thus, arterial reconstruction may be important to improve long-term outcomes [16].
However, immediate revascularization in situ is associated with high complication rates, and the risk of graft infection is still as high as 21.1–32.4 % in spite of using extra-anatomic bypass, which occurs through non-infected tissue planes [2]. Considering the enormous cavity as what has been shown in Fig. 1, surgical arterial reconstruction would be extremely cumbersome.
Exclusion of a ruptured pseudoaneurysm due to drug abuse with SG was therefore considered an appropriate alternative therapeutic option for rapid control of a massive hemorrhage. In addition, effective hemostasis using SG could give enough time for subsequent treatment, especially in these critically ill patients who had been in hemorrhagic shock as shown in our series.
The main concern is the risk of infection in such scenario. Infection that always goes with pseudoaneurysms in drug addicts could be local and systemic. Systemic infection like sepsis also occurred in our series. Staphylococcus 1, either sensitive or resistant to methicillin, is said to be the most commonly cultured organism detected in these patients [17, 18]. But we report a much complicated bacteriologic result. This is probably due to inappropriate antibiotic usage before these patients received formal medical care in China. Mixed and antibiotic-resistant bacterial infection makes it more difficult to manage.
However, it seems that suitable antibiotics for the pathogens are not so important when compared with debridement and drainage. Based on what we learned from our series, early debridement and drainage could greatly reduce the risk of graft infection and lead a favorable result, while delayed debridement with similar antibiotic regimens still leads to continuous damage to the arterial wall, which gives rise to serious postoperative complications, as we described above. Femoral artery is relatively superficial, and this anatomic feature provides a great opportunity for radical debridement and other local measures such as sartorius flaps, antibiotic-loaded polymethylmethacrylate beads, which might further benefit the management of infection [19].
It is much safer to treat SG placement as bridge therapy, particularly given that SG placement reserves the autologous graft resource for subsequent treatment. Second-stage revascularization reduces the risk of complications what occur in immediate revascularization using autologous graft. But there is no published literature providing us experiences in when comes to the end of the bridge therapy. Since there were no signs of graft infection or other complications in most patients, the SG placement was subsequently considered a definitive solution. This policy has been supported by other reports on use of SGs for mycotic pseudoaneurysms [5, 8, 20–22].
However, the patency rate of SG comes to the next focus. Although our series showed comparatively lower rate of postoperative claudication and high short-term patency rate, stent thrombosis did occur in one of our patients. Lupattelli et al. reported one case with acute arterial thrombosis after covered stent exclusion of bleeding mycotic pseudoaneurysm which was treated by catheter-directed thrombolysis later [23]. However, thrombolysis was not suitable for our patient in the settings of old thrombus. The limited follow-up time makes the long-term patency rate unknown. The longest follow-up lasted for 38 months in our series, which is the longest follow-up reported in literature. Hence, reports of long-term success in treating mycotic aneurysms with SGs are not available yet, more evidences especially large prospective trials with long-term follow-up are needed.
The SG type should be taken into account too. We applied nitinol self-expanding stent (Fluency®) in all cases because it was the only SG we had, but it may not be the most preferred option when using proximally to the inguinal ligament or even across the hip joint, as it is relatively prone to kinking and fracture. Other SGs such as the Viabahn® may provide a better option [24].
Although SG placement preserves the opportunity for a secondary arterial reconstruction if complications occur, the unknown long-term patency rate proposes a more careful selection of patients. The DFA was covered in 2 cases for emergency hemostasis. Considering DFA keeps the limb alive when SFA is occluded, it raises the risk of above knee amputation if the SG occludes.
Another aspect is to be mentioned is that intravenous drug abuse is not only a health problem but also a social problem. Except medical factors like infection and long-term patency of the SG, some non-medical factors play important roles in the decision-making process. The obviously higher expense is one of the limitations for SG implantation. Given that this group tends to be notoriously non-compliant with follow-up [2], the possibilities of withdrawing standard treatment midway, not following medical instructions or attending follow-up clinic, give rise to higher risk of postoperative complications. All these are relevant to the fate of the SG. Another vital issue that never can be ignored is recurrent drug dependence which did happen in our series. It may be lethal if using the SG for drug re-injection. Therefore, a more comprehensive assessment, including these non-medical factors, should be made before usage of SG placement, and systemic rehabilitation and appropriate surveillance protocols should be added to the postoperative management.
The limitations of this study include its retrospective and cross-sectional nature, the small number of patients, and the single reconstructive technique as stent placement. Further research is still required for better understanding and management of pseudoaneurysms in drug addicts.
Conclusions
With the ability to conveniently and rapidly control massive hemorrhage, SG placement gives enough time for subsequent treatment of pseudoaneurysms due to intravenous drug abuse. With appropriate broad-spectrum antibiotics and early debridement, the incidence of SG infection is relatively low. It also preserves patency of the affected vessels and therefore reduces the incidence of postoperative claudication. However, considering the high cost, uncertain long-term prospects, strong demand for compliance, and the risk of using the conduits for re-puncture, we suggest that covered SG placement should only be used in selected cases. It is an effective alternative especially as temporary bridge measure for critical patients. But more evidence is required for the application of SG placement as definitive solution. Heightened awareness must be emphasized for early detection of any associated complications, which have yet to be fully understood.
References
Tsao JW, Marder SR, Goldstone J, Bloom AI (2002) Presentation, diagnosis, and management of arterial mycotic pseudoaneurysms in injection drug users. Ann Vasc Surg 16(5):652–662
Georgiadis GS, Lazarides MK, Polychronidis A, Simopoulos C (2005) Surgical treatment of femoral artery infected false aneurysms in drug abusers. ANZ J Surg 75(11):1005–1010
Semba CP, Sakai T, Slonim SM, Razavi MK, Kee ST, Jorgensen MJ, Hagberg RC, Lee GK, Mitchell RS, Miller DC, Dake MD (1998) Mycotic aneurysms of the thoracic aorta: repair with use of endovascular stent-grafts. J Vasc Interv Radiol 9(1 Pt 1):33–40
Schneider PA, Abcarian PW, Leduc JR, Ogawa DY (1998) Stent-graft repair of mycotic superficial femoral artery aneurysm using a Palmaz stent and autologous saphenous vein. Ann Vasc Surg 12(3):282–285
Clarke MG, Thomas HG, Chester JF (2005) MRSA-infected external iliac artery pseudoaneurysm treated with endovascular stenting. Cardiovasc Intervent Radiol 28(3):364–366
Shariff N, Combs W, Roberts J (2009) Large mycotic pseudoaneurysm of the left circumflex treated with antibiotics and covered stent. J Invasive Cardiol 21(2):E37–E38
Wales L, Kruger AJ, Jenkins JS, Mitchell K, Boyne NS, Walker PJ (2010) Mycotic carotid pseudoaneurysm: staged endovascular and surgical repair. Eur J Vasc Endovasc Surg 39(1):23–25
Kwon K, Choi D, Choi SH, Koo BK, Ko YG, Jang Y, Shim WH, Cho SY (2002) Percutaneous stent-graft repair of mycotic common femoral artery aneurysm. J Endovasc Ther 9(5):690–693
Klonaris C, Katsargyris A, Vasileiou I, Markatis F, Liapis CD, Bastounis E (2009) Hybrid repair of ruptured infected anastomotic femoral pseudoaneurysms: Emergent stent-graft implantation and secondary surgical debridement. J Vasc Surg 49(4):938–945
Lupattelli T, Garaci FG, Basile A, Minnella DP, Casini A, Clerissi J (2009) Emergency stent grafting after unsuccessful surgical repair of a mycotic common femoral artery pseudoaneurysm in a drug abuser. Cardiovasc Intervent Radiol 32(2):347–351
Hu ZJ, Wang SM, Li XX, Li SQ, Huang XL (2010) Tolerable hemodynamic changes after femoral artery ligation for the treatment of infected femoral artery pseudoaneurysm. Ann Vasc Surg 24(2):212–218
Naqi SA, Khan HM, Akhtar S, Shah TA (2006) Femoral pseudoaneurysm in drug addicts-excision without revascularization is a viable option. Eur J Vasc Endovasc Surg 31(6):585–587
Salimi J, Shojaeefar A, Khashayar P (2008) Management of infected femoral pseudoaneurysms in intravenous drug abusers: a review of 57 cases. Arch Med Res 39(1):120–124
Mousavi SR, Saberi A, Tadayon N, Zeynalzadeh M, Kavyani A (2010) Femoral artery ligation as treatment for infected pseudo-aneurysms, secondary to drug injection. Acta Chir Belg 110(2):200–202
Patel KR, Semel L, Clauss RH (1989) Routine revascularization with resection of infected femoral pseudoaneurysms from substance abuse. J Vasc Surg 10(3):358
Yegane RA, Salehi NA, Ghaseminegad A, Bahrami F, Bashashati M, Ahmadi M, Hojjati M (2006) Surgical approach to vascular complications of intravenous drug abuse. Eur J Vasc Endovasc Surg 32(4):397–401
Jayaraman S, Richardson D, Conrad M, Eichler C, Schecter W (2012) Mycotic pseudoaneurysms due to injection drug use: a ten-year experience. Ann Vasc Surg 26(6):819–824
Behera A, Menakuru SR, Jindal R (2003) Vascular complications of drug abuse: an Indian experience. ANZ J Surg 73(12):1004–1007
Stone PA, Armstrong PA, Bandyk DF, Brumberg RS, Flaherty SK, Back MR, Johnson BL, Shames ML (2006) Use of antibiotic-loaded polymethylmethacrylate beads for the treatment of extracavitary prosthetic vascular graft infections. J Vasc Surg 44(4):757–761
Callaert JR, Fourneau I, Daenens K, Maleux G, Nevelsteen A (2003) Endoprosthetic treatment of a mycotic superficial femoral artery aneurysm. J Endovasc Ther 10(4):843–845
Sanada J, Matsui O, Arakawa F, Tawara M, Endo T, Ito H, Ushijima S, Endo M, Ikeda M, Miyazu K (2005) Endovascular stent-grafting for infected iliac artery pseudoaneurysms. Cardiovasc Intervent Radiol 28(1):83–86
Mofidi R, Bhat R, Nagy J, Griffiths GD, Chakraverty S (2007) East of Scotland Vascular Network. Endovascular repair of a ruptured mycotic aneurysm of the common iliac artery. Cardiovasc Intervent Radiol 30(5):1029–1032
Palestrant S, Knuttinen MG, Gaba RC, Bui JT, Owens CA (2011) Acute arterial thrombosis after covered stent exclusion of bleeding mycotic pseudoaneurysm: treatment using catheter-directed thrombolysis. Int J Vasc Med 2011:264053
Calligaro KD, Balraj P, Moudgill N, Rao A, Dougherty MJ, Eisenberg J (2013) Results of polytetrafluoroethylene-covered nitinol stents crossing the inguinal ligament. J Vasc Surg 57(2):421–426
Acknowledgments
The study was supported by National Key Clinical Specialties Construction Program of China.
Conflict of interest
The authors had full access to the data and take responsibility for its integrity, read and agree with the manuscript as written, and have no conflict of interest to declare.
Statement of informed consent
No informed consent was obtained for this article because data were analyzed retrospectively and anonymously.
Statement of human and animal rights
Ethical approval is not required for this retrospective study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Fu, Q., Meng, X., Li, F. et al. Stent-Graft Placement with Early Debridement and Antibiotic Treatment for Femoral Pseudoaneurysms in Intravenous Drug Addicts. Cardiovasc Intervent Radiol 38, 565–572 (2015). https://doi.org/10.1007/s00270-014-0994-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-014-0994-y